Introduction
Psychological trauma may occur when an individual suffers from serious loss or his/her life is under serious threat. If such traumatic experience is failed to be resolved, it may lead to drug misuse including alcohol dependence. Early childhood trauma may predispose an individual to mental health issues, including development of alcohol dependence later in life. Childhood trauma includes various forms like emotional abuse, physical abuse, sexual abuse, emotional neglect and physical neglect. Those who experience and suffer from early-life trauma may consume alcohol to cope with trauma related symptoms. In general, onset of trauma precedes onset of alcohol dependence. Childhood trauma can act as preceding factor for alexithymia. Childhood emotional abuse might be a risk factor for alexithymia among inpatient alcohol dependents.
Aim
Present synopsis aims at finding out relationship between childhood trauma and alexithymia in persons diagnosed with Alcohol Dependence Syndrome (ADS).
Materials and Methods
The study would be a case control study. It will be conducted at tertiary healthcare centre from central rural India. Study participants will be selected from psychiatry inpatients with diagnosis of ADS. The study will include total 110 persons of which 55 will belong to “case” group and 55 will belong to “control” group, both including persons between age group of 18-45 years who fulfill International Classification of Mental and Behavioural Disorders 10th revision Diagnostic Criteria for Research (ICD 10 DCR) and diagnostic criteria for ADS.
Conclusion
The study expect to find significant relationship between childhood traumatic experiences and alexithymia among the persons with ADS.
Addiction psychiatry, Emotional abuse, Emotional neglect, Physical abuse, Physical neglect, Sexual abuse
Introduction
The ADS is the diagnostic terminology used in ICD 10 DCR, for people having alcohol consumption pattern leading to clinically significant impairment over a period of 1-12 months [1]. Operational definition of ADS includes a cluster of physiological, behavioural, and cognitive phenomena in which use of alcohol takes on a much higher priority for a given individual than other behaviours that once had greater value [1]. These persons often take alcohol in larger amounts or over a longer period then intended and there is persistent desire or unsuccessful efforts to cut down or control the alcohol use. They spend more time in activities to obtain alcohol, use alcohol, or recover from its effects. They also develop a craving, or a strong desire to use alcohol. Recurrent alcohol use results in their failure to fulfill major role obligations at work, school, or home. They drink alcohol continuously despite having knowledge about alcohol induced/exacerbated persistent as well as recurrent social and/or interpersonal problems. Important social, occupational, or recreational activities are given up or reduced because of alcohol use. They recurrently use alcohol in situations, in which it is physically hazardous and alcohol use is persistent despite of persistent and/or recurrent physical and/or psychological problems that have been caused or exacerbated by alcohol. Later, continued alcohol use leads to tolerance and finally patient lands up into alcohol withdrawal when he rapidly decreases or stop drinking alcohol [1]. ADS have been prevalent across the country in all societal strata. It is a problem of public health concern. Alcohol consumption pattern varies as regards with age, education, religion, liquor type and other socio-demographic data. Over last 20 years period, alcohol use pattern has varied between various societies and cultures [2]. According to available data from World Health Organisation (WHO), worldwide 5.9% of total deaths are due to alcohol consumption [3]. About 16% of individuals with age of 15 years and above are indulged in heavy episodic drinking [3]. Prevalence of ADS among Indian male population is 9.1% [4]. As per the data from available literature, the prevalence of heavy episodic drinking among Indian males with age above 15 years is 28.4% [4]. Literature has also shown that the prevalence of heavy episodic drinking among Indian male drinkers only with age above 15 is 55.1% [4]. Binge alcohol use is defined as five or more drinks on one occasion in the prior 30 days [5]. Early onset of drinking is defined as onset of alcohol consumption prior to age of 22 years, while late onset of drinking is defined as onset of alcohol consumption after the age of 22 years [6]. Severity of ADS is measured by using Severity of Alcohol Dependence Questionnaire (SADQ) [7].
Trauma typically occurs when the individual’s life is under threat or when a serious loss has been experienced. If childhood psychological trauma is not effectively dealt and resolved, it may predispose an individual to development of alcohol and drug misuse [8]. Early childhood psychological traumas may act as predisposing or triggering factors for development of psychological problems, including alcohol dependence in later life. Such individuals with history of childhood traumas may consume alcohol in order to cope with their trauma related symptoms.
So, most of the time, beginning of ADS is preceded by onset of childhood trauma. A study has suggested a strong positive relationship between exposure to psychological traumas in early life and development of ADS later in life, even though it was impossible to establish the direct causal relationship between the two [8]. Although prevalence of traumatic events varies across the different studies, experiencing a lifetime traumatic event is common among persons with substance use disorders including alcohol dependence [9,10]. As many as 89% of the persons with substance use disorder report having experienced a traumatic event in their lifetime [11] and substance use is 1.5-5.5 times more prevalent in individuals with trauma histories than without [12].
Alexithymia was first described by Sifneos PE, who described it in a population of persons with psychosomatic illnesses. It presented with “a relative paucity of fantasy life or day dreaming, impaired emotional functioning and difficulty in finding right words to express their emotions [13]. Alexithymia is a state that is characterised by a triad of difficulty in identification of one’s own feelings, difficulty in differentiating between the physical sensations and emotional arousal and difficulty in explaining one’s own feelings to other people i.e., known as externally oriented [14].
Available literature on addiction has emphasised on the role of dysregulation of emotions in development of drug addiction(s) including alcohol addiction. Individuals with substance dependence had reported use of various substances which included alcohol, opioids and 3,4-methylenedioxymethamphetamine (MDMA) [15]. It has reflected impairment in the perception of facial emotions [15]. Studies have suggested existing link between alexithymia and craving for various drugs including alcohol. But, such a link has not been consistent across different studies [15,16]. Profound alcohol users with alexithymia report more alcohol craving, compulsive drinking urges and obsessive thoughts about alcohol [16], and this association between craving and alexithymia appears to be maintained over 12 weeks [17]. According to a study, number of childhood psychological trauma among individuals of ADS was associated with alexithymia in adulthood, and among the three components of alexithymia, the most commonly associated component was “difficulty in identifying feelings-DIF” factor of TAS-20. Same study suggested that childhood emotional abuse might act as a predisposing factor for development of alexithymia in inpatients suffering from ADS [18].
While searching literature, it was found out that there is paucity of studies on relationship between childhood trauma, alexithymia and ADS [18,19]. Evren C et al., observed that 43.5% of persons with ADS had alexithymia [18]. Same study had observed high rates of Childhood Abuse or Neglect (CAN) and alexithymia in persons with diagnosis of ADS [18]. Evren C et al., inferred that special attention is needed to identify the CAN as well as alexithymia among persons with ADS, as assessment of both early in treatment course could be helpful as maximum part of treatment depends on verbalisation which is otherwise impaired due to co-existing alexithymia in persons with ADS [18]. Dalbudak E et al., inferred that relationship exist between alexithymia and childhood trauma in males with diagnosis of ADS [19]. The research gap exists between the previous studies and present study as in the previous studies [18,19], the relationship of severity and types of various childhood trauma as well as levels of alexithymia with alcohol related parameters like age of onset of alcohol dependence (early versus late), duration of alcohol dependence, severity of ADS, type of liquor (country made versus foreign liquor), quantity of alcohol consumption, pattern of alcohol consumption (daily versus binge drinking) and family history of alcoholism were not assessed, which will be assessed in the present study. Ghogare AS and Saboo AV, had assessed these alcohol related parameters among persons with alcohol use disorder but those parameters were studied in context of alcohol induced cognitive impairment among study participants [20]. In addition, this is the first study in rural setting of India assessing the relation between childhood trauma and alexithymia in persons suffering from ADS. Based on previous study findings [18-20], this study hypothesised that childhood trauma and alexithymia act as inclination predictors towards development of ADS. “Will there be an association between childhood trauma and alexithymia in persons with diagnosis of ADS?” reflects the research question of the current study. The alternate hypothesis (H0) will be that there will be no association between childhood trauma and alexithymia in persons suffering from ADS. The primary objective of the study will be to find out the relationship between childhood trauma and alexithymia among persons suffering from ADS who will be attending psychiatry inpatient as well as outpatient departments of Jawaharlal Nehru Medical College, Datta Meghe Institute of Medical Sciences, Sawangi, Maharashtra, over a period of two years. This study design is chosen with primary aim to assess whether childhood trauma(s) act as risk factor for the development of alexithymia which can in turn lead to ADS.
Materials and Methods
The present case control study will be conducted in psychiatry inpatient as well as outpatient department of Psychiatry of Acharya Vinoba Bhave Rural Hospital and Jawaharlal Nehru Medical College, Sawangi, Maharashtra, India by doctor of philosophy in Psychiatry (PhD in Psychiatry) candidate and the PhD guide will monitor as well as guide the conduction of study. The study will start from August 1, 2020 and study is approved by Institutional Ethics Committee of Datta Meghe Institute of Medical Sciences (Deemed University) with letter number: {DMIMS (DU)/IEC/DEC-2019/8549}, dated 16th December 2019. Prior to beginning of the study, the nature of the study will be explained to study participants in their vernacular language and written informed consent will be taken from study participants. Confidentiality regarding each and every participant’s personal identity and privacy will be strictly maintained.
Inclusion criteria: The study participants fulfilling ICD 10 DCR diagnostic criteria for ADS, giving consent for the study and belonging to the age group of 18-45 years will be included in the study.
Exclusion criteria: Those who will not fulfill ICD 10 DCR diagnostic criteria for ADS, suffering from major medical, surgical or psychiatric disorders other than ADS will be excluded from the study after doing detailed psychiatric as well as clinical evaluations.
Those study participants who will be in the alcohol withdrawal phase will be first made to undergo detoxification treatment phase of one week. Once the detoxification completes, study participants will be assessed for alexithymia and childhood trauma using respective questionnaires described below. Cases will be enrolled consecutively. Case group will include ADS patients with alexithymia and control group will include ADS patients without alexithymia. Both groups will be matched based on socio-demographic characteristics like age, gender as well as alcohol related parameters like age at onset of alcoholism (early versus late), duration of ADS, severity of ADS (mild versus moderate versus severe), type of liquor (country versus foreign), quantity of alcohol consumed and family history of ADS.
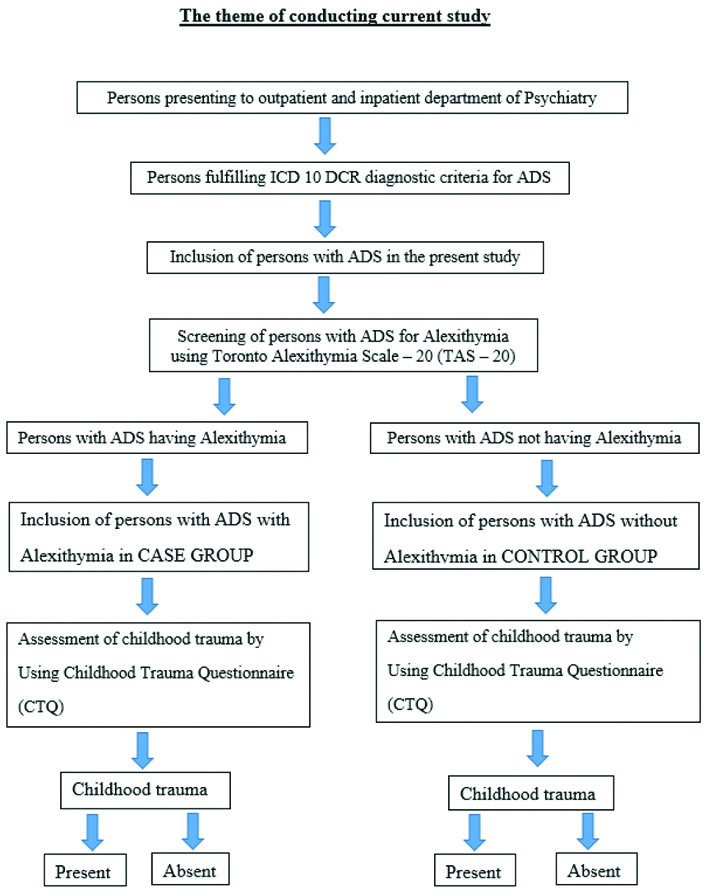
Sample size for the present case control study is calculated using Open Epi software version 3.1 sample size calculation. ODDS for the childhood trauma were 2.65 as reported by Dalbudak E et al., and it was used to calculate the sample size at 80% power and 95% Confidence Interval (CI) [19]. The reported sample size is 55 for the “cases” and 55 for the “controls”. So, final study sample size will be 110. In both case and control groups, the study will assess childhood trauma retrospectively by applying Childhood Trauma Questionnaire (CTQ) to each study participant. So, alexithymia will be the “outcome” in ADS patients, while childhood trauma will be the “exposure”. The theme of conducting the study retrospectively is shown in [Table/Fig-1].
Theme of conducting the current study.
The baseline socio-demographic data will include age, gender, education status, occupation status, religion, marital status, socio-economic status, type of family (nuclear versus joint family) and area of residence. The baseline clinical data will include age at onset of alcohol consumption (early onset versus late onset of drinking), duration of alcohol consumption, severity of ADS as measured by SADQ, type of alcohol consumed (country liquor versus foreign liquor), pattern of alcohol consumption (daily versus binge drinking), and family history of alcoholism. All study participants will be evaluated in detail for past and current history of any medical and surgical disorders as well as psychiatric disorders in addition to ADS. If anyone with ADS found to have major medical, surgical and psychiatric illnesses other than ADS, then they will not be included in the present study.
Psychiatric Measures
All study participants after fulfilling the inclusion criteria will be subjected to assessment by using various scales like SADQ, Toronto alexithymia scale 20 item (TAS-20) and CTQ.
Severity of Alcohol Dependence Questionnaire (SADQ): The SADQ is a 20-item questionnaire designed to measure the severity of dependence on alcohol. It is relatively quick to complete (approximately five minutes) and is easy to score. A score of less than 16 indicates mild alcohol dependence, 16 to 30 indicate moderate alcohol dependence and 31 or higher indicates severe alcohol dependence [21]. SADQ is freely available for research purpose.
Toronto Alexithymia Scale 20 item (TAS-20): Alexithymia is typically measured with the TAS-20 [22]. TAS-20 is a 20-item scale, graded using a five-point Likert scale, that provides total scores ranging from 20 to 100. TAS-20 consists of three subscales: i) difficulty identifying feelings (DIF) (7 items- item no. 1,3,6,7,9,13, and 14); ii) difficulty describing feelings (DDF) (5 items- item no. 2,4,11,12, and 17); and iii) Externally Oriented Thinking (EOT) (items 8- item no. 5,8,10,15,16,18,19, and 20). While there is some disagreement over whether alexithymia should be considered as a dimensional or categorical variable [23], in general, scores above 61 on the TAS-20 tend to be considered clinically significant for alexithymia. Scores between 52 to 61 are considered to be borderline alexithymia while scores of 51 or below are considered to be non-alexithymia [24]. Permission has been obtained from author of the TAS-20 regarding its use for research purpose.
Childhood Trauma Questionnaire (CTQ): In 2003, Bernstein DP et al., shortened the original inventory and created a 28-item questionnaire CTQ in which the items are rated on a five-point Likert scale [25]. Confirmatory factor analysis revealed five subscales, which are emotional abuse, physical abuse, sexual abuse, emotional neglect and physical neglect. The severity of each childhood trauma subscales includes “mild,” “moderate,” “severe,” and “extreme.” According to Bavilacqua L et al., the cut-off scores for each subscale were for sexual abuse ≥8, physical abuse ≥8, emotional abuse ≥10, physical neglect ≥8 and emotional neglect ≥15 [26]. CTQ is copyrighted by Pearson and the authors have obtained quotation (dated 10th September 2019) of amount to be paid from Pearson India for purchasing CTQ for research purpose in the present study. The authors are waiting for institutional grant for purchasing CTQ.
Statistical Analysis
Categorical data in cases and controls will be described using proportions and percentages. Continuous data were presented as mean and standard deviation and tested for statistical significance using a Student’s t-test for two groups’ comparison. Association of childhood trauma with alexithymia will be studied in persons with ADS. Odds ratio of childhood trauma with occurrence of alexithymia will be reported for the same.
Discussion
The present study will assess the relationship between childhood psychological trauma and alexithymia among persons with ADS. Primary aim of this study will be to assess whether childhood psychological trauma(s) act as risk factor for development of alexithymia which may in turn lead to development of ADS. Literature has shown that if such psychological trauma occurring in childhood is not effectively dealt, then it may make an individual vulnerable to development of drug misuse including alcohol dependence later in life [8]. Individuals with such history of childhood traumas may consume alcohol to help themselves cope with their trauma related stress. In such way, in most of cases, onset of ADS preceded the onset of childhood trauma [8]. The present study, will be going to divide the study participants into two groups- case group and control group. In the case group, we will include persons with ADS having alexithymia, while the control group will include persons with ADS without alexithymia. On doing proper matching of cases and controls, the study will assess the types as well as severity of various childhood traumas in both the groups. Various types of childhood trauma that will be assessed in this study will include emotional abuse, physical abuse, sexual abuse, emotional neglect and physical neglect [25]. Then, each type of childhood trauma mentioned above will be divided into different levels of severity like mild, moderate and severe [25]. After an assessment of types and severity of various childhood traumas among “case group” and “control group”, the study will compare them between both groups. Literature has shown that around 89% of individuals with ADS have experienced childhood trauma [11] and substance use including alcohol that is 1.5-5.5 times more prevalent in persons with trauma histories than without [12]. One study had observed that more the number of childhood traumas (i.e., multiple types of childhood traumas in single individual) among persons with ADS, higher were the probability of clinically significant alexithymia [18]. Same study found that persons with ADS had difficulty in identifying their own feelings (DIF) which is one of the components of TAS-20 alexithymia scale [18]. That study also suggested that emotional abuse during childhood act as a predisposing factor for occurrence of alexithymia in patients with diagnosis of ADS [18].
Strength(s)
This study will find out the relationship between types and severity of childhood trauma, levels of alexithymia and alcohol related parameters in-depth like age at onset of alcoholism (early versus late), duration of ADS, severity of ADS, quantity of alcohol consumption, pattern of alcohol consumption (binge versus daily), type of alcohol consumed (country versus foreign liquor), and family history of ADS. Such in-depth assessment of relationship between childhood trauma, alexithymia and alcohol related parameters were not assessed by previous studies. Similarly, such type of data is not available in Indian literature and it is one of the most important areas being overlooked by researchers. Findings of this study might help persons suffering from ADS, to express their feelings and make their treatment plan more successful as most of the therapy of ADS is dependent on verbalisation, which is otherwise difficult among population with alexithymia.
Limitation(s)
First limitation includes recall bias involved in remembering the childhood trauma. Recall bias will affect accurate scoring of the CTQ which will be addressed by allowing participants to get comfortable with the settings and examiner, and by providing them ample time to answer the questions. Second limitation includes the social desirability bias. Social desirability bias manifests when persons on questioning about details of their past as well as present alcohol consumption, may answer in such a manner as to portray themselves in a good light. To reduce the social desirability bias, study participants will be encouraged to give as honest as possible details regarding their alcohol consumption history.
Conclusion(s)
In the conclusion, the probable outcome of this study will be that childhood trauma and alexithymia act as inclination forecasting factors towards the development of ADS. The authors expect to find significant relationship between childhood trauma and alexithymia among persons diagnosed with ADS.
[1]. International Statistical Classification of Diseases and Related Health Problems. Tenth Revision Vol. 1: Tabular list. Vol. 2: Instruction manual. Vol. 3: Index 1992 GenevaWorld Health Organization [Google Scholar]
[2]. Gupta P, Saxena S, Pednekar M, Maulik P, Alcohol consumption among middle-aged and elderly men: A community study from Western IndiaAlcohol Alcohol 2003 38(4):327-31.10.1093/alcalc/agg07712814899 [Google Scholar] [CrossRef] [PubMed]
[3]. World Health Organisation. Global status report on Alcohol and Health 2014. Available at http://apps.who.int/iris/bitstream/10665/112736/1/ 9789240692763_eng.pdf Accessed on 06-11-2017 [Google Scholar]
[4]. Global status report on alcohol and health 2018. Geneva: World Health Organization; 2018. Licence: CC BY-NC-SA 3.0 IGO [Google Scholar]
[5]. Strain EC, Substance-Related Disorders. In: Sadock BJ, Sadock VA, Ruiz PComprehensive Textbook of Psychiatry 2017 10th edPhiladelphiaWolters Kluwer:3255 [Google Scholar]
[6]. Strat YL, Grant BF, Ramoz N, Gorwood P, A new definition of early age at onset in alcohol dependenceDrug Alcohol Depend 2009 108:43-48.10.1016/j.drugalcdep.2009.11.01120018459 [Google Scholar] [CrossRef] [PubMed]
[7]. Schuckit MA, Substance-Related Disorders. In: Sadock BJ, Sadock VA, Ruiz PComprehensive Textbook of Psychiatry 2017 10th edPhiladelphiaWolters Kluwer:3259-60. [Google Scholar]
[8]. Crimmins SM, Cleary SD, Brownstein HH, Spunt BJ, Warley RM, Trauma, drugs and violence among juvenile offendersJ Psychoactive Drugs 2000 32:43-54.10.1080/02791072.2000.1040021110801067 [Google Scholar] [CrossRef] [PubMed]
[9]. Westermeyer J, Wahmanholm K, Thuras P, Effects of childhood physical abuse on course and severity of substance abuseAm J Addict 2001 10:101-10.10.1080/10550490175022776911444153 [Google Scholar] [CrossRef] [PubMed]
[10]. Simpson TL, Miller WR, Concomitance between childhood sexual and physical abuse and substance use problems. A reviewClin Psychol Rev 2002 22:27-77.10.1016/S0272-7358(00)00088-X [Google Scholar] [CrossRef]
[11]. Farley M, Golding JM, Young G, Mulligan M, Minkoff JR, Trauma history and relapse probability among patients seeking substance abuse treatmentJ Subst Abuse Treat 2004 27:161-67.10.1016/j.jsat.2004.06.00615450649 [Google Scholar] [CrossRef] [PubMed]
[12]. Norman SB, Tate SR, Anderson KG, Brown SA, Do trauma history and PTSD symptoms influence addiction relapse context?Drug Alcohol Depend 2007 90:89-96.10.1016/j.drugalcdep.2007.03.00217459611 [Google Scholar] [CrossRef] [PubMed]
[13]. Sifneos PE, The prevalence of ‘alexithymic’ characteristics in psychosomatic patientsPsychother Psychosom 1973 22(2):255-62.10.1159/0002865294770536 [Google Scholar] [CrossRef] [PubMed]
[14]. Bagby RM, Taylor GJ, Affect dysregulation and alexithymia. In GJ Taylor, RM Bagby, & JDA Parker (Eds.)Disorders of Affect Regulation: Alexithymia in Medical and Psychiatric Illness 1997 New YorkCambridge University Press:26-45.10.1017/CBO9780511526831.005 [Google Scholar] [CrossRef]
[15]. Kornreich C, Foisy ML, Philippot P, Dan B, Tecco J, Noel X, Impaired emotional facial expression recognition in alcoholics, opiate dependence subjects, methadone maintained subjects and mixed alcohol-opiate antecedents subjects compared with normal controlsPsychiatry Res 2003 119(3):251-60.10.1016/S0165-1781(03)00130-6 [Google Scholar] [CrossRef]
[16]. Thorberg FA, Young RM, Sullivan KA, Lyvers M, Connor JP, Feeney GF, Alexithymia, craving and attachment in a heavy drinking populationAddict Behav 2011 36(4):427-30.10.1016/j.addbeh.2010.12.01621215527 [Google Scholar] [CrossRef] [PubMed]
[17]. Lyvers M, Hinton R, Gotsis S, Roddy M, Edwards MS, Thorberg FA, Traits linked to executive and reward systems functioning in clients undergoing residential treatment for substance dependencePersonal Individ Diff 2014 70:194-99.10.1016/j.paid.2014.07.004 [Google Scholar] [CrossRef]
[18]. Evren C, Evren B, Dalbudak E, Ozcelik B, Oncu F, Childhood abuse and neglect as a risk factor for alexithymia in adult male substance dependent inpatientsJ Psychoactive Drugs 2009 41:85-92.10.1080/02791072.2009.1040067719455912 [Google Scholar] [CrossRef] [PubMed]
[19]. Dalbudak E, Evren C, Cetin T, Durkaya M, Cetin R, History of trauma and relationship with alexithymia, temperament and character dimensions in male alcohol dependent inpatientsJ Psych and Neurol Sciences 2010 23(1):01-12.10.5350/DAJPN2010230101 [Google Scholar] [CrossRef]
[20]. Ghogare AS, Saboo AV, A cross sectional study of cognitive impairment in patients of alcohol use disorder attending a tertiary health care center in Central IndiaAnn Indian Psychiatry 2019 3:155-60.10.4103/aip.aip_34_19 [Google Scholar] [CrossRef]
[21]. Stockwell T, Murphy D, Hodgson R, The severity of alcohol dependence questionnaire: Its use, reliability and validityBr J Addict 1983 78(2):145-55.10.1111/j.1360-0443.1983.tb05502.x6135435 [Google Scholar] [CrossRef] [PubMed]
[22]. Parker JD, Taylor GJ, Bagby M, The 20-item Toronto alexithymia scale III. Reliability and factorial validity in a community populationJ Psychosom Res 2003 55:269-75./10.1016/S0022-3999(02)00578-0 [Google Scholar] [CrossRef]
[23]. Parker JD, Keefer KV, Taylor GJ, Bagby RM, Latent structure of the alexithymia construct: A taxometric investigationPsychol Assess 2008 20(4):385-96.10.1037/a001426219086762 [Google Scholar] [CrossRef] [PubMed]
[24]. Taylor GJ, Parker JDA, Bagby RM, Bourke MP, Relationships between alexithymia and psychological characteristics associated with eating disordersJ Psychosom Res 1996 41(6):561-68.10.1016/S0022-3999(96)00224-3 [Google Scholar] [CrossRef]
[25]. Bernstein DP, Stein JA, Newcomb MD, Walker E, Pogge D, Ahluvalia T, Development and validation of a brief screening version of the Childhood Trauma QuestionnaireChild Abuse Negl 2003 27(2):169-90.10.1016/S0145-2134(02)00541-0 [Google Scholar] [CrossRef]
[26]. Bevilacqua L, Carli V, Sarchiapone M, George DK, Goldman D, Roy A, Interaction between FKBP5 and childhood trauma and risk of aggressive behaviourArch Gen Psychiatr 2012 69(1):62-70.10.1001/archgenpsychiatry.2011.15222213790 [Google Scholar] [CrossRef] [PubMed]