Infantile Epididymitis Presenting as Scrotal Swelling with Sinus in Paediatric Patient: A Case Report and Review of Literature
MD Mokarram Ali1, Amit Kumar2, Rashi3, Amit Kumar Sinha4, Bindey Kumar5
1 Senior Resident, Department of Paediatric Surgery, AIIMS, Patna, Bihar, India.
2 Senior Resident, Department of Paediatric Surgery, AIIMS, Patna, Bihar, India.
3 Senior Resident, Department of Paediatric Surgery, AIIMS, Patna, Bihar, India.
4 Associate Professor, Department of Paediatric Surgery, AIIMS, Patna, Bihar, India.
5 Professor, Department of Paediatric Surgery, AIIMS, Patna, Bihar, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Md Mokarram Ali, Department of Paediatric Surgery, Second Floor, OPD Building, AIIMS, Patna, Bihar, India.
E-mail: mohdmokarramali1990@gmail.com
Scrotal swelling with intermittent discharge and sinus is rare in paediatric age group. Among various differential diagnosis, Infantile Epididymitis is one possibility of scrotal swelling in infancy. Here, Authors reporting one such case of scrotal swelling in a four-year-old child which was present since three months of age. After failed initial medical management, swelling was excised which was reported as epididymitis in histopathological examination.
Scrotal sinus, Surgical management, Scrotum
Case Report
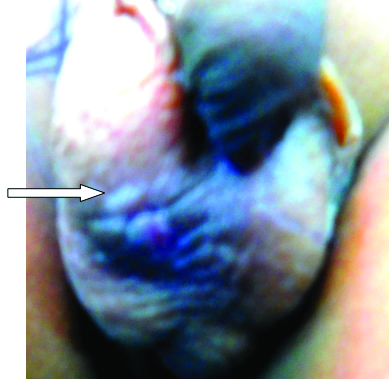
A four-year-old male child presented to the Outpatient Department with complaint of discharge from a swelling in right scrotum since last one year. According to mother, swelling was present in right scrotum since three months of age. Apart from swelling, there was no history of fever and pain in the swelling. There was no history of any trauma or incision and drainage. The patient had no urinary problems. The growth of the child was according to the age. Initially, there was no discharge from the swelling. The discharge from the swelling became apparent at three years of age which was initially purulent. Patient received oral antibiotics but condition did not improve. All symptoms were partially controlled with oral medications but swelling persisted and so was the discharge which became sero-purulent. On examination, the swelling was 3×3 cm, firm in consistency and overlying skin was indurated with a pin point sinus like opening [Table/Fig-1]. Swelling seemed fixed to testis and non tender. Bilateral testes were normal on examination.
Swelling over right hemiscrotum with visible sinus opening.
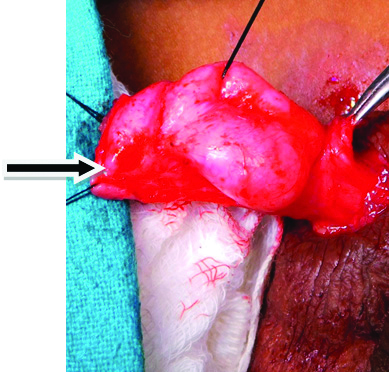
Patient was admitted and further evaluation was done. Routine blood investigations were in normal range. On ultrasonography of the scrotum, there was a hypodense area of 4×3 cm adjacent to epididymal head of right testis but free from the testis. A differential diagnosis of tubercular sinus was thought for which he was evaluated by Mantoux test which was negative. Due to persistence of the swelling and discharge, patient was taken for exploration and excision of swelling with sinus tract. On exploration, the swelling was seen arising from epididymis of right testis with sinus tract extending to the adjacent scrotal skin. Entire epididymis was found to be indurated. Testis was free from the lesion [Table/Fig-2,3]. The swelling along with sinus tract was excised with preservation of right testis and sent for histopathological examination. Postoperative period was uneventful and patient was discharged on postoperative day three. Histopathological examination of the tissue was suggestive of epididymitis. On follow-up at three months, there was no recurrence and wound healed satisfactorily.
Sinus tract visible separately from testes.

Sinus tract with endurated epididymis head.
Discussion
Infantile Epididymitis presenting as scrotal swelling with discharging sinus in children is a rare phenomenon. It has been reported with an incidence of approximately 2-7% in infancy [1]. Overall, scrotal swelling presenting as sinus is rarely seen in infancy.
The differential diagnosis of chronic scrotal swelling in this young age group can be hidradenitis suppurativa, tubercular or pyogenic epididymo-orchitis or scrotal abscess [2]. Two case reports of Amyand’s hernia presenting as chronic scrotal sinus have been reported [3,4]. It was diagnosed with ultrasound of inguinoscrotal area which showed inguinal hernia with bizarre congenital fistula. There is another case report of anorectal median raphe sinus in which patient presented as intermittent discharge from scrotum for two years [5]. Sinogram in this case revealed a sinus tract which was seen to be extending to the depth of scrotum without any internal communication. Incarcerated inguinal hernia may also present as a scrotal sinus [6]. In the present case, patient presented with scrotal swelling since three months of age with intermittent discharge, partially controlled by medication but recurred on stopping it. There was no history of abscess or tubercular contact. Bladder outlet obstruction as cause of epididymitis was ruled out as patient has no voiding difficulty and urinary stream was normal. Tuberculosis was ruled out by negative Mantoux test. Ultrasound revealed hypodense lesion arising from epididymis head of right testis. There was no evidence of incarcerated inguinal hernia in ultrasonography. During the surgery, swelling was seen to be located at the head of epididymis of right testis with thickening of spermatic cord with tract extending to adjacent scrotal skin. Right testis was normal. Biopsy of the tissue reported it as epididymitis.
Conclusion(s)
Infantile epididymitis presenting as discharging sinus is rare in paediatric age group. It may present as diagnostic dilemma and may wrongly be treated as abscess or tubercular lesion. Proper evaluation and treatment in these cases produce good results.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? NA
For any images presented appropriate consent has been obtained from the subjects. NA
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: May 07, 2020
Manual Googling: May 19, 2020
iThenticate Software: Aug 08, 2020 (14%)
[1]. Lewis AG, Bukowiski TP, Jarvis PD, Wacksman J, Sheldon CA, Evaluation of acute scrotum in the emergency departmentJ Pediatr Surg 1995 30:277-82./10.1016/0022-3468(95)90574-X [Google Scholar] [CrossRef]
[2]. Sah SP, Bhadani PP, Regmi R, Tewari A, Raj GA, Fine needle aspiration cytology of tubercular epididymitis and epididymo-orchitisActa Cytol 2006 50:243-49.10.1159/00032594916780016 [Google Scholar] [CrossRef] [PubMed]
[3]. Jain P, Mishra A, Amyand’s hernia presenting as chronic scrotal sinusJ Indian Assoc Pediatr Surg 2012 17:128-29.10.4103/0971-9261.9813422869981 [Google Scholar] [CrossRef] [PubMed]
[4]. Logan MT, Nottingham JM, Amyand’s hernia: A case report of an incarcerated and perforated appendix within an inguinal hernia and review of the literatureAm Surg 2001 67:628-29. [Google Scholar]
[5]. Pandey A, Verma R, Gupta V, Singh SP, Anoscrotal median raphe sinus in a childJ Cutan Aesthet Surg 2014 7:162-63.10.4103/0974-2077.14667125538438 [Google Scholar] [CrossRef] [PubMed]
[6]. Ameh EA, Awotula OP, Amoah JN, Spontaneous scrotal faecal fistula in infantsPediatr Surg Int 2002 18:524-25.10.1007/s00383-002-0754-y12415400 [Google Scholar] [CrossRef] [PubMed]