Early Childhood Caries (ECC) continues to be one of the most common chronic diseases in children throughout the world, exerting a negative impact on quality of life. This condition can cause pain, infection, and tooth loss as well as problems with speaking, chewing, and nutrition. The aetiology of ECC is complex and involves socioeconomic, biological, and behavioural factors. Rehabilitation in very young patients is challenging due to difficulties inherent to the age of the child, which limits cooperation, the extent of tooth decay, and the motivation of family members, especially in patients with the early loss of primary teeth. Therefore, paediatric dentists need to plan and implement individualised approaches on a case-by-case basis. This paper reports a case of a three-year-old boy diagnosed with ECC involving extensive carious lesions, root remnants, and multiple abscesses. The treatment plan involved prosthetic rehabilitation with complete dentures. Regular check ups were important to the functional adaptations and proper hygiene counselling. The child adapted extremely well to the dentures. Improvements in appearance, speech, and chewing function enhanced the child’s self-confidence and assisted in establishing proper dietary patterns.
Children, Dental caries, Dental prosthesis, Denture, Mouth rehabilitation
Case Report
A three-year-old male child was referred to the Paediatric Dentistry Department of the Lutheran University of Brazil with a chief complaint of continuous pain and swelling of the face lasting one week. The mother reported that the child had been taking antibiotics for five days with no improvement. No significant medical history was reported and the patient was an only child. The mother also reported having sought dental care at a primary care unit, where a panoramic radiograph was requested, but the problem was not treated because the service did not offer dental treatment for young children.
The mother reported that the child had free access to cariogenic foods, breastfeeding upon demand, and frequent use of bottles containing sweetened liquids since the age of six months. Due to the deficient feeding pattern and dental pain, the patient was anaemic and had suffered weight loss.
The extraoral examination revealed swelling on the left side of the submandibular region, which was red in color. On palpation, swelling was hard in consistency and tenderness was present. Swelling was associated with pain, which was spontaneous in nature and did not get relieved after use of analgesics. For the intraoral examination, protective stabilisation performed by the mother was necessary due to the child’s uncooperative behaviour.
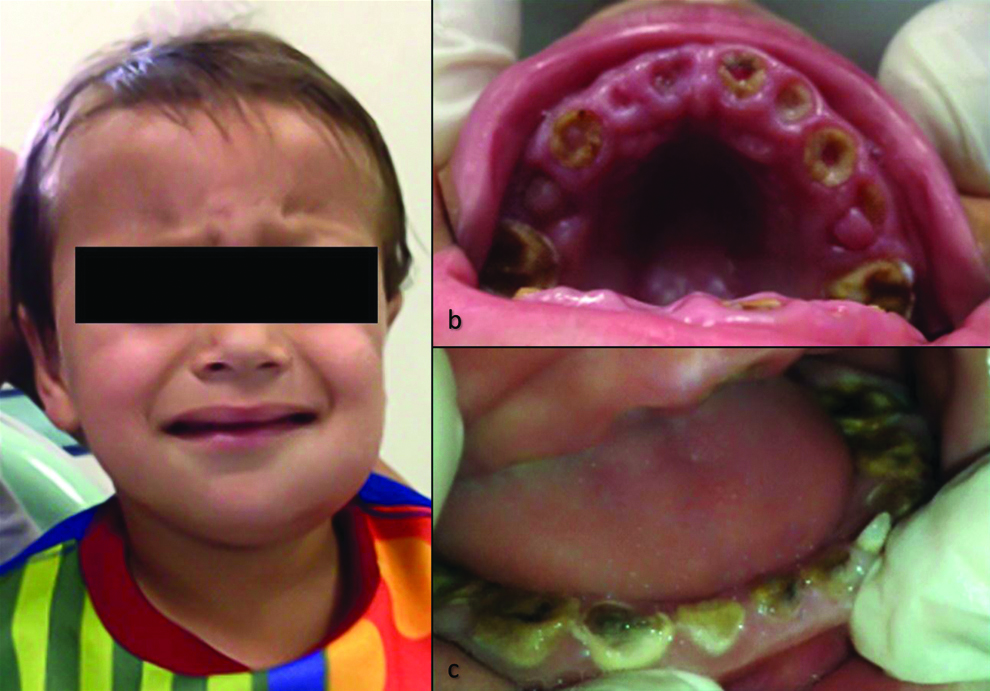
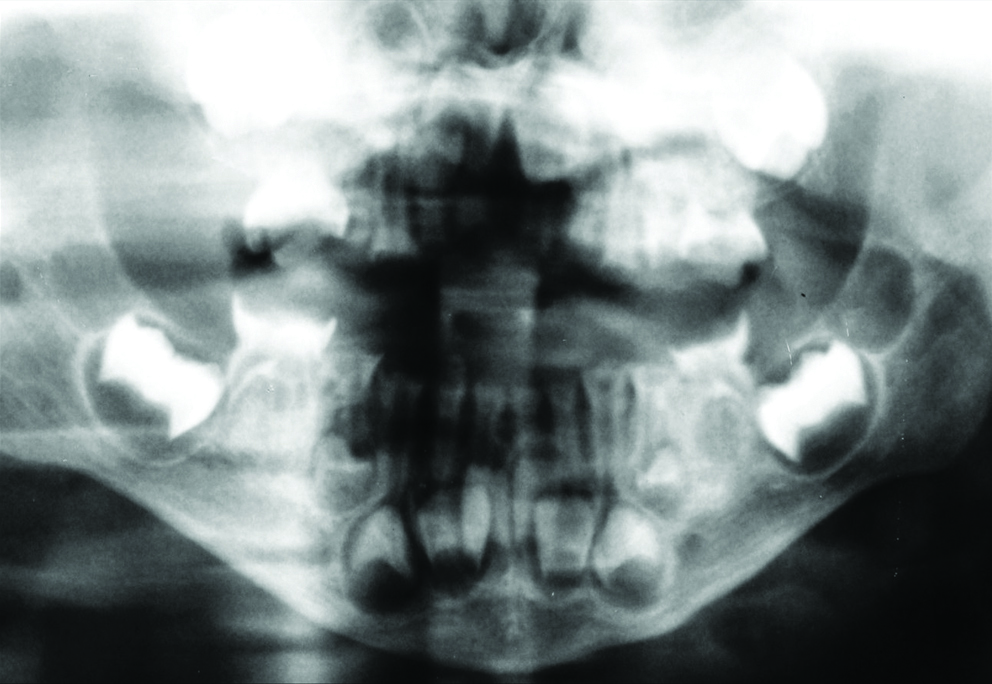
The intraoral examination revealed crown destruction and abscess associated with maxillary anterior teeth in teeth #55 and #65, and root remnants of teeth #54 and #64. The mandibular anterior teeth and primary molars exhibited extensive carious lesions. Tooth #75 exhibited both abscess and oedema [Table/Fig-1]. Extraoral swelling was associated with pulp necrosis in tooth #75 [Table/Fig-2].
a) Three-year-old patient with evidence of swelling on left side of face; b) Upper arch with extensive carious lesions and root remnants; c) Lower arch with severe crown destruction and swelling of tooth #75.
Diagnostic panoramic radiograph.
(*As the child was not very cooperative only this image could be obtained.)
The option for multiple extractions and prosthetic rehabilitation was due to the extensive tooth decay. The guardians rejected general anaesthesia due to the high cost and limited access to specialised healthcare services. A written consent was obtained from the mother.
The treatment plan consisted of behavioural changes and the guardians received instructions on oral hygiene and the use of a fluoride toothpaste. The behavioural recommendations were weaning from breastfeeding, regular eating times, and the control of sugar intake. All procedures were performed under local anaesthesia (2% lidocaine 1:100,000, DFL, Brazil). Treatment was carried out in multiple sessions, during which the patient’s behaviour became more cooperative but always with the presence of the mother.
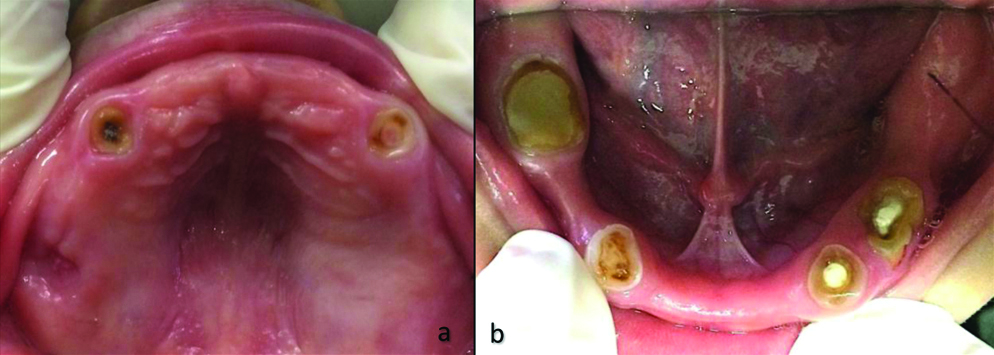
Teeth #51, #52, #61, and #62 were extracted in the first session, followed by the extraction of teeth #54 and #55 and finally teeth #64 and #65 in subsequent sessions. Endodontic treatment was performed on teeth #53 and #63. The canals (length: 12 mm) were obturated with Feapex (Formula and Ação, Brazil) and restored with composite resin (Filtek Bulk Fill- 3M). The procedures on the lower arch began with the extraction of tooth #75 and endodontic treatment of tooth #74, followed by the extraction of tooth #84 and endodontic treatment of tooth #85 in subsequent sessions. Finally, teeth #71, #72, #81, and #82 were extracted and endodontic treatment was performed on teeth #83 and #73, followed by composite resin restoration. A total of 10 sessions were needed until the oral cavity was able to receive the prostheses [Table/Fig-3].
a) Upper arch after extractions and maintenance of teeth #53 and #63; b) Lower arch and maintenance of teeth #73, #74, #83, and #85.
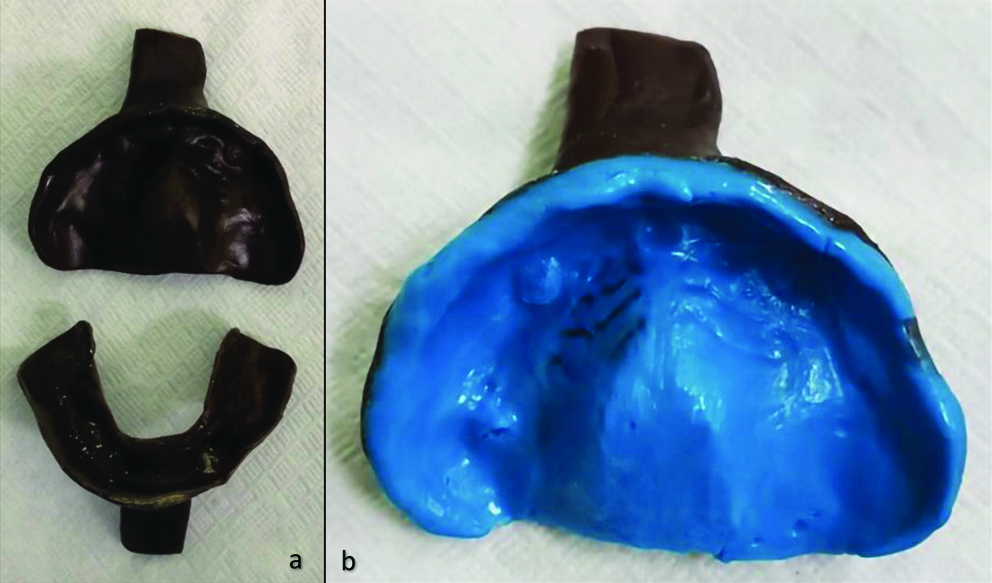
The multiple extractions led to the loss of vertical dimension, with difficulty chewing and speaking as well as compromised facial aesthetics. Rehabilitation involved the use of complete prostheses (upper and lower) based on the motivation and cooperation of the parents. Moreover, the child was cognitively able to use the dentures. The roots of the primary canines and teeth #74 and #85 were maintained, enabling greater retention and stabilisation of the prostheses. Fabrication involved anatomic moulding with alginate (Orthoprint, Zhermack) and the creation of individual acrylic resin trays (Autocril, Imodonto). The impression was performed with addition silicone (Express XT Denso, 3M) and the test base was made in acrylic resin, with wax (Artwax, Odontomega) used to record maxillomandibular relations. The teeth were then selected and assembled in an articulator (10600, DentFlex), followed by testing and adaptation of the prosthesis. On the day of delivery of the dentures, occlusion and retention were adjusted to ensure proper joint function, balance, and the absence of trauma. A total of six sessions were needed to fabricate the dentures. The parents and the child were instructed regarding use and hygiene (daily brushing of the dentures) as well as the importance of periodic clinical monitoring. The wearing instructions were continual denture use during the day and removal to sleep at night [Table/Fig-4].
a) Individual upper and lower moulds; b) Modelling with addition silicone (Express XT Denso-3M).
The child returned in one week for the first follow-up. The next evaluation took place after three months and there was no need to modify the prostheses. According to the mother, the child used the dentures continuously and was able to speak well. The last evaluation took place after six months. In this phase, we sought to motivate the child and the family to adopt healthy habits of diet and oral hygiene in order to avoid the recurrence of dental caries [Table/Fig-5].
a) Complete upper and lower prostheses; b) Patient well adapted to prosthetic rehabilitation.

Discussion
Early Childhood Caries is defined as one or more carious lesions (cavitated or not), extracted teeth, or restored surfaces in children less than six years of age. This condition can lead to pain, swelling, infection, and even tooth loss [1]. Early Childhood Caries is also associated with difficulties sleeping and eating, irritability, and psychological problems [2,3]. Recent studies demonstrate an increase in ECC throughout the world, affecting more than 600 million children [4].
Children are usually uncooperative for dental treatments and techniques are used to restrict physical movements, enabling the procedures with protection and safety for the patient, guardian, and dental team [5,6]. In the present case, the family had difficulty obtaining dental care for the child and previous dental care involved only the prescription of antibiotics and referral to other services without proper intervention. One-fifth of health units in Brazil do not provide dental care for young children [7-9].
Prosthetic rehabilitation in cases of multiple loss is essential to restoring chewing function, improving phonetics, preventing the development of harmful oral habits, and minimising negative psychological impacts [10-12]. Although total removable prostheses are uncommon for this age group, it was adequate for this patient, as three to five years of age is a period of stability in the bone on both the transverse and sagittal planes [10]. In a recently published case report, a three-year-old child with ECC received a fixed prosthesis as part of his oral rehabilitation [13]. However, this was not an option for the present case as the multiple tooth losses and the remaining dental roots impeded the fixation of a prosthesis or the adaptation of a removable space maintainer. The few studies on the use of dentures in young children have reported positive outcomes [11,12].
Although the fabrication of complete dentures is similar to that performed for adults and the clinicians concur that children adapt extremely well, it is important to determine the expected level of cooperation [10,14]. Regular check up appointments should be made every three to six months and modifications must be made to accommodate the child’s growth and development until the eruption of permanent teeth.
Conclusion(s)
Early Childhood Caries is a public health problem that affects children throughout the world. Rehabilitation with removable complete prostheses is a viable treatment option that can lead to improvements in eating, speech, chewing, and aesthetics.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: May 25, 2020
Manual Googling: Aug 19, 2020
iThenticate Software: Sep 25, 2020 (1%)
[1]. Marcenes W, Kassebaum NJ, Bernabé E, Flaxman A, Naghavi M, Lopez A, Global burden of oral conditions in 1990-2010: A systematic analysisJ Dent Res 2013 92(7):592-97.10.1177/0022034513490168 [Google Scholar] [CrossRef]
[2]. Bönecker M, Abanto J, Tello G, Oliveira LB, Impact of dental caries on preschool children’s quality of life: An updateBraz Oral Res 2012 26(Suppl 1):103-07.10.1590/S1806-8324201200070001523318751 [Google Scholar] [CrossRef] [PubMed]
[3]. Kramer PF, Feldens CA, Ferreira SH, Bervian J, Rodrigues PH, Peres MA, Exploring the impact of oral diseases and disorders on quality of life of preschool childrenCommunity Dent Oral Epidemiol 2013 41(4):327-35.10.1111/cdoe.1203523330729 [Google Scholar] [CrossRef] [PubMed]
[4]. Tinanoff N, Baez RJ, Diaz Guillory C, Donly KJ, Feldens CA, McGrath C, Early childhood caries epidemiology, aetiology, risk assessment, societal burden, management, education, and policy: Global perspectiveInt J Paediatr Dent 2019 29(3):238-48.10.1111/ipd.1248431099128 [Google Scholar] [CrossRef] [PubMed]
[5]. Vasiliki B, Konstantinos A, Vassilis K, Nikolaos K, van Loveren C, Jaap V, The effect of parental presence on the child’s perception and co-operation during dental treatmentEur Arch Paediatr Dent 2016 17(5):381-86.10.1007/s40368-016-0241-027378545 [Google Scholar] [CrossRef] [PubMed]
[6]. American Academy of Pediatric DentistryProtective stabilization for pediatric dental patientsIn: The Reference Manual of Pediatric Dentistry 2019-2020 2019 Chicago, ILAmerican Academy of Pediatric Dentistry:280-85. [Google Scholar]
[7]. Essvein G, Baumgarten A, Rech RS, Hilgert JB, Neves M, Dental care for early childhood in Brazil: From the public policy to evidenceRev Saude Publica 2019 53(1):1510.11606/S1518-8787.201905300054030726496 [Google Scholar] [CrossRef] [PubMed]
[8]. Aminoshariae A, Kulild JC, Donaldson M, Hersh EV, Evidence-based recommendations for analgesic efficacy to treat pain of endodontic originJ Am Dent Assoc 2016 147(10):826-39.10.1016/j.adaj.2016.05.01027475974 [Google Scholar] [CrossRef] [PubMed]
[9]. Machado GCM, Daher A, Costa LR, Factors associated with no dental treatment in preschoolers with toothache: A cross-sectional study in outpatient public emergency servicesInt J Environ Res Public Health 2014 11(8):8058-68.10.3390/ijerph11080805825111875 [Google Scholar] [CrossRef] [PubMed]
[10]. Tannure P, Moraes G, Borba M, Abrahão A, Andrade M, Fidalgo T, Prosthetic oral rehabilitation of a child with S-ECC: A case report with histopathologic analysisJ Clin Pediatr Dent 2015 39(5):410-14.10.17796/1053-4628-39.5.41026551361 [Google Scholar] [CrossRef] [PubMed]
[11]. Sacramento PA, de Castilho ARF, Frasseto F, Gaviao MBD, Nobre-dos-Santos M, Rontani RMP, One-year clinical evaluation of oral rehabilitation after the loss of multiple primary teethGen Dent 2011 59(3):230-33. [Google Scholar]
[12]. Parisotto TM, De Souza-E-Silva CM, Steiner-Oliveira C, Nobre-dos-Santos M, Gavião MB, Prosthetic rehabilitation in a four-year-old child with severe early childhood caries: A case reportJ Contemp Dent Pract 2009 10(2):90-97.10.5005/jcdp-10-2-9019279977 [Google Scholar] [CrossRef] [PubMed]
[13]. Goldenfum GM, Dallagnol SC, Rodrigues JA, Early childhood caries: A case report of an extensive rehabilitationJ Clin Diag Res 2018 12(4):ZD01-03.10.7860/JCDR/2018/31018.11360 [Google Scholar] [CrossRef]
[14]. Mishra A, Pandey R, Pandey N, Jain E, A pedoprosthetic rehabilitation in patients with severe early childhood caries (S-ECC)BMJ Case Rep 2013 2013:bcr201301026910.1136/bcr-2013-01026923843409 [Google Scholar] [CrossRef] [PubMed]