Vertigo is a subjective sensation of motion in which the individual or his/her surroundings seem to whirl dizzily [1]. In the community, 1 in 5 of the adult population has suffered such symptoms with 30% of these suffering for more than 5 years [2]. About 5-10% of patients seen in general OPD, and between 10-20 percent of the patients seen by otolaryngologists and neurologists are those with complaints pertaining to disequilibrium and vertigo [2]. Owing to overlapping symptoms and terms such as dizziness, light headedness, giddiness and presyncope, a proper diagnosis is often challenging. Such diagnostic dilemma may well be seen in routine ENT or vertigo clinics. Though vertigo patients are also seen by neurologists and general physicians, the Otolaryngologist’s perspective is focused on peripheral vertigo. Certain conditions like benign paroxysmal positional vertigo, Meniere’s disease, vestibular neuronitis are known common causes of peripheral vertigo in clinical practice [3]. Lesser common ones being labyrinthitis and acoustic neuroma. The aim of this study was to revisit the various aetiological factors for vertigo in patients in contemporary Otolaryngology practice so as to further streamline the concepts and existing knowledge.
Materials and Methods
A cross-sectional observational study was conducted under the Department of Otorhinolaryngology of a tertiary care teaching hospital, over a period of 12 months from March 2016 to March 2017. The study was carried out after taking due clearances from the Institutional Ethics and Research Committee (letter no. SRHU/HIMS/ETHICS/2017/144). Data was recorded as per proforma after obtaining written informed consent.
Inclusion criteria:
All patients complaining of sense of rotation of self or surroundings with at least one episode in preceding one month.
Patients who were more than 18 years of age.
Exclusion criteria:
Subjects with previous treatment history.
Subjects with severe cervical spine disease, known cerebro-vascular disease, previous neurological disorders, known cardiac ailments, underlying mental illnesses.
One-hundred and ten cases complaining of the sense of rotation of either self or their surroundings were recruited from the patients attending the Otorhinolaryngology department of the institute. A detailed history was obtained regarding the nature of symptoms, their onset, duration, frequency and other associated complaints. Severity of symptoms was graded as per Scale for Vestibular Vertigo Severity Level and Clinical Response Evaluation (SVVSLCRE) [4].
Sample size was calculated by estimation of proportion formula z pq/l2 where, z=95% confidence interval, p=50% (estimated prevalence 0.7-1.5%) [5]), q=1-p, l=20%.
Comprehensive otological and vestibular evaluation was done in all cases. Bed side clinical tests were done which included Dix hallpike, Fistula test, Head Impulse test, Spontaneous Nystagmus testing, Romberg’s test and Gait testing. Laboratory tests included Pure tone audiometry, Videonystagmography, Haemogram and random blood glucose levels. Though the focus of the authors was on peripheral vertigo, the cases who presented to the OPD after excluding the role of other specialities were hence included in the present study.
Data Analysis
Data was analysed using freely available software solutions (SPSS Version 22.00) and electronic spreadsheets (MS Excel) to store and manage the collected data. Descriptive analysis was done to determine means, frequencies and proportions of the various variables and findings were presented by means of graphs, tables and charts where appropriate. Chi-square test was used to assess any associations/relationships between outcomes i.e., aetiological diagnosis and variables such as presence or absence of postural variation.
Results
The mean age of patients in the study was 49.75 years with maximum patients in the age group of 41-50 years. The number of male and female patients was 55 each with male to female ratio of 1:1 [Table/Fig-1].
Demographic characteristics (n=110).
| Variable | Value |
|---|
| Age (Years) |
| Mean | 49.75 |
| Age groups (Years) |
| <20 | 2 (1.8%) |
| 21-30 | 14 (12.7%) |
| 31-40 | 14 (12.7%) |
| 41-50 | 30 (27.3%) |
| 51-60 | 22 (20.0%) |
| >60 | 28 (25.5%) |
| Sex |
| Male | 55 (50%) |
| Female | 55 (50%) |
Majority of the patients presented with acute onset of vertigo i.e., 99 (90%) patients. The total duration of symptoms most commonly observed ranged between one week to one month in 41 (37.3%) patients. Maximum patients 46 (41.8%) reported duration of each episode ranging between 1 minute to 10 minutes. Out of 110 patients, 109 patients reported with mild and moderate type of vertigo (Level II and III SVVSLCRE) i.e., it didn’t disrupt their day to day activities significantly. Only 1 patient (0.9%) reported with vertigo severe enough to hamper the daily activities (Level IV SVVSLCRE) [Table/Fig-2].
Characteristics of vertigo symptom (n=110).
| Vertigo | Numbers | % |
|---|
| Onset | Acute | 99 | 90.0% |
| Insidious | 11 | 10.0% |
| Total | 110 | 100% |
| Total duration of symptom | <1 week | 16 | 14.5% |
| 1 week-1 month | 41 | 37.3% |
| >1 month-6 months | 28 | 25.5% |
| 7 months-2 years | 14 | 12.7% |
| >2 years | 11 | 10.0% |
| Total | 110 | 100% |
| Duration of each episode | <1 minute | 26 | 23.6% |
| 1 minute-10 minute | 46 | 41.8% |
| 11 minute-1 hours | 21 | 19.1% |
| 2 hours-12 hours | 14 | 12.7% |
| >12 hours | 3 | 2.7% |
| Total | 110 | 100% |
| Intensity | Mild | 100 | 90.9% |
| Moderate | 9 | 8.2% |
| Severe | 1 | 0.9% |
| Total | 110 | 100% |
| Positional variation | Absent | 39 | 35.5% |
| Present | 71 | 64.5% |
| Total | 110 | 100% |
| Character | Continuous | 3 | 2.7% |
| Intermittent | 107 | 97.3% |
| Total | 110 | 100% |
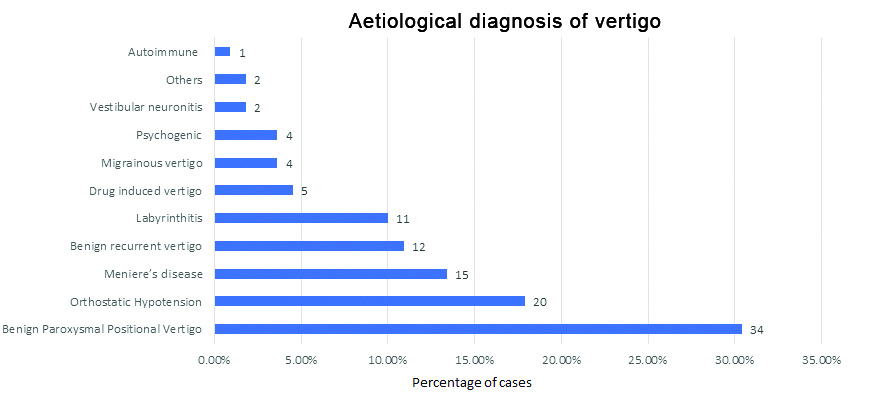
According to the study, most common aetiological diagnosis was BPPV which was observed in 34 (30%) patients followed by orthostatic hypotension which was observed in 20 patients [Table/Fig-3].
Aetiological diagnosis of vertigo (n=110).
In present study, BPPV was significantly associated with positional variation in vertigo. Out of 34 (30.9%) patients of BPPV, 18 (18.2%) patients had positional variation. This was followed by the patients of orthostatic hypotension i.e., out of 20 (18.2%) patients, 15 (13.6%) patients had positional variation. Positional variation was observed in all 12 (10.9%) patients of benign recurrent vertigo. There was a significant statistical association between positional variation and the patients with vertigo [Table/Fig-4].
Association between positional variation and aetiological diagnosis in vertigo patients. (n=110).
| Diagnosis | Positional variation | Total | *p-value |
|---|
| Absent | Present |
|---|
| BPPV | 14 (12.7%) | 18 (18.2%) | 34 (30.9%) | <0.001 |
| Orthostatic hypotension | 5 (4.5%) | 15 (13.6%) | 20 (18.2%) |
| Meniere’s disease | 10 (9.1%) | 5 (4.5%) | 15 (13.6%) |
| Labyrinthitis | 1 (0.9%) | 10 (9.1%) | 11 (10%) |
| Benign recurrent vertigo | 0 | 12 (10.9%) | 12 (10.9%) |
| Migrainous vertigo | 2 (1.8%) | 2 (1.8%) | 4 (3.6%) |
| Drug induced vertigo | 4 (3.6%) | 1 (0.9%) | 5 (4.5%) |
| Psychogenic | 1 (0.9%) | 3 (2.7%) | 4 (3.6%) |
| Vestibular neuronitis | 1 (0.9% | 1 (0.9%) | 2 (1.8%) |
| Others | 0 | 2 (1.8%) | 2 (1.8%) |
| Autoimmune | 1 (0.9%) | 0 | 1 (0.9%) |
| Total | 110 | 100% |
*Chi-square test; BPPV: Benign paroxysmal positional vertigo
Discussion
In present study of 110 patients, 99 (90%) patients reported acute onset of vertigo and 11 (10%) patients reported insidious onset of vertigo. This is explained by the fact that benign paroxysmal positional vertigo, labyrinthitis and Meniere’s disease contributed to majority of the cases. Maximum patients i.e., 46 (41.8%) reported duration of each episode ranging between 1 minute to 10 minutes. This again can be attributed to the fact that in the present study, the patients of benign paroxysmal positional vertigo, orthostatic hypotension and labyrinthitis constituted the majority. A major proportion (64.5%) reported a positional variation in their symptoms which was explained by benign paroxysmal positional vertigo and orthostatic hypotension as observed in previous study [6]. A study conducted by Jeon E et al., establishes a clear diagnostic significance of positional variation in benign paroxysmal positional vertigo and orthostatic hypotension [7]. One hundred and seven patients (97.3%) reported intermittent character of vertigo and only three patients (2.7%) reported a continuous vertigo. The likely cause of continuous vertigo was mainly attributed to vestibular neuronitis, drug induced (anti-epileptic medication) vertigo and Meniere’s disease [8,9]. Hypoglycaemia was excluded as having a causative role in present study. Three patients had deranged level of random blood glucose. The most common diagnosis observed in the study was benign paroxysmal positional vertigo (30.4%). This observation was similar to the study done by Neuhauser H and Lempert T who mentioned BPPV as the most frequent cause of dizziness [6]. Similar results were reported by Burman D et al., who also observed it as the most frequent cause of vertigo [8]. Patangay K et al., reported BPPV was the most frequent cause of vertigo amongst 205 cases. They diagnosed 43 cases of BPPV out of 205 cases i.e., 21% [9]. In another study by Bansal M, BPPV was the most common cause of vertigo [10]. Silva C et al., observed that head injury was associated with 10% of BPPV patients [11]. In index study, head injury was present in 7 patients of BPPV, thus contributing 24.2% of the cases. Orthostatic hypotension was the second most common cause of vertigo in our study with 17.9% patients. Jeon E et al., observed orthostatic hypotension as a major cause of orthostatic dizziness with prevalence of 9.8% [12]. In another study by Kim H et al., they found the patients had autonomic dysfunction (which was indicated by change in systolic blood pressure) as a cause of residual dizziness in BPPV patients [13]. Maarsingh OR et al., had reported presyncope as the most common subtype of dizziness comprising 67% of the patients [14]. In our study Meniere’s disease comprised 13.6% of the cases which was similar to Neuhauser H and Lempert T who observed 3 to 11% of the cases [6] and Burman D et al., who diagnosed 10.5% patients as those having Meniere’s disease [8]. However, Abrol R et al., observed it as a causative factor in only about 4% cases [5]. In present study, 10.9% cases were diagnosed with benign recurrent vertigo. Similar observations were made by Neuhauser H and Lempert T who described a strong relation of vertigo symptoms to benign recurrent vertigo, comprising 10% of the 208 cases [6]. In the present study, it was observed that 11 (10%) cases were diagnosed as labyrinthitis. Burman D et al., reported 7.4% cases [8] whereas, Bansal M observed only 3.12% cases diagnosed with labyrinthitis [10]. Whereas, Isaradisaikul S et al., described it as a lesser common diagnosis with labyrinthitis constituting just 0.7% of the cases evaluated by them [15]. In present study, four (3.6%) patients were diagnosed with migrainous vertigo. It is in accordance with the observations made by Bansal M where 3.12% patients were found to have similar diagnosis [10]. In the study by Neuhauser H and Lempert T they found a strong association between migraine and vertigo and it was the second most common cause of recurrent vertigo after BPPV [6]. Five patients (3.6%) in the study were diagnosed with drug induced vertigo. Two patients had history of intake of anti-tubercular drug (injectable Streptomycin). Another two patients had history of anti-epileptic drug (Carbamazepine) intake. One patient was on polydrug regimen consisting of oral hypoglycaemics and multivitamins for diabetes mellitus, diabetic neuropathy and chronic renal failure. In a study, conducted by Sanchez-Sellero I et al., out of 18 patients studied with drug induced vestibulotoxicity, three patients were on anti-tubercular drugs (ethambutol, streptomycin and isoniazid) [16]. In a study conducted by Ferreira L et al., anticonvulsant medication intake was associated with 2.25 times increased risk of dizziness [17]. In the present study, 3.6% patients were diagnosed with psychogenic vertigo. This was in spite of not having any previous underlying mental health condition. Bisdorff A et al., observed anxiety to be strongly related to symptoms of vertigo [18]. Two (1.9%) patients in the study were diagnosed with Vestibular Neuronitis which constituted as the ninth cause in order of frequency. This was in contrast with the study by Neuhauser H and Lempert T who observed it as the second most common cause of vertigo [6]. In another study by Burman D et al., it was observed that 6.4% patients were diagnosed with this condition [8]. The strength of the present study was that positional variation observed in the cases was not solely attributed to BPPV out rightly. A careful evaluation identified orthostatic hypotension as a causative factor in a good number of cases. Further studies are suggested to establish the true prevalence of this condition.
Limitation(s)
The cases in which no identifiable vestibular lesion could be established despite subjecting them to comprehensive vestibular examination and audio-vestibular tests.
Conclusion(s)
The most common aetiological factor of vertigo was found to be benign paroxysmal positional vertigo, which can be effectively treated by performing Epley’s maneuver and does not have other comorbid otological conditions. This was followed by orthostatic hypotension, which can be easily missed by otologists. Therefore, it should be kept as a possibility during work up of dizzy patients. Vertigo carries a large spectrum of aetiologies and hence should not be treated under a blanket regimen. The aetiological factors and diagnosis must be established in accordance with a meticulous clinical examination and investigations which should further guide the treatment strategy.
*Chi-square test; BPPV: Benign paroxysmal positional vertigo