Congenital Lacrimal Fistula in a Seven-Year-Old Female: A Rare Cause of Epiphora
Praveena Kher1, Jigna Motwani2
1 Professor, Department of Ophthalmology, Datta Meghe Insitute of Medical Sciences, Sawangi, Wardha, Maharashtra, India.
2 Junior Resident, Department of Ophthalmology, Datta Meghe Insitute of Medical Sciences, Sawangi, Wardha, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Jigna Motwani, Junior Resident, Department of Ophthalmology, Jawaharlal Nehru Medical College, 1st Floor, C Block, AVBRH, Sawangi (MEGHE), Wardha, Maharashtra, India.
E-mail: jignamotwani04@gmail.com
Congenital lacrimal fistulas are rare epithelium-lined tracts that tend to have a direct communication between skin and the lacrimal drainage system. These are benign developmental abnormalities, that may require no treatment. This is a rare diagnosis since patients are usually asymptomatic and presents only when epiphora is associated. When symptomatic, congenital lacrimal fistula presents as epiphora, or mucoid discharge, rarely patients could develop nasolacrimal duct obstruction, which may present as recurrent dacryocystitis. Thorough clinical examination is the best way to diagnose the condition, where a fistula ostium may be found inferonasal to medial canthus of the eye. Further, lacrimal probing and irrigation is helpful. Surgical management of the fistula is advised only if the disease is symptomatic which ranges from simple excision to dacryocystorhinostomy. This is a report of one such patient with congenital lacrimal fistula which was treated surgically by fistulectomy.
Embryology, Lacrimal apparatus disease, Surgery
Case Report
A seven-year-old female presented with continuous watering from the left eye, since three months. Her mother, did not give history of redness, swelling or any mucopurulent discharge from the eye. On asking further, the mother revealed presence of an opening in the left lower lid that she observed since birth. There were occasional secretions from the opening that were minimal and hence, neglected by the mother.
There was no history of trauma or previous history of surgery. She was firstborn and birth history was unremarkable. There was no family history of similar condition. The systemic examination was within normal limits.
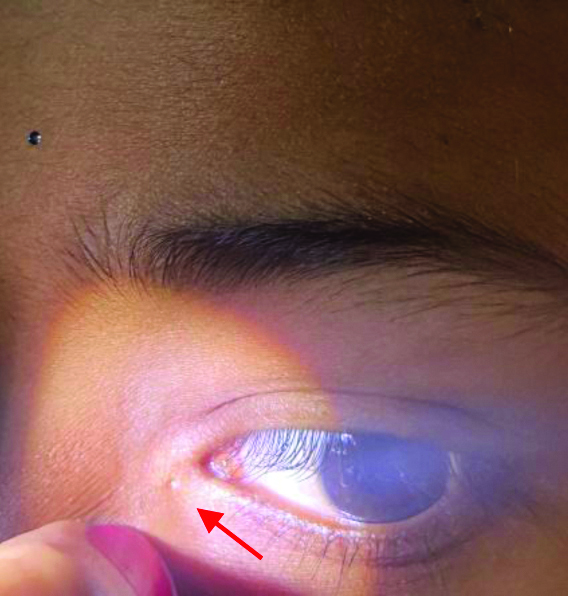
On examination, no facial asymmetry or dysmorphic features were present. The child had no epicanthal folds or mongoloid slant to palpebral fissure, no hypertelorism and no facial clefts. The uncorrected visual acuity was 20/20 in both eyes. Local examination of the left eye revealed a prominent orifice on the inferomedial aspect of medial canthus on inspection [Table/Fig-1]. Both eyelids were normal. On palpation, no swelling was found at the medial canthus of left eye. On applying pressure over lacrimal sac area, there was no reflux of mucopurulent discharge. The rest of the anterior and posterior segment examination of eye was normal. Right eye examination was normal.
The red arrow points at the opening of the lacrimal fistula seen inferonasal to the medial canthus of the left eye.
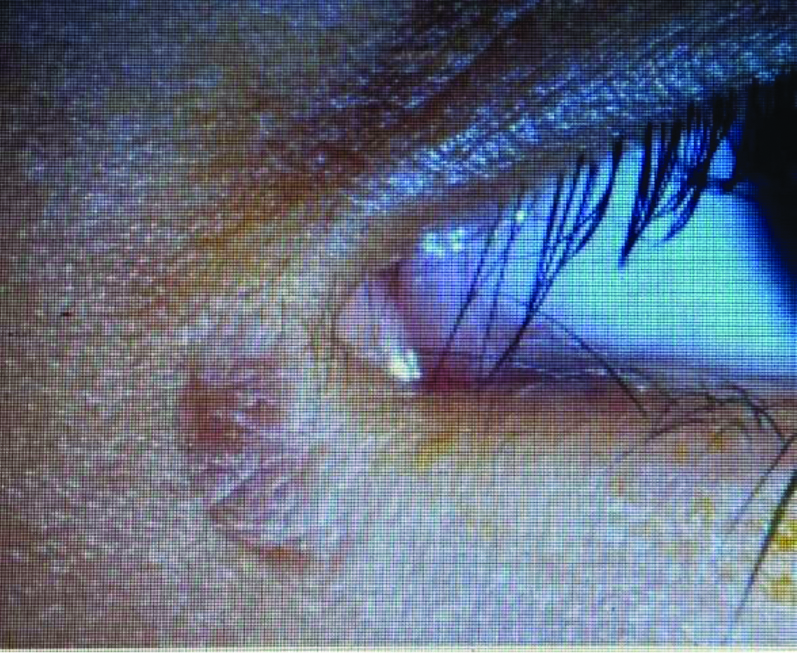
Since the patient was cooperative, lacrimal syringing was performed. Under topical anaesthesia with 0.5% paracaine, with the help of syringe filled with diluted fluorescein dye and lacrimal cannula, the fistula opening at the medial canthal angle was confirmed to have a connection with the lacrimal apparatus of the left eye by the dye visible at the orifice as seen in [Table/Fig-2]. Probe test revealed a fistulous tract going upwards and medially. Other developmental anomalies of the lacrimal tract were ruled out. Nasolacrimal duct was patent. A diagnosis of congenital lacrimal fistula was made. There were no associated congenital anomalies or syndromic features in the patient or presence of other acquired causes.
Reflux of fluorescein dye revealing the fistula ostium.

After ensuring patient cooperation, under local anaesthesia of 2% lignocaine and 0.001% adrenaline with 25% bupivacaine, the surgical procedure was conducted. Probing was done to identify the fistula tract. Incision of about 0.5 cm was taken at the edge of the fistula ostium and dissecting through it, the underlying bone was reached. With simultaneous probing the lacrimal apparatus was identified. After careful dissection of the fistula, it was excised in its whole extent and the wound was carefully sutured with 6-0 vicryl ensuring complete removal of the fistula. Postoperatively, the wound looked healthy.
The patient’s review in the post-surgical period was uneventful. She completed the course of oral and local antibiotics and was asymptomatic one month later. The fistulectomy wound had healed well [Table/Fig-3]. Lacrimal syringing was done on follow-up to rule out any relapses of the condition. There was no recurrence of the fistula. The lacrimal drainage system in the left eye was patent.
Scarred inferonasal area at the medial canthus of the left eye.
Discussion
A congenital lacrimal fistula is a rare developmental anomaly of abnormal canalisation of the lacrimal system forming a connection between skin and the common canaliculus, lacrimal sac or nasolacrimal duct [1]. The incidence of congenital lacrimal fistula is documented as 1 in 2000 births around globe [2,3]. Most cases are unilateral, but some bilateral cases with syndromic or familial association have been reported. Many cases are asymptomatic, but few may present with complaints of tearing from the ostium of the fistula or from the eye [1].
As justified by its aetiopathogenesis, the epithelial lining of lacrimal fistula is found to be stratified squamous epithelium. Congenital lacrimal fistulas may have an association with diseases like Down’s syndrome [4], VACTERL (Vertebral anomalies, Anal atresia, Cardiac malformations, Tracheoesophageal fistula, Renal anomalies, and Limb anomalies) syndrome [5], CHARGE (Coloboma, Heart defect, Atresia choanae, Retarded growth and development, Genital hypoplasia, Ear anomalies/deafness) syndrome [6], ectrodactyly-ectodermal dysplasia-clefting syndrome [7]. Lacrimal fistulas can also be acquired following trauma, nasolacrimal duct obstruction or recurrent acute dacrocystitis. One case report showed its association with Sjogren’s syndrome [8].
Common symptoms for congenital lacrimal fistulas are epiphora from birth or late-onset epiphora, associated tearing from the ostium, blepharitis, nasolacrimal obstruction at the upper duct or sac level giving rise to mucoid discharge following infection [1]. The fistula opening is commonly seen inferonasal to the medial canthal angle [3]. Diagnostic testing frequently involves nasolacrimal probing, irrigation and intubation dacrocystography. Contrast dacrocystography can be done to outline the anatomy of the lacrimal drainage system. Higher investigations like Computed Tomography (CT) may be done. It is important to rule out nasolacrimal duct obstruction in all cases. If symptomatic, congenital lacrimal fistulas can be treated successfully with excision alone. In cases of nasolacrimal duct obstruction, excision with nasolacrimal tract intubation is recommended [9]. Dacryocystorhinostomy can be done only in refractory cases, is the recent school of thought [10]. Congenital lacrimal fistula may show complications related to its syndromic association [11], or a recurrence of the fistula, or persistent epiphora, infections causing persistent discharge, or dacrocystitis.
Conclusion(s)
Congenital lacrimal fistula is one of the rare diagnosis because of its vastly asymptomatic nature. Adequate treatment is essential following diagnosis to prevent complications causing infections of the lacrimal drainage system. Complete removal of the fistula and relieve of symptoms on follow-up should be ensured. The rarity of this case is due to its non-association with any systemic or syndromic anomalies.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jun 06, 2020
Manual Googling: Aug 19, 2020
iThenticate Software: Sep 28, 2020 (5%)
[1]. Chaung JQ, Sundar G, Ali MJ, Congenital lacrimal fistula: A major reviewOrbit 2016 35(4):212-20.10.1080/01676830.2016.117605227191932 [Google Scholar] [CrossRef] [PubMed]
[2]. Welham RA, Bergin DJ, Congenital lacrimal fistulasArch Ophthalmol 1985 103(4):545-48.10.1001/archopht.1985.010500400870253985836 [Google Scholar] [CrossRef] [PubMed]
[3]. Francois J, Bacskulin J, External congenital fistulae of the lacrimal sacOphthalmologica 1969 159:249-26.10.1159/0003059225384317 [Google Scholar] [CrossRef] [PubMed]
[4]. Singh M, Singh U, Bilateral congenital lacrimal fistula in down syndromeMiddle East Afr J Ophthalmol 2013 20:263-64.10.4103/0974-9233.11480724014994 [Google Scholar] [CrossRef] [PubMed]
[5]. Harrison AR, Dailey RA, Wobig JL, Bilateral congenital lacrimal anlage ducts (lacrimal fistula) in a patient with the VACTERL associationOphthal Plast Reconstr Surg 2002 18:149-50.10.1097/00002341-200203000-0001111897957 [Google Scholar] [CrossRef] [PubMed]
[6]. Onaran Z, Yimazbaş P, Ornek K, Bilateral punctum atresia and lacrimal sac fistula in a child with CHARGE syndromeClin Exp Ophthalmol 2009 37(9):894-95.10.1111/j.1442-9071.2009.02187.x20092601 [Google Scholar] [CrossRef] [PubMed]
[7]. Ghosh D, Saha S, Basu SK, Bilateral congenital lacrimal fistulas in an adult as part of ectrodactyly-ectodermal dysplasia-clefting syndrome: A rare anomalyIndian J Ophthalmol 2015 63:800-03.10.4103/0301-4738.17152426655010 [Google Scholar] [CrossRef] [PubMed]
[8]. Ishikawa S, Shoji T, Nishiyama Y, Shinoda K, A case with acquired lacrimal fistula due to Sjögren’s syndromeAmerican Journal of Ophthalmology Case Reports 2019 15:10052610.1016/j.ajoc.2019.10052631388605 [Google Scholar] [CrossRef] [PubMed]
[9]. Birchansky LD, Nerad JA, Kersten RC, Kulwin DR, Management of congenital lacrimal sac fistulaArch Ophthalmol 1990 108(3):388-90.10.1001/archopht.1990.010700500860372310340 [Google Scholar] [CrossRef] [PubMed]
[10]. Al-Salem K, Gibson A, Dolman PJ, Management of congenital lacrimal (anlage) fistulaBritish Journal of Ophthalmology 2014 98:1435-36.10.1136/bjophthalmol-2013-30485424831722 [Google Scholar] [CrossRef] [PubMed]
[11]. Ali MJ, Paulsen F, Syndromic and nonsyndromic systemic associations of congenital lacrimal drainage anomalies: A major reviewOphthalmic Plast Reconstr Surg 2017 33(6):399-407.10.1097/IOP.000000000000092328472008 [Google Scholar] [CrossRef] [PubMed]