Tumours of oral cavity mostly require nasotracheal intubation. Nasal intubation with traditional direct laryngoscopy requires more time compared to the oral intubation. Therefore, nasotracheal intubation produces more intense haemodynamic stress response which last significantly longer than those following oral intubation [7].
Oral and maxillofacial surgeries involve surgical manipulation of facial skeletal elements and thus have marked impact on the cardiovascular stress response, which can result in a significant increase in the MAP and HR. To blunt such haemodynamic stress response, frequent adjustments in the depth of anaesthesia and analgesia are required [8]. Controlled hypotension is of utmost importance in such surgeries to reduce bleeding in the surgical field and thereby facilitate the surgery [4]. Surgical stimulus like hemi-mandibulectomy which is commonly performed in surgeries involving buccal mucosa cancer results in an intense surge in stress response. Dexmedetomidine is considered as a near-ideal hypotensive agent due to the ease of its administration, predictable interaction with anaesthetic agents and lack of major side effects while maintaining adequate perfusion of the vital organs [4]. Postoperatively, a compromised airway is a particular concern in these patients. Utilisation of an adjuvant treatment that effectively controls the autonomic responses with fewer side effects would be extremely beneficial [8].
Lacuna in knowledge exists in terms of the use of low doses of dexmedetomidine without the bolus dose for attenuation of haemodynamic stress response to nasotracheal intubation and other surgical stimuli intraoperatively in oral oncological surgeries. Thus, the aim of this study was to study the effect of 2 low doses of dexmedetomidine, 0.4 mcg/kg/hr, 0.2 mcg/kg/hr and normal saline (0.9%) on haemodynamic stress response in patients undergoing elective oral oncological surgeries, by observing the following parameters: HR, SBP, DBP, and MAP. The secondary objectives were to assess the incidence of adverse effects like bradycardia, hypotension, hypertension and to monitor saturation of oxygen (SpO2) during the 15 minute period of infusion prior to pre-oxygenation.
Materials and Methods
This study was a single blinded, randomised clinical controlled study in which 120 patients scheduled to undergo elective oral oncological surgeries under general anaesthesia wherein the patients did not know which group they belonged to when enrolled. The Institutional Ethical Committee approval (No:KMIO/MEC/016/24.November.2016) and written informed consent from the patients were obtained. The study was conducted from December 2016 to December 2017.
Patients aged between 18 to 65 years, belonging to ASA physical status Grade I and Grade II and consenting for the study were included. Exclusion Criteria were patients with difficult airway, chronic hypertension, morbid obesity, severe cardiac disease, diabetes mellitus with autonomic neuropathy, patients on drugs like beta blockers or calcium channel blockers and with hepatic or renal dysfunction.
Procedure
A total of one twenty patients were randomly allocated to one of the three groups by a computer generated table of random numbers. Equal number of patients was allotted in each group [Table/Fig-1].
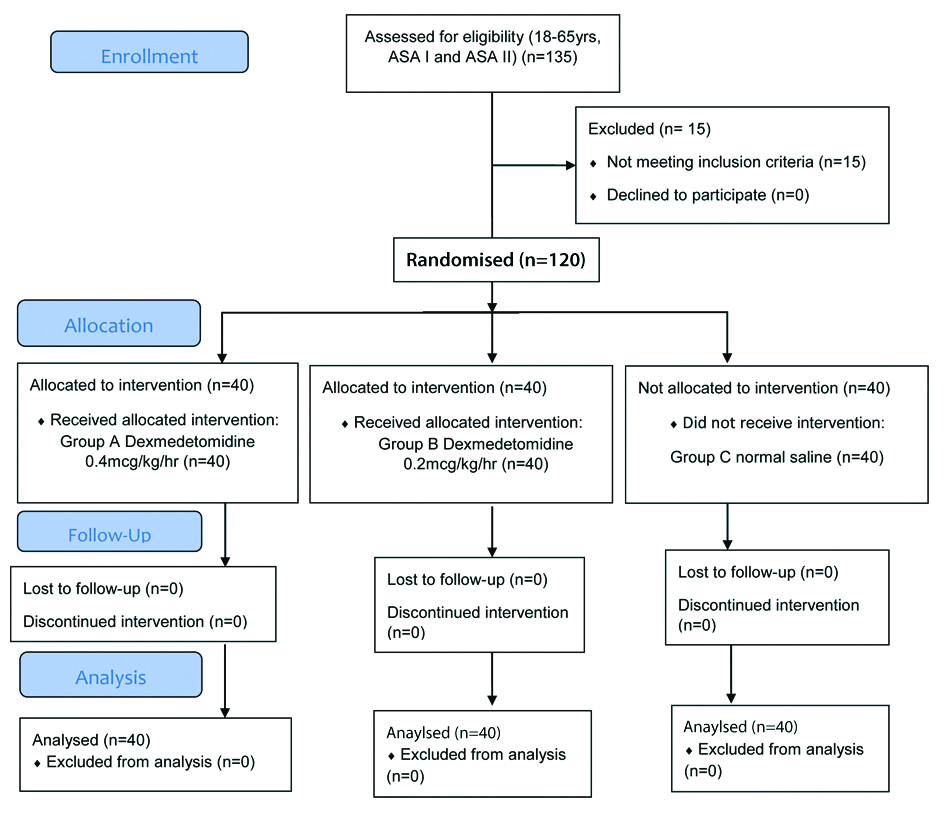
Group A (40 patients) received intravenous dexmedetomidine infusion at the rate of 0.4 mcg/kg/hr
Group B (40 patients) received intravenous dexmedetomidine infusion at the rate of 0.2 mcg/kg/hr
Group C (40 patients) received normal saline (0.9%) infusion intravenously at a comparable rate
The selected patients underwent pre-anaesthetic check-up. All patients were explained regarding the surgical procedure. Premedication, induction and maintenance of anaesthesia was standardised as per institutional protocol. All the patients were kept fasting for 6 hours prior to the procedure.
On arrival to operation theatre, NPO status was confirmed, routine noninvasive monitoring with pulse oximetry, Non-Invasive Blood Pressure (NIBP), Electrocardiogram (ECG) were connected. Basal parameters were recorded. Intravenous line was secured and adequate intravenous crystalloid infusion was started in all patients. Another intravenous line was secured for dexmedetomidine infusion. The infusion was prepared at a concentration of 4 mcg/mL. (0.5 mL containing 50 mcg of the drug was taken in a 20 mL syringe and diluted upto 12.5 mL with normal saline). It was administered through an infusion pump. Depending on the weight of the patient and dose selected for the patient as per the randomisation chart, the pump was set so as to deliver the calculated dose of dexmedetomidine. Subsequently, all patients were premedicated with IV injection Midazolam (0.02 mg/kg), injection Ondansetron (0.05 mg/kg) and injection Fentanyl (1 mcg/kg) IV. Fifteen minutes after the drug infusion was started, patients were preoxygenated for three minutes with 100% oxygen, general anaesthesia was induced with injection Propofol (2 mg/kg) IV and after confirming adequacy of ventilation, injection Succinylcholine (1.5 mg/kg) was administered to facilitate laryngoscopy and tracheal intubation. Patients were intubated nasally with appropriate size cuffed endotracheal tube and tube position was confirmed by bilateral five point auscultation. Patient was connected to volume controlled mode of mechanical ventilation. Anaesthesia was maintained with O2:N2O (50%:50%) and Isoflurane to maintain HR and BP within 20% of baseline values. Muscle relaxation was maintained with injection Vecuronium bromide IV, an initial loading dose of 0.08 mg/kg followed by intermittent doses of injection Vecuronium (0.01 mg/kg) when required.
Intraoperative monitoring consisted of NIBP, MAP, continuous ECG, and SpO2. Patients were observed for any side effects throughout the surgery. Side effects like bradycardia was treated with injection Atropine (0.01 mg/kg) IV when the HR was less than <50 bmp. Hypotension (Fall in blood pressure SBP <90 mmhg or MAP <60 mmHg) was treated with bolus of intravenous fluids and vasopressors if required. Hypertension (blood pressure more than 20% from baseline) was treated with nitroglycerine infusion IV. Respiratory depression during the period of infusion prior to pre-oxygenation was considered as (SPO2 <95%).
At the beginning of skin closure, drug infusion was stopped. At the end of surgery, neuromuscular blockade was reversed with injection Neostigmine (0.05 mg/kg) and injection Glycopyrolate (0.01 mg/kg) IV. On observation of regular, spontaneous and adequate respiration with good muscle power, the patient was shifted to ICU with nasal endotracheal tube in situ as per institutional protocol. As per ASA guidelines, standard monitors were connected to the patient and the variables like HR, blood pressure; MAP and SpO2 were noted down at specified time intervals.
Statistical Analysis
Sample Size
Software R environment ver. 3.2.2 was used to derive the following formula to compute sample size and power, respectively: Where, k is the number of groups and n is the common sample size in each group. For a one-way ANOVA effect size is measured by f where;
For results to be significant, power of 80% and α level of 5%, the sample size requires approximately 40 patients in each group. f=0.4.
Thus, a total of 120 patients were distributed randomly into 3 groups of 40 patients each, by a computer generated table of random numbers. The primary outcome measure used for sample size was MAP.
The Statistical software namely SPSS 18.0, and R environment ver. 3.2.2 were used for the analysis of the data and Microsoft Word and Excel have been used to generate graphs, tables etc. Descriptive and inferential statistical analysis has been carried out in the present study. Results on continuous measurements are presented in Mean±SD (Min-Max) and results on categorical measurements are presented in Number (%). Analysis of variance (ANOVA) has been used to find the significance of study parameters between three or more groups of patients. Post-Hoc Tukey’s test (two-tailed, independent) has been used to find the significance of study parameters on continuous scale between two groups (Inter group analysis) on metric parameters. Chi-square test has been used to find the significance of study parameters on categorical scale between two or more groups, Nonparametric setting for Qualitative data analysis. The level p<0.05 was considered as the cut off value or significance.
Results
The study population was similar and comparable in terms of demographic parameters such as age, gender, height, weight and ASA physical status. Participants in all three groups were matched in terms of diagnosis and procedures done which were similar in all three groups and not statistically significant [Table/Fig-2,3,4,5,6 and 7].
Age distribution of study population.
| Age in years | Group A (n=40) | Group B (n=40) | Group C (n=40) | Total | p-value |
|---|
| <30 | 2 (5%) | 0 (0%) | 0 (0%) | 2 (1.67%) | 0.739 |
| 30-40 | 5 (12.5%) | 5 (12.5%) | 5 (12.5%) | 15 (12.5%) |
| 41-50 | 14 (35%) | 13 (32.5%) | 11 (27.5%) | 38 (31.67%) |
| 51-60 | 18 (45%) | 20 (50%) | 22 (55%) | 60 (50%) |
| 61-65 | 1 (2.5%) | 2 (5%) | 2 (5%) | 5 (4.17%) |
| Total | 40 (100%) | 40 (100%) | 40 (100%) | 120 (100%) |
| Mean±SD | 48.05±9.23 | 50.55±8.23 | 51.15±7.49 | 49.92±8.39 |
Chi-square test
Gender distribution of study population.
| Gender | Group A (n=40) | Group B (n=40) | Group C (n=40) | Total | p-value |
|---|
| Female | 24 (60%) | 23 (57.5%) | 23 (57.5%) | 70 (58.3%) | 0.966 |
| Male | 16 (40%) | 17 (42.5%) | 17 (42.5%) | 50 (41.7%) |
| Total | 40 (100%) | 40 (100%) | 40 (100%) | 120 (100%) |
Chi-square test
Comparison of Weight and Height in three groups of patients studied.
| Variables | Group A (n=40) | Group B (n=40) | Group C (n=40) | Total | p-value |
|---|
| Weight (kg) | 58.05±8.66 | 54.28±10.04 | 55.18±9.57 | 55.83±9.50 | 0.179 |
| Height (cm) | 161.90±8.86 | 158.45±11.21 | 157.75±10.48 | 159.37±10.31 | 0.156 |
Chi-square test
ASA Grade distribution in three groups of patients studied.
| ASA grade | Group A (n=40) | Group B (n=40) | Group C (n=40) | Total | p-value |
|---|
| I | 35 (87.5%) | 32 (80%) | 29 (72.5%) | 96 (80%) | 0.245 |
| II | 5 (12.5%) | 8 (20%) | 11 (27.5%) | 24 (20%) |
| Total | 40 (100%) | 40 (100%) | 40 (100%) | 120 (100%) |
Chi-square test
Diagnosis distribution in three groups of patients studied.
| Diagnosis | Group A (n=40) | Group B (n=40) | Group C (n=40) | Total | p-value |
|---|
| CA BM | 14 (35%) | 25 (62.5%) | 22 (55%) | 61 (50.8%) | 0.3255 |
| CA L GBS | 12 (30%) | 4 (10%) | 6 (15%) | 22 (18.3%) |
| CA Tongue | 6 (15%) | 7 (17.5%) | 4 (10%) | 17 (14.2%) |
| CA L RMT | 5 (12.5%) | 3 (7.5%) | 2 (5%) | 10 (8.3%) |
| CA R Lower alveolus | 0 (0%) | 1 (2.5%) | 2 (5%) | 3 (2.5%) |
| CA Lip | 1 (2.5%) | 0 (0%) | 1 (2.5%) | 2 (1.7%) |
| CA L Maxilla | 1 (2.5%) | 0 (0%) | 1 (2.5%) | 2 (1.7%) |
| CA lower lip | 0 (0%) | 0 (0%) | 1 (2.5%) | 1 (0.8%) |
| CA palate | 0 (0%) | 0 (0%) | 1 (2.5%) | 1 (0.8%) |
| CA R angle of mouth+BM | 1 (2.5%) | 0 (0%) | 0 (0%) | 1 (0.8%) |
| Total | 40 (100%) | 40 (100%) | 40 (100%) | 120 (100%) |
CA: Cancer; BM: Buccal mucosa; GBS: Gingivobuccal sulcus; RMT: Retromolar trigone; R: Right; L: Left
Chi-square test
Procedure distribution in three groups of patients studied.
| Procedure | Group A (n=40) | Group B (n=40) | Group C (n=40) | p-value |
|---|
| Partial Maxillectomy | 1 (2.5%) | 0 (0%) | 1 (2.5%) | p=0.540 |
| Partial Maxillectomy+ND | 1 (2.5%) | 0 (0%) | 0 (0%) |
| L Subtotal Maxillectomy | 1 (2.5%) | 0 (0%) | 0 (0%) |
| WE+ R Maxillectomy | 0 (0%) | 0 (0%) | 1 (2.5%) |
| Glossectomy+B/L MND | 1 (2.5%) | 0 (0%) | 0 (0%) |
| WE+Upper alveolectomy | 0 (0%) | 0 (0%) | 1 (2.5%) |
| HM+WE | 0 (0%) | 1 (2.5%) | 0 (0%) |
| WE+MND | 3 (7.5%) | 5 (12.5%) | 7 (17.5%) |
| WE+Forehead flap | 0 (0%) | 1 (2.5%) | 0 (0%) |
| WE+HM+MND | 9 (22.5%) | 9 (22.5%) | 5 (12.5%) |
| WE+MND+Forehead flap | 1 (2.5%) | 0 (0%) | 0 (0%) |
| WE+MND+NL flap | 1 (2.5%) | 0 (0%) | 0 (0%) |
| WE+MND+PMMC | 1 (2.5%) | 0 (0%) | 0 (0%) |
| WE+HM+MND+Local flap | 1 (2.5%) | 0 (0%) | 0 (0%) |
| WE+HM+MND+PMMC | 20 (50%) | 24 (60%) | 25 (62.5%) |
ND: Neck dissection; L: Left; WE: Wide excision; R: Right; B/L: Bilateral; MND: Modified neck dissection; HM: Hemimandibulectomy; NL: Nasolabial; PMMC: Pectoralis major myocutaneous flap
Chi-Square test used
Baseline and 15 minute HR of all three groups are statistically insignificant.
After intubation, group A showed significant reduction in HR compared to group C (p=0.023). There was no significant statistical difference in terms of HR distribution at all-time intervals between group A and B. Whereas Group C had higher HR than Group A and B at majority of the time intervals intraoperatively which was statistically significant (p<0.05). Before shifting to ICU, the HR of all three groups was comparable [Table/Fig-8].
Comparison of Heart Rate (HR) (beats/min) (Mean±SD) in three groups of patients studied.
| Heart rate (beats/min) | Results | Statistical significance (p-value) |
|---|
| Group A (n=40) | Group B (n=40) | Group C (n=40) | A-B | A-C | B-C |
|---|
| Baseline | 88.20±12.79 | 83.98±13.18 | 82.68±12.49 | 0.307 | 0.136 | 0.893 |
| 15 min | 84.33±12.38 | 83.00±15.53 | 85.18±12.54 | 0.900 | 0.958 | 0.754 |
| After intubation | 84.68±11.51 | 89.23±16.46 | 93.20±14.39 | 0.331 | 0.023* | 0.429 |
| 30 min | 82.33±10.24 | 83.70±13.77 | 87.10±12.34 | 0.870 | 0.191 | 0.429 |
| 1 h | 79.20±8.81 | 79.08±10.10 | 84.78±11.93 | 0.998 | 0.046* | 0.040* |
| 1 h 30 min | 78.03±8.65 | 78.35±10.25 | 85.97±12.95 | 0.990 | 0.004** | 0.006** |
| 2 h | 77.21±9.00 | 78.68±9.99 | 84.39±10.46 | 0.791 | 0.006** | 0.038* |
| 2 h 30 min | 75.26±9.70 | 80.20±8.73 | 86.72±8.91 | 0.085+ | <0.001** | 0.020* |
| 3 h | 73.52±12.62 | 77.60±7.48 | 88.81±11.20 | 0.517 | <0.001** | 0.017* |
| 3 h 30 min | 82.86±8.15 | 76.50±17.68 | 80.75±7.80 | 0.689 | 0.933 | 0.864 |
| 4 h | 80.50±7.00 | - | 81.00±9.35 | 0.025+ | <0.001** | 0.014* |
| Before shifting to ICU | 77.43±10.65 | 83.38±9.00 | 89.83±10.50 | 0.307 | 0.136 | 0.893 |
ANOVA, Post-Hoc Tukey test; +Suggestive significance (p-value: 0.05<p<0.10); *Moderately significant (pvalue: 0.01<p≤0.05); **Strongly significant (p-value: p≤0.01)
Baseline SBP, DBP and MAP of all three groups showed no statistical significance. After intubation, group A showed a significant reduction in SBP, DBP and MAP when compared to group B and group C with statistical significance p=0.009, p=0.001; p=0.001 and p=0.001, p=0.021, p= 0.001, respectively. Also, Group C has higher SBP, DBP and MAP distribution compared to Group A at almost all time intervals intraoperatively which are statistically significant (p<0.001) and higher SBP and MAP compared to Group B at majority of the time intervals (p<0.05).
Groups B and C showed no significant statistical differences in DBP.
Before shifting the patient to ICU, group A showed statistically significant lower values of SBP, DBP and MAP when compared to group B and group C (p<0.001). Changes in SBP, DBP and MAP are shown in [Table/Fig-9,10 and 11], respectively.
Comparison of SBP (mm Hg) in three groups of patients studied.
| SBP (mm Hg) | Results | Statistical significance (p-value) |
|---|
| Group A (n=40) | Group B (n=40) | Group C (n=40) | A-B | A-C | B-C |
|---|
| Baseline | 139.47±11.18 | 139.3±11.45 | 137.45±9.42 | 0.937 | 0.378 | 0.432 |
| 15 min | 135.15±10.01 | 137.93±11.59 | 133.43±11.30 | 0.498 | 0.763 | 0.164 |
| After Intubation | 134.85±10.51 | 143.60±14.51 | 147.03±13.83 | 0.009** | <0.001** | 0.472 |
| 30 min | 125.03±8.47 | 131.35±14.14 | 138.63±13.06 | 0.056+ | <0.001** | 0.023* |
| 1 h | 116.68±12.58 | 126.75±9.46 | 135.68±13.65 | 0.001** | <0.001** | 0.003** |
| 1 h 30 min | 116.63±9.91 | 125.05±11.20 | 133.77±10.09 | 0.001** | <0.001** | 0.001** |
| 2 h | 116.31±8.86 | 124.84±10.01 | 133.08±12.51 | 0.002** | <0.001** | 0.003** |
| 2 h 30 min | 111.85±12.82 | 126.33±9.56 | 133.66±10.90 | <0.001** | <0.001** | 0.038* |
| 3 h | 113.76±9.85 | 126.53±9.43 | 133.00±12.92 | 0.003** | <0.001** | 0.227 |
| 3 h 30 min | 114.14±17.36 | 125.50±2.12 | 118.25±7.14 | 0.587 | 0.888 | 0.825 |
| 4 h | 109.50±12.69 | - | 122.00±6.48 | - | <0.001** | - |
| Before shifting to ICU | 122.25±8.02 | 137.35±9.01 | 146.78±13.02 | <0.001** | <0.001** | <0.001** |
ANOVA, Post-Hoc Tukey test; *Moderately significant (p-value: 0.01<p≤0.05); **Strongly significant (p-value: p≤0.01)
Comparison of DBP (mm Hg) in three groups of patients studied.
| DBP (mm Hg) | Results | Statistical significance (p-value) |
|---|
| Group A (n=40) | Group B (n=40) | Group C (n=40) | A-B | A-C | B-C |
|---|
| Baseline | 90.55±7.75 | 90.12±8.86 | 89.15±5.42 | 0.818 | 0.352 | 0.556 |
| 15 min | 88.08±8.56 | 89.33±9.28 | 87.18±5.03 | 0.763 | 0.568 | 0.201 |
| After Intubation | 87.30±6.47 | 94.40±11.13 | 92.58±7.8 | 0.001** | 0.021* | 0.617 |
| 30 min | 83.00±7.23 | 87.08±11.02 | 89.30±7.14 | 0.093+ | 0.004** | 0.486 |
| 1 h | 76.55±8.71 | 84.10±8.41 | 88.05±9.00 | 0.001** | <0.001** | 0.110 |
| 1 h 30 min | 77.55±6.48 | 82.65±8.91 | 86.03±8.67 | 0.015* | <0.001** | 0.157 |
| 2 h | 76.28±6.98 | 82.78±8.07 | 86.22±9.24 | 0.002** | <0.001** | 0.171 |
| 2 h 30 min | 73.68±9.93 | 84.87±9.15 | 87.28±7.44 | <0.001** | <0.001** | 0.559 |
| 3 h | 73.48±8.28 | 82.47±9.53 | 83.06±11.33 | 0.022* | 0.012* | 0.984 |
| 3 h 30 min | 74.14±11.08 | 91.50±2.12 | 74.00±5.48 | 0.091+ | 1.000 | 0.116 |
| 4 h | 70.50±9.29 | - | 78.75±9.00 | - | <0.001** | - |
| Before shifting to ICU | 77.75±6.15 | 90.58±8.41 | 90.98±8.86 | <0.001** | <0.001** | 0.972 |
ANOVA, Post-Hoc Tukey test; *Moderately significant (p-value: 0.01<p≤0.05); **Strongly significant (p-value: p≤0.01)
Comparison of MAP (mmHg) in three groups of patients studied.
| MAP (mmHg) | Results | Statistical significance (p-value) |
|---|
| Group A (n=40) | Group B (n=40) | Group C (n=40) | A-B | A-C | B-C |
|---|
| Baseline | 106.86±8.17 | 106.52±8.73 | 105.25±5.51 | 0.858 | 0.305 | 0.439 |
| 15 min | 103.77±8.62 | 105.53±9.10 | 103.3±5.01 | 0.597 | 0.766 | 0.179 |
| After Intubation | 103.15±7.10 | 110.8±11.46 | 110.77±8.25 | 0.001** | 0.001** | 1.000 |
| 30 min | 97.01±6.34 | 101.83±11.4 | 105.74±8.22 | 0.044* | <0.001** | 0.126 |
| 1 h | 89.68±9.55 | 98.19±7.92 | 103.93±9.54 | <0.001** | <0.001** | 0.015* |
| 1 h 30 min | 90.33±6.82 | 96.78±8.64 | 101.94±8.09 | 0.001** | <0.001** | 0.012* |
| 2 h | 89.52±7.09 | 96.80±7.49 | 101.84±9.28 | <0.001** | <0.001** | 0.022* |
| 2 h 30 min | 86.36±10.5 | 98.64±8.42 | 103.16±7.15 | <0.001** | <0.001** | 0.131 |
| 3 h | 85.87±8.56 | 97.16±7.74 | 99.71±10.24 | 0.001** | <0.001** | 0.706 |
| 3 h 30 min | 87.48±12.88 | 102.83±2.12 | 87.58±5.83 | 0.211 | 1.000 | 0.260 |
| 4 h | 83.50±10.30 | - | 94.00±9.52 | - | <0.001** | - |
| Before shifting to ICU | 92.58±5.29 | 106.17±7.61 | 109.57±9.04 | <0.001** | <0.001** | 0.107 |
ANOVA, Post-Hoc Tukey test; *Moderately significant (p-value: 0.01<p≤0.05); **Strongly significant (p-value: p≤0.01)
No significant differences in SpO2 across the groups at all time intervals. At the 2nd hour, Group A and B showed statistical significance (p=0.009), however this was clinically insignificant [Table/Fig-12].
Comparison of SpO2% in three groups of patients studied.
| SpO2% | Results | Significance (p-value) |
|---|
| Group A | Group B | Group C | A-B | A-C | B-C |
|---|
| Baseline | 98.80±0.46 | 98.82±0.38 | 98.82±0.38 | 0.832 | 0.832 | 1.000 |
| 15 min | 98.90±0.38 | 98.83±0.38 | 98.83±0.38 | 0.656 | 0.656 | 1.000 |
| After intubation | 100.00±0.00 | 100.00±0.00 | 100.00±0.00 | - | - | - |
| 30 min | 100.00±0.00 | 100.00±0.00 | 100.00±0.00 | - | - | - |
| 1 h | 100.00±0.00 | 100.00±0.00 | 100.00±0.00 | - | - | - |
| 1 h 30 min | 100.00±0.00 | 100.00±0.00 | 100.00±0.00 | - | - | - |
| 2 h | 100.00±0.00 | 99.78±0.42 | 99.86±0.35 | 0.009** | 0.135 | 0.541 |
| 2 h 30 min | 99.65±0.49 | 99.67±0.48 | 99.62±0.49 | 0.986 | 0.975 | 0.930 |
| 3 h | 99.57±0.51 | 99.47±0.52 | 99.63±0.50 | 0.815 | 0.946 | 0.663 |
| 3 h 30 min | 99.00±0.00 | 99.00±0.00 | 99.50±0.58 | 1.000 | 0.071+ | 0.211 |
| 4 h | 99.75±0.5 | - | 99.75±0.50 | - | - | - |
| Before shifting to ICU | 99.25±0.63 | 99.28±0.64 | 99.25±0.59 | 0.982 | 1.000 | 0.982 |
SpO2– Saturation of oxygen; ANOVA, Post-Hoc Tukey test, *Moderately significant (pvalue: 0.01<p≤0.05); **Strongly significant (p-value: p≤0.01)
There is more hypertension in Group C compared to Group A, whereas hypotension with bradycardia and hypertension alone, are more in Group A compared to Group B and C [Table/Fig-13].
Incidence rate of side effects in study groups.
| Side effects | Group A (n=40) | Group B (n=40) | Group C (n=40) | Total (n=120) |
|---|
| No | 35 (87.5%) | 38 (95%) | 30 (75%) | 103 (85.8%) |
| Yes | 5 (12.5%) | 2 (5%) | 10 (25%) | 17 (14.2%) |
| • Hypotension+bradycardia | 3 (7.5%) | 1 (2.5%) | 0 (0%) | 4 (3.3%) |
| • Hypotension | 2 (5%) | 1 (2.5%) | 0 (0%) | 3 (2.5%) |
| • Hypertension | 0 (0%) | 0 (0%) | 10 (25%) | 10 (8.3%) |
Discussion
Oral oncological surgeries require precise, accurate and delicate surgery of hard and soft tissues. Tumour resection from the tongue and floor of the mouth and neck dissections are at increased risk for extensive bleeding. Excessive intraoperative bleeding can cause impaired visibility of the structures. This can be reduced most effectively by maintaining stable haemodynamics throughout the surgery. Since bleeding in the surgical field will be reduced, surgical field operative conditions improve. Thus, maintaining the surgical plane and avoiding unnecessary damage to vital structures. This helps to execute the required surgical procedure easily [9]. Nasotracheal intubation is preferred in patients undergoing these surgeries. So, adequate attenuation of the heamodynamic response to nasotracheal intubation is also necessary.
In this study, two low doses of dexmedetomidine (0.4 mcg/kg/hr and 0.2 mcg/kg/hr) were used. Dexmedetomidine infusion was initiated 15 minutes prior to pre-oxygenation. The rationale behind this was the fact that the onset of action of Dexmedetomidine is 5 minutes and peak effect occurs at 15 min [10].
Dexmedetomidine has been used previously as an infusion with or without bolus dose. Bolus dose results in a biphasic response in blood pressure. Low dose infusion of 0.25 to 0.5 mcg/kg/hr, results in a monophasic response of 10 to 15% fall in MAPs and HR [1]. Thus, in this study the loading dose was not used because it sometimes evokes transient hypertension [11].
In this study, 0.4 mcg/kg/hr of dexmedetomidine showed significant reduction in HR, SBP, DBP and mean arterial blood pressure at intubation when compared to other two groups. But 0.2 mcg/kg/hr reduced SBP and MAP during initial period of surgery and later did not show any efficacy. Dexmedetomidine 0.4 mcg/kg/hr and 0.2 mcg/kg/hr have no significant statistical difference in terms of mean HR values however 0.4 mcg/kg/hr showed decreased SBP, DBP and MAP (p<0.05). This implies that dexmedetomidine in the dose of 0.4 mcg/kg/hr has good sympatholytic activity and thus, effectively attenuates stress response to intubation and surgical stimuli throughout the perioperative period.
Previous studies have used dexmedetomidine infusion rates ranging from 0.1 to 10 mcg/kg/hr1 [9-11] and some studies which used higher dose had increased incidences of hypotension and bradycardia [12-14]. Very few studies have used low dose dexmedetomidine infusion to evaluate its effects on haemodynamic stress response [1,11,12].
Studies by Manne GR et al., and Srivastava VK et al., conducted on patients undergoing laparoscopic cholecystectomy, using different doses of infusion of intravenous dexmedetomidine (0.2 to 0.5 mcg/kg/hr) and saline showed a statistically significant decrease in HR and MAP at intubation and extubation [1,15].
Jo YY et al., used two low doses of intravenous dexmedetomidine (0.4 and 0.2 mcg/kg/hr) in the concentration of 4 mcg/mL and used saline for control group to study the effect of dexmedetomidine on haemodynamic responses during emergence and nasotracheal intubation after oral and maxillofacial surgery [17]. They observed that mean MAP and HR were significantly lower with dexmedetomidine groups intravenous than in the control group during eye opening and after extubation during oral and maxillofacial surgeries that could provide stable haemodynamic profiles. In the present study, the patients were not extubated due to anticipation of postoperative airway oedema and bleed. Hence, the effect of the drug on extubation was not studied.
Dexmedetomidine was started as low dose infusion over 15 minutes prior to induction followed by observation of its effect on SpO2. None of the patients had a fall in SpO2 or required O2 supplementation prior to induction of anaesthesia. Thus, dexmedetomidine did not seem to cause any respiratory compromise.
Hypotension with bradycardia was noticed in more patients who received dexmedetomidine 0.4 mcg/kg/hr compared to those who received dexmedetomidine 0.2 mcg/kg/hr, both of which were treated with IV fluid bolus and inj. Atropine 0.6 mg IV. Patients that had hypotension alone were treated with IV fluid bolus. The patients that received saline had hypertension, which was treated with IV nitroglycerine infusion. None of the above observations were statistically significant. Studies conducted by Manne GR et al., Jagadish V et al., Vaswani JP et al., and Luthra A et al., showed similar side effects [1,17,18]. As these side effects were transient and responded well to treatment in the intraoperative period, they did not require postoperative follow-up.
As maxillofacial cancer surgeries require extensive resection and sometimes reconstruction leading to postoperative airway oedema, all the patients were shifted to ICU with nasal endotracheal tube and extubated during the first postoperative day as per institution protocol.
Limitation(s)
The limitations of the study was that it was limited only to ASA I and II grade patients and its effects on ASA III and IV grade patients were not studied. The study was restricted only to oral and maxillofacial oncological surgeries and was limited in knowing the efficacy of the same low dose of dexmedetomidine in general surgical patients.
Conclusion(s)
It was concluded that low dose intravenous dexmedetomidine infusion of 0.4 mcg/kg/hr was more effective than intravenous dexmedetomidine 0.2 mcg/kg/hr infusion in attenuating the haemodynamic stress response to intubation, and surgical stimulus, in oral and maxillofacial oncological surgeries, with minimal side effects.
Chi-square test
Chi-square test
Chi-square test
Chi-square test
CA: Cancer; BM: Buccal mucosa; GBS: Gingivobuccal sulcus; RMT: Retromolar trigone; R: Right; L: Left
Chi-square test
ND: Neck dissection; L: Left; WE: Wide excision; R: Right; B/L: Bilateral; MND: Modified neck dissection; HM: Hemimandibulectomy; NL: Nasolabial; PMMC: Pectoralis major myocutaneous flap
Chi-Square test used
ANOVA, Post-Hoc Tukey test; +Suggestive significance (p-value: 0.05<p<0.10); *Moderately significant (pvalue: 0.01<p≤0.05); **Strongly significant (p-value: p≤0.01)
ANOVA, Post-Hoc Tukey test; *Moderately significant (p-value: 0.01<p≤0.05); **Strongly significant (p-value: p≤0.01)
ANOVA, Post-Hoc Tukey test; *Moderately significant (p-value: 0.01<p≤0.05); **Strongly significant (p-value: p≤0.01)
ANOVA, Post-Hoc Tukey test; *Moderately significant (p-value: 0.01<p≤0.05); **Strongly significant (p-value: p≤0.01)
SpO2– Saturation of oxygen; ANOVA, Post-Hoc Tukey test, *Moderately significant (pvalue: 0.01<p≤0.05); **Strongly significant (p-value: p≤0.01)