Giant Intermuscular Thenar Lipoma: A Case Report and Literature Review
Prabhakar Ulaganathan1
1 Senior Civil Surgeon, Department of Plastic Surgery, Government District Headquarters Hospital, Kumbakonam, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Prabhakar Ulaganathan, 70, Jagannatha Pillayar Koil West Street, Kumbakonam, Tamil Nadu, India.
E-mail: druprabhakarplastic@gmail.com
Lipoma is the most common benign tumour in hand. Lipoma in hand of size more than 5 cm is classified as Giant Lipoma. Lipoma of larger sizes is rare in hand because of accessibility and lesser subcutaneous tissues. Large lipoma interferes in the hand functions. Lipoma in dominant hand is usually noted early and gets operated. This case is of 65 year old female patient who reported with the swelling in right hand for past 25 years. The size of the lipoma was big and asymptomatic till the presentation. The swelling was investigated and surgically removed which was diagnosed histopatholoically as Intermuscular Thenar Lipoma.
Soft tissue neoplasms, Thenar muscle, Thumb
Case Report
A 65-year-old female patient presented with complaints of swelling in the right hand for past 25 years. There were no complaints of pain or loss of function. It was slow growing and gradually increased to attain this size. There was no sensory neurological deficit in the thumb. She was able to do her personal work without any difficulty.
On examination, there was a well-defined lobular mass of size 8×7 cm occupying entire right thenar eminence. It was firm and non-mobile. Thumb movements were full. She was able to oppose the thumb to other fingers with difficulty but a firm grip could not be made [Table/Fig-1]. Clinical diagnosis of Lipoma was made.

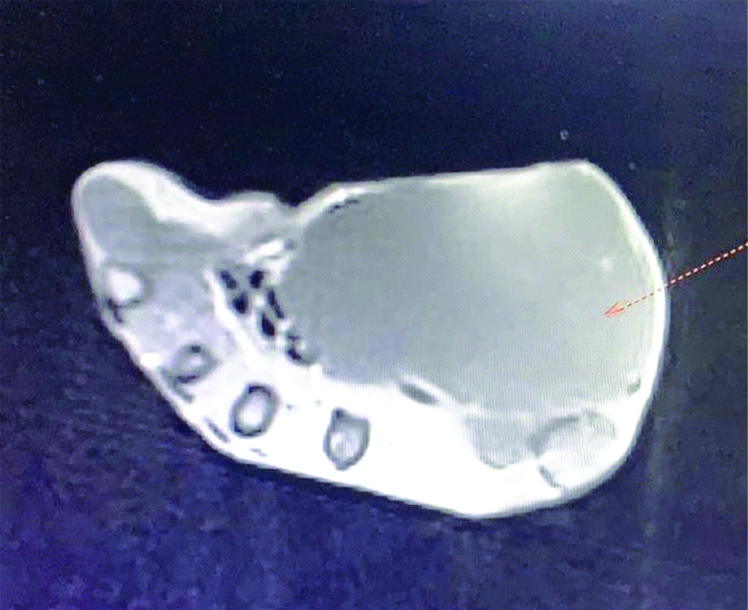
Blood investigations were within normal limits. MRI study of right hand was done. It showed features of large well-defined multi lobulated T2 and T1 hyper signal intense mass lesion of size 8.1×4.9×6.7 cm seen involving subcutaneous tissue in the palmar aspect and thenar eminence of right hand. Mass extended into the first interdigital space and was abutting the adjacent flexor tendon. There were no evidence of invasive features or sarcomatous degeneration or bony involvement [Table/Fig-2,3]. Fine Needle Aspiration Cytology was done to rule out the possibility of malignancy, the aspirate showed fat cells, fat droplets and fragments of mature adipose tissue suggestive of lipoma.
MRI of the hand showing the intense mass lesion of size 8.1×4.9×6.7 cm.

Surgical removal was planned as the tumour was big and interfered with her thumb movements. Surgery was done under supraclavicular block with tourniquet control. On exploration, a firm multi lobulated yellowish tumour found in between the thenar muscles. Flexor pollicis brevis muscle was found to be stretched. There was an indentation of tumour beneath that muscle [Table/Fig-4]. Thenar muscles were found atrophied and nerves were found stretched. Careful dissection using magnification was done to preserve the muscles and neurovascular pedicles [Table/Fig-5]. Excess skin was removed and wound was closed in layer after keeping suction drain [Table/Fig-6].
Lipoma stretching thenar muscle

Lipoma excision done preserving structures.


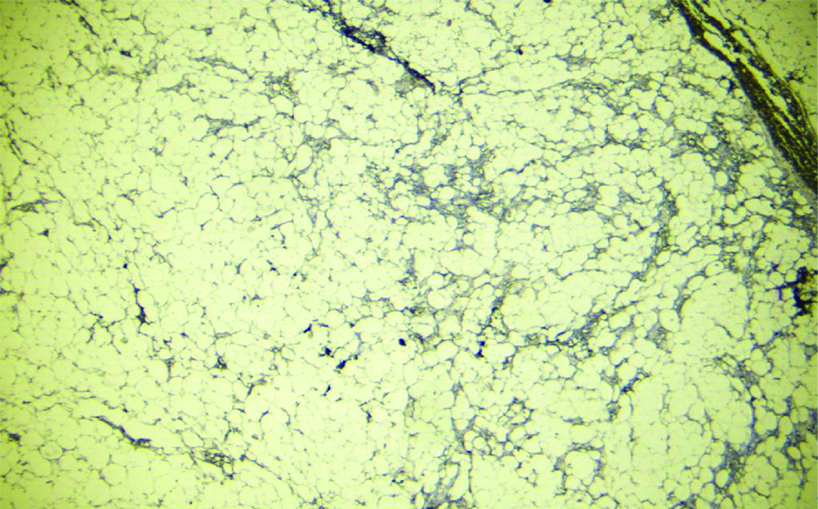
Specimen was sent for histopathological examination. The H&E stained multiple sections showed a benign mesenchymal neoplasm composed of lobules of fat cells separated by thin fibrous septa suggestive of Lipoma [Table/Fig-7]. Postoperatively, the thumb function was full and active with no neurovascular deficit. She was able to oppose the fingers without difficulty and able to make complete fist. Grip strength was also improved.
Histopathological features. (H&E 10X)
Discussion
Lipoma can arise in any part of body as fat is present everywhere. Hence, it is called as ubiquitous tumour or universal tumour. The aetiology is unclear. Genetic abnormalities are found in two-third of cases and possible causes are trauma, obesity, liver diseases, alcohol abuse. Lipoma is the most common soft tissue tumour of hand. Lipoma is either superficial or deep. Deep Lipoma is beneath the deep facia and subdivided into intermuscular and intramuscular. Intermuscular Lipoma is well encapsulated and expansile in growth. Intramuscular Lipoma is irregular and infiltrative in growth. Lipoma of hand more than 5 cm size is called as Giant Lipoma [1-3].
It is usually insidious in onset and slow to grow. Some patients may have symptoms of pain, paresthesia, sensory deficit, reduced range of movements, decreased grip strength, muscle paralysis, muscle atrophy and trigger finger [4,5]. Lipoma can interfere in finger movements, can be painful due to nerve entrapment and long standing lipoma can induce muscle atrophy and paralysis. Malignant changes can occur in large and intramuscular lipoma.
Differential diagnosis includes neurofibroma, sebaceous cyst and abscess, giant cell tumour of tendon sheath, haemangioma, fibroma, schwannoma, malignant fibrous histiocytoma, rhabdomyosarcoma and liposarcoma [6].
Lipomas are mostly asymptomatic and get operated for pain, fear of cancer, functional deformity and cosmetic reasons. Small asymptomatic lipoma may be left for observation. Ultrasound, CT scan and MRI are done to investigate. The location of the lipoma such as deep to fascia, its relation to the muscle like inter or intra muscular, infiltrative nature are the points to be noted during imaging study. Ultrasound is cost effective and non-ionising. The disadvantage of ultrasound is operator dependent and less useful in defining tissues. CT scan gives details like tumour infiltration, necrosis, and plane of tumour etc., with risk of radiation exposure. MRI gives better anatomical details especially about nerves, tendons etc., which will be useful during decision making and surgery [7]. The chances of malignancy are more when the size of Lipoma is more than 5 cm and intramuscular [8]. Hence, FNAC is useful for treatment planning as it gives pathological details. Adequate and representative sampling is must for arriving at the diagnosis.
According to Ivan Chernev and Amanda Norwood “many of the giant lipomas have well-differentiated liposarcomatous components, which are difficult to differentiate form their benign counterpart” [9]. Cytogenetic testing is useful in differentiating doubtful cases of lipoma from well-differentiated liposarcoma. Intramuscular lipoma is rare [10-12]. Lipoma was found to be of intermuscular type in this case. Many giant lipoma of hand up to a size of 12×10×8 cm (960 cc) is reported in literature [13]. Lipoma is rare in thenar muscles. It is recommended that lipoma of more than 4 cm size at thenar muscles should be considered as giant lipoma [14]. This is the largest intermuscular thenar lipoma, reported so far [Table/Fig-8] [3,6,15,16].
Giant Thenar Lipoma reported in literature [3,6,15,16].
| Case report | Year | Location | Size in cm | Volume in cc |
|---|
| Mohan L and Semoes J [15] | 2008 | Thenar | 5×5 | 125 |
| Yadav SP et al., [3] | 2013 | Thenar | 9.5×4.5×4 | 171 |
| Yildiran G et al., [6] | 2015 | Thenar | 5×3×2 | 30 |
| Cemboluk Ö et al., [16] | 2017 | Thenar | 2.5×5.9×6.2 | 91 |
| Present case | 2020 | Thenar | 8.1×4.9×6.7 | 266 |
Conclusion(s)
Size of the lipoma alone is not a major deciding factor for management of giant lipoma of the hand. Other features such as plane of the tumour, its relation to other structures and histological diagnosis are more important than size in planning the treatment. Bloodless surgical field by using tourniquet and careful dissection using magnification are important to achieve good results.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: May 07, 2020
Manual Googling: May 19, 2020
iThenticate Software: Aug 10, 2020 (10%)
[1]. Chatterton BD, Moores TS, Datta P, Smith KD, An exceptionally large giant lipoma of the handBMJ Case Rep [Internet] 2013 2013:bcr2013200206Available from: http://casereports.bmj.com/content/2013/bcr-2013-200206.abstract10.1136/bcr-2013-200206 [Google Scholar] [CrossRef]
[2]. Kim KS, Lee H, Lim DS, Hwang JH, Lee SY, Giant lipoma in the hand: A case reportMedicine (Baltimore) [Internet] 2019 98(52):e18434-34.Available from: https://pubmed.ncbi.nlm.nih.gov/3187672210.1097/MD.000000000001843431876722 [Google Scholar] [CrossRef] [PubMed]
[3]. Yadav SP, Jategaonkar PA, Haldar PJ, Giant hand lipoma revisited: Report of a thenar lipoma & its literature reviewJ Hand Microsurg [Internet] 2013 5(2):84-85.Available from: https://pubmed.ncbi.nlm.nih.gov/2442668210.1007/s12593-013-0093-324426682 [Google Scholar] [CrossRef] [PubMed]
[4]. Nadar MM, Bartoli CR, Kasdan ML, Lipomas of the hand: A review and 13 patient case seriesEplasty [Internet] 2010 10e66-66. Available from: https://pubmed.ncbi.nlm.nih.gov/21045920 [Google Scholar]
[5]. Cribb GL, Cool PW, Ford DJ, Mangham DC, Giant lipomatous tumours of the hand and forearmJ Hand Surg Am 2005 30(5):509-12.10.1016/j.jhsb.2005.05.00215992974 [Google Scholar] [CrossRef] [PubMed]
[6]. Yildiran G, Akdag O, Karamese M, Selimoglu MN, Tosun Z, Giant lipomas of the handHand Microsurg [Internet] 2015 4(1):8 LP-1110.5455/handmicrosurg.175443 [Google Scholar] [CrossRef]
[7]. Capelastegui A, Astigarraga E, Fernandez-Canton G, Saralegui I, Larena JA, Merino A, Masses and pseudomasses of the hand and wrist: MR findings in 134 casesSkeletal Radiol 1999 28(9):498-507.10.1007/s00256005055310525793 [Google Scholar] [CrossRef] [PubMed]
[8]. Rydholm A, Berg NO, Size, site and clinical incidence of lipoma. Factors in the differential diagnosis of lipoma and sarcomaActa Orthop Scand 1983 54(6):929-34.10.3109/174536783089929366670522 [Google Scholar] [CrossRef] [PubMed]
[9]. Chernev I, Norwood A, Re: Giant hand lipoma revisited: Report of a thenar lipoma and its literature reviewJ Hand Microsurg [Internet] 2014 6(2):113-14.Available from: https://pubmed.ncbi.nlm.nih.gov/2541456510.1007/s12593-014-0148-025414565 [Google Scholar] [CrossRef] [PubMed]
[10]. Lee YH, Jung JM, Baek GH, Chung MS, Intramuscular lipoma in thenar or hypothenar musclesHand Surg an Int J devoted to hand Up limb Surg Relat Res J Asia-Pacific Fed Soc Surg Hand 2004 9(1):49-54.10.1142/S021881040400200515368626 [Google Scholar] [CrossRef] [PubMed]
[11]. Papakostas T, Tsovilis AE, Pakos EE, Intramuscular lipoma of the thenar: A rare caseArch bone Jt Surg [Internet] 2016 4(1):80-82.Available from: https://pubmed.ncbi.nlm.nih.gov/26894225 [Google Scholar]
[12]. Berlund P, Kalamaras M, A case report of trigger wrist associated with carpal tunnel syndrome caused by an intramuscular lipomaHand Surg an Int J devoted to hand Up limb Surg Relat Res J Asia-Pacific Fed Soc Surg Hand 2014 19(2):237-39.10.1142/S021881041472017424875510 [Google Scholar] [CrossRef] [PubMed]
[13]. Lisenda L, van Deventer S, Pikor T, Lukhele M, Case report: Giant lipoma of the handSA Orthop J 2013 12(3):46-48. [Google Scholar]
[14]. Ayas MS, Okutan AE, Kerimoglu S, Giant thenar intramuscular lipoma; A literature review and redefinition of the term giant lipomaHand Microsurg 2019 8(1):44-50.10.5455/handmicrosurg.301881 [Google Scholar] [CrossRef]
[15]. Mohan L, Semoes J, Thenar intramuscular lipoma: An unusual caseInternet J Surg 2008 17(02):01-03.10.5580/1a67 [Google Scholar] [CrossRef]
[16]. Cemboluk Ö, Daldal İ, Topçu HN, Giant lipoma of the hand to extending from thenar region to deep palmar space: A case reportJ hum Rhythm 2017 3(4):212-15. [Google Scholar]