Case Report
Clinical Examination and Diagnosis
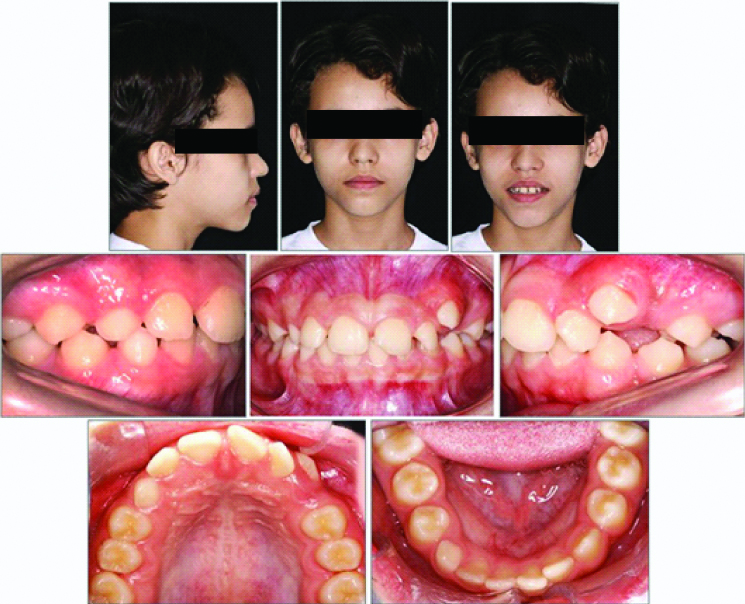
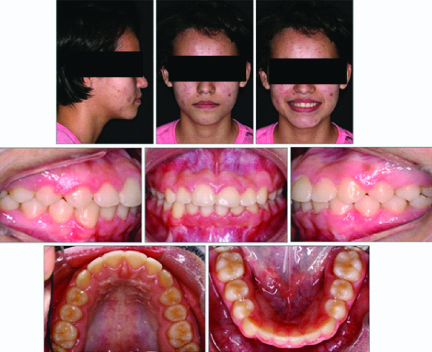
A 12-year-old girl came to the private practice orthodontic clinic in the city of Cascavel, Brazil with a chief complaint of prolonged retention of deciduous teeth, pointing to the maxillary and mandibular right deciduous canine. According to her medical history, she was healthy with no significant history. Patient had no history of dental trauma. She did not report any TMJ dysfunction or breathing problems. Extraorally, her face was well-balanced and symmetrical, but smiling revealed diastema and a malpositioned maxillary left canine. Intraorally, she had Angles Class I malocclusion in both sides with spacing issues in both arches, a rotated maxillary left central incisor, and ectopic maxillary left canine in buccal eruption. Her mandibular dental midline was shifted 2.0 mm to the right. Deep overbite and the overjet were within normal limits [Table/Fig-1].
Pretreatment facial and intraoral photographs.
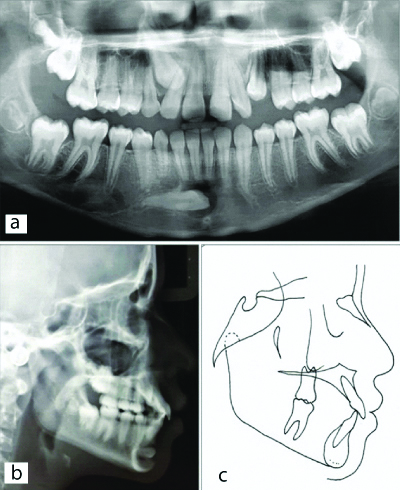
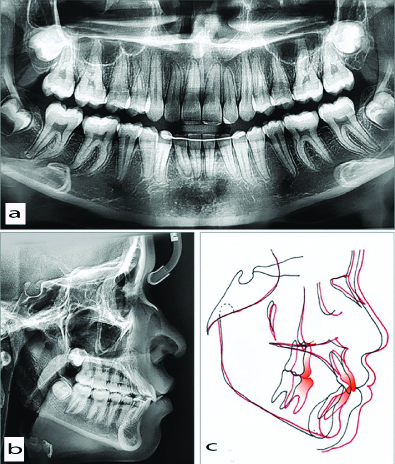
The panoramic radiograph depicted an impacted and a transmigrated mandibular right canine classified as type 2 according to Mupparapu M, where the canine is horizontally impacted near the inferior border of the mandible below the apices of the incisors, and no pathology associated, retention of the right maxillary and mandibular deciduous canine, and right maxillary permanent canine was impacted lacking space for eruption [1]. Radiographic evidence showed no sign of root resorption in the right mandibular lateral incisor, canine, and first premolar. The Steiner, Tweed and McNamara’s cephalometric measurements assessment were done and revealed a strong relationship between maxilla and mandible (ANB=2°), good vertical relationship (GoGn-SN=30°), FMA=26°, and Y-axis=60°). The maxillary (1-NA=7 mm, 1-NA=27°) and mandibular incisors (1-NB=5,0 mm, 1-NB=32°) were proclined [Table/Fig-2,3].
a) Pretreatment OrthoPantogram; b,c) Pretreatment lateral cephalogram.
Cephalometric measurements.
| Measurements | Norm | Prettreatment | Posttreatment | Follow-up |
|---|
| SNA angle (°) | 82° | 87 | 87 | 88 |
| SNB angle (°) | 80° | 85 | 87 | 87 |
| ANB angle (° | 2° | 2 | 0 | 1 |
| Facial angle (°) | 87° | 90 | 89 | 90 |
| Convexity (°) | 0° | 6 | 0 | 1 |
| FMA (°) | 25° | 26 | 22 | 23 |
| GoGn-SN) (°) | 32° | 30 | 26 | 28 |
| Y-Axis (°) | 59° | 60 | 59 | 59 |
| 1-NA (mm) | 4 | 7 | 8 | 7 |
| 1-NA (° | 22° | 27 | 34 | 28 |
| 1-NB (mm) | 4 | 5 | 6 | 7 |
| 1-NB (°) | 25° | 32 | 35 | 32 |
| IMPA (°) | 90° | 97 | 102 | 101 |
| Interincisal angle (°) | 132° | 119 | 112 | 118 |
| Z-angle (°) | 75° | 64 | 68 | 68 |
SNA angle: sella, nasion, A point; SNB angle: sella, nasion, B point; ANB angle: A point, nasion, B point; FMA: Frankfort-mandibular plane angle; IMPA: Incisor mandibular plane angle
Treatment Objectives
The treatment objectives were to move the mandibular right transmigrated canine and maxillary right canine into their ideal position in the arch with no harmful effects on the neighbouring teeth to maintain a Class I molar and canine relationships, correct the mandibular dental midline, correct the overbite, and achieve an aesthetic smile with minimal profile change.
Treatment Alternatives
Before initiating treatment, the following treatment alternatives were considered for the impacted and transmigrated right mandibular permanent canine:
No treatment is the condition in which deciduous canine was aesthetically acceptable and could be retained. Monitor and restore, when necessary, with a fixed prosthesis or an implant or transplantation after extraction of the mandibular right canine;
Conservative approach can be used by traction of the canine in its correct anatomic position using proper mechanics after performing a surgical exposition and employ bonding hooks or brackets for tractioning. Disadvantages of this option include a lengthy treatment time and chance of root resorption of neighboring teeth traction of the canine, as well as the possibility of ankylosis;
Extraction of the canine and closing the space completely by moving the posterior teeth. Treatment time would also be extended as a more rigorous anchorage would be necessary, making orthodontic mechanics difficult;
Extraction of the canine and moving the first and second premolar, opening space between the second premolar and first molar for implant-prosthesis rehabilitation after completion of growth.
Extraction of the canine and restoring it with an implant-based prosthesis. This would be needed after completion of growth. A provisional prosthesis would be indicated to maintain the space after the debonding and retention stage.
These cases serve as a challenge to the Orthodontist and patient because of the lack of certainty of the best treatment for each individual case. The patient and her parents did not want post-orthodontic restoration, so they opted for the second treatment plan. All risks, including the risk to achieve the desired outcome, the long and time-consuming treatment, and root resorption were explained to the patient and parents then signed the consent form.
Treatment Progress
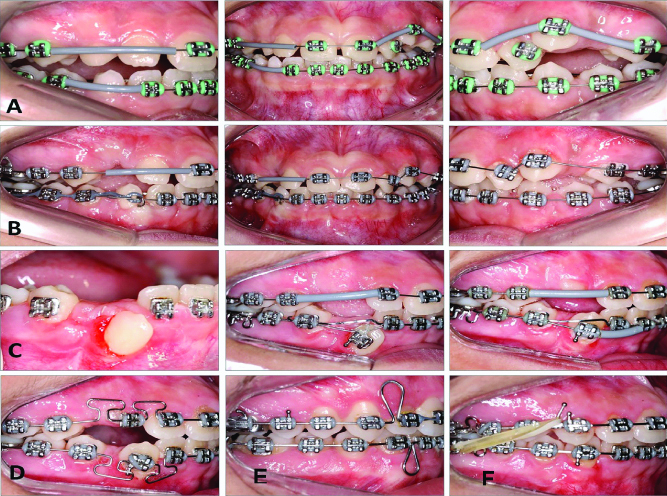
The treatment started with placement of a lingual holding arch on the mandibular first molars to maintain the arch perimeter. As soon as the alignment and leveling stage was completed, the patient was referred for surgery to bond the button on the transmigrated right mandibular canine with 0.010-in triple braided wire for traction. The right deciduous canine was extracted using lidocaine anaesthetic 3%, when the mandibular right canine was close to the deciduous canine. Afterwards, a Roth 0.022×0.028-in fixed appliance was placed in the maxillary and mandibular arches. The mandibular impacted canine erupted physiologically and it was moved distally to be positioned in the middle of the lateral incisor and first premolar by using elastic chains (3M Unitek). It was applied with the magnitude of 50 g/f and the posterior teeth were used as anchorage [Table/Fig-4]. Because the physiological eruption and the combination with the application of light force were the reason for the good gingival and periodontal results; A panoramic radiography [Table/Fig-5] exhibited spontaneous change of the maxillary right canine, and the uprighting of the mandibular canine was performed with elastic traction that was changed every 4 weeks. As soon as the mandibular canine erupted, the leveling began a 0.018×0.025-in stainless steel archwire was used to stabilise the adjacent teeth and an overlay with a NiTiarchwire (3M) was used to deliver light forces (60 g/f) to align and level the canine [Table/Fig-4a-c]. There was no way to be sure for the possibility of the canine ankylosis, but in every four weeks consultation, the leveling was observed.
Progress. A,B. Alignment and leveling of maxillary and mandibular arches. C. Exposition of the canine. D. Uprighting the mandibular right canine. E. Retraction archwires. F. Finishing archwires.
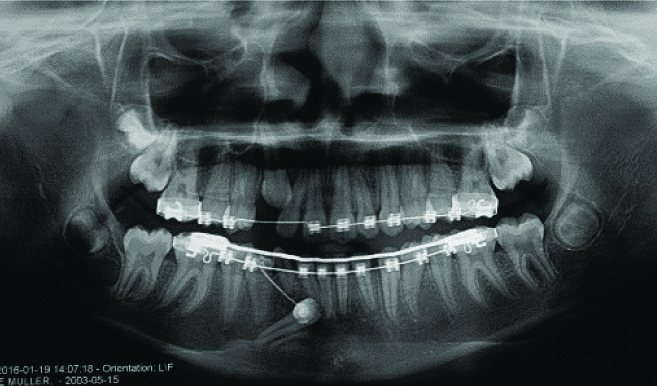
Progress panoramic radiography.
Direct buccal traction of the mandibular canine would apply pressure on the root of the lateral incisor distobuccally, so the transposed canine was initially retracted, taking care to prevent root interference expanding slightly the archwire in the canine region, before the canine was moved buccally into its ideal position.
After improving the leveling, around 0.018-in stainless steel double key loop archwire was used to correct the distal root inclination in both arches to extrude and upright both canines [Table/Fig-4d] followed by 0.019×0.026-in stainless steel archwire. Once the teeth were aligned and leveled, 0.019×0.026-in TP Orthodontics stainless steel archwires with teardrop loops were tied for retracting the anterior teeth [Table/Fig-4e]. After space closure, 0.019×0.025-in SS finishing arches with clipped hooks for Class II elastics were placed in order to achieve intercuspation of the maxillary and mandibular teeth [Table/Fig-4f]. At the conclusion of orthodontic treatment, braces were taken off. A maxillary Hawley and mandibular canine-to-canine bonded retainer were used for retention.
Treatment Results
After 3 years and 1 month, the impacted transmigrated mandibular canine was brought to its right position and had normal response to vitality test with less gingival recession.
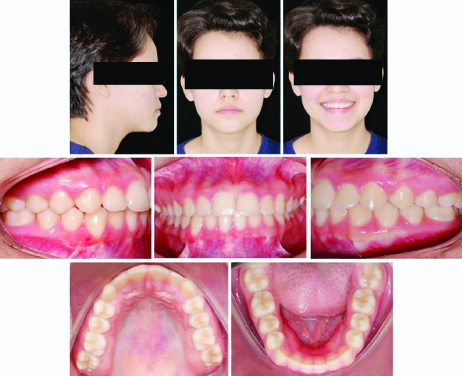
The post-treatment results demonstrated that the treatment goals were accomplished as indicated by a facial and intraoral photograph indicating good alignment, leveling, and dental midline correction. The torque control of the maxillary anterior teeth had improved the patient’s smile. Post-treatment intraoral photographs demonstrated inter-digitation of the teeth and a correct overjet and overbite with a coincidence of midlines [Table/Fig-6]. The mandibular right canine root inclination was buccally positioned based on the great initial inclination. At least 6 more months would be necessary to finish properly by moving the root lingually, but as per the patient’s request, the orthodontic appliance was removed without complete correction of the canine inclination [Table/Fig-6].
Post-treatment facial and intraoral photographs.
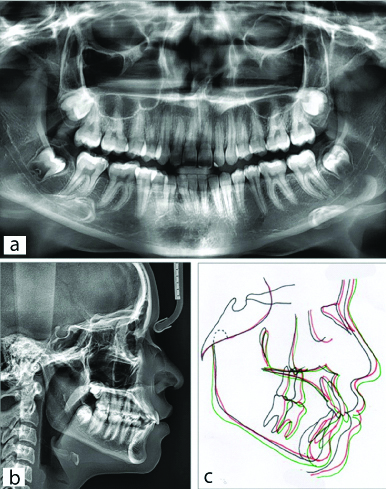
Post-treatment panoramic radiographs showed the optimal positioning of the right mandibular canine and maxillary teeth with proper root parallelism and a strong appearance of the ridges and trabecular bone. A cephalometric analysis revealed a well-balanced and harmonious facial profile [Table/Fig-3,7]. Superimposition showed no significant changes in skeletal measurements except for a reduction of ANB owing to mandibular growth, and a facial profile was maintained after treatment [Table/Fig-7b,c,8].
a) Post-treatment Orthopantogram, b) Post-treatment lateral cephalogram, c) Post-treatment cephalometric superimposition (black lines): before treatment; red lines: after treatment).
1.5-year follow-up facial and intraoral photographs.
At 1.5-year follow-up, the occlusion was well-maintained, and the repositioned transmigrated mandibular canine presented minimal gingival recession [Table/Fig-3,9]. Overall, superimpositions showed that the sagittal relationship between maxilla and mandible (ANB=1°, SNA=88°, SNB=87°) was maintained. The cephalometric measurements showed that the maxillary and mandible incisors remained virtually in the same position [Table/Fig-3,9].
a) 1.5 year follow-up Orthopantogram,b)1.5 year follow-up lateral cephalogram, c) 1.5 tear follow-up cephalometric superimposition (black lines: before treatment; red lines: after treatment; green lines: follow-up).
Discussion
The current clinical case described the treatment of a patient presenting with a horizontally impacted and transmigrated mandibular right canine and successfully treated with a fixed appliance. All advantages and disadvantages of the repositioning as well as the risks of being unable to achieve the desired goals along with the need for strong cooperation were discussed, and these were understood and accepted by the patient and their parents.
Transmigration of a mandibular canine has been associated with the presence of a retained primary canine on the affected side and higher prevalence of Angle’s Class I malocclusion [2], and most of the patients do not have any symptoms, and these canines are often discovered at the radiological examination before orthodontic treatment [3], characteristics similar to those of the present clinical case. The mandibular left canine is affected more often than the right and migrates more in females than males (1.6:1 ratio) [4]. Transmigration on the right side in a female patient is described here.
This clinical case was planned on an individual basis after taking into consideration the patient’s facial and dento-skeletal characteristics, the duration of treatment, risk factors involved, patient preferences, and the orthodontist’s experience as stated by Cavuoti S et al., and as a result of the unfavourable position and complexity of bringing the mandibular right canine into the arch [4], surgical extraction is the most common management [4,5]. Surgical removal, exposure and orthodontic alignment, intra-alveolar tooth transplantation (surgical repositioning of a tooth in its alveolar socket) and observation are viable treatment approaches [6].
In the present clinical case, the transmigrated mandibular right canine was horizontally impacted, crossing the midline, and the cusp tip was close to the lateral incisor with no associated cyst, as stated by Celikoglu M et al., with the deciduous canine aesthetically acceptable and could be kept, but the parents decided for extraction and perform the tractioning of transmigrated canine [7], in accordance with the conclusion of a systematic review that the orthodontic traction are the most commonly used treatment strategies [8].
Even though the literature recommends surgical removal when the canine has transmigrated, because root resorption of adjacent teeth is a common occurrence [8,9], the treatment to facilitate eruption was challenging because the 3D mechanical movement was difficult to plan and execute. Even though, in the present clinical case, the conservative approach was selected, moving the canine a substantial distance from its original position based on patient age and occlusion, stage of the canine’s root development, position of the canine, relationship between the canine and adjacent teeth, and mainly on the patient’s and her parents’ wishes.
There are no clear guidelines for successful management of repositioned canines based on their position or location and in the present clinical case, although it was difficult to orthodontically traction it into a normal position the results were favourable, in agreement with, Wertz RA to move it into the line of occlusion [10], applying a number of mechanics devised to recover impacted maxillary canines into occlusion [11]. The biomechanics applied in the present clinical case delivered light forces. The double key loop archwire was not fully inserted into the bracket slot with the objective of obtaining the final alignment and leveling of the tooth, but rather, progressively, consultation to consultation. The tear drop loop was used to completely close the space and for anterior teeth retraction.
When the transmigrated canine was moving toward the occlusion line, the canine required individualised torque bend. For a perfect positioning, more six months would be required for moving the root lingually, but the parents were satisfied with the results. The Jiang Q et al., approach could be applied here by bonding auxiliary brackets and wire at the gingival one-third area of the 3 adjacent teeth to maximise the torque as this has shown to be clinically effective featuring efficient torque control [12].
In a similar case, Plaza SP concluded that a transmigrated canine treatment by orthodontic traction is a challenge to the clinician, but it was possible to perform it successfully, as presented in this case report [11]. Although treatment time was long with proper biomechanics, the adverse effects were minimised or avoided and the best results were achieved even without using mini-implants.
The outcome presented in this clinical case was satisfying for the doctors and praised by the parents and the patient. The endeavor to do the treatment was worth it for the successful tractioning of a transmigrated and angulated mandibular right canine with a 1.5-year follow-up stability. The success of the treatment was governed by light forces and motivating the patient.
Conclusion(s)
The biomechanics applied for the treatment of an impacted and transmigrated mandibular right canine had a long pathway with no negative effects (such as root resorption or periodontal problems). Excellent results were yielded, both aesthetically and functionally, with stability at 1.5-years follow-up.
[1]. Mupparapu M, Patterns of intra-osseous transmigration and ectopic eruption of mandibular canines: Review of literature and report of nine additional casesDentomaxillofac Radiol 2002 31(6):355-60.10.1038/sj.dmfr.460073212424633 [Google Scholar] [CrossRef] [PubMed]
[2]. Plakwicz P, Abramczyk J, Wojtaszek-Lis J, Sajkowska J, Warych B, Gawron K, The retrospective study of 93 patients with transmigration of mandibular canine and a comparative analysis with a control groupEur J Orthod 2019 41(4):390-96.10.1093/ejo/cjy06730295778 [Google Scholar] [CrossRef] [PubMed]
[3]. Joshi MR, Transmigrant mandibular canines: A record of 28 cases and a retrospective review of the literatureAngle Orthod 2001 71(1):12-22. [Google Scholar]
[4]. Cavuoti S, Matarese G, Isola G, Abdolreza J, Femiano F, Perillo L, Combined orthodontic-surgical management of a transmigrated mandibular canineAngle Orthod 2016 86(4):681-91.10.2319/050615-309.126502299 [Google Scholar] [CrossRef] [PubMed]
[5]. Janakiraman N, Vaziri H, Safavi K, Nanda R, Uribe F, Management of severely impacted mandibular canines and congenitally missing mandibular premolars with protraction of autotransplanted maxillary premolarAm J Orthod Dentofacial Orthop 2016 150(2):339-51.10.1016/j.ajodo.2015.08.02227476368 [Google Scholar] [CrossRef] [PubMed]
[6]. Verma SL, Sharma VP, Singh GP, Management of a transmigrated mandibular canineJ Orthod Sci 2012 1(1):23-28.10.4103/2278-0203.9477824987621 [Google Scholar] [CrossRef] [PubMed]
[7]. Celikoglu M, Kamak H, Oktay H, Investigation of transmigrated and impacted maxillary and mandibular canine teeth in an orthodontic patient populationJ Oral Maxillofac Surg 2010 68(5):1001-06.10.1016/j.joms.2009.09.00620188449 [Google Scholar] [CrossRef] [PubMed]
[8]. Dalessandri D, Parrini S, Rubiano R, Gallone D, Migliorati M, Impacted and transmigrant mandibular canines incidence, aetiology, and treatment: A systematic reviewEur J Orthod 2017 39(2):161-69.10.1093/ejo/cjw02727036134 [Google Scholar] [CrossRef] [PubMed]
[9]. Bertl MH, Frey C, Bertl K, Giannis K, Gahleitner A, Strbac GD, Impacted and transmigrated mandibular canines: An analysis of 3D radiographic imaging dataClin Oral Investig 2018 22(6):2389-99.10.1007/s00784-018-2342-029392413 [Google Scholar] [CrossRef] [PubMed]
[10]. Wertz RA, Treatment of transmigrated mandibular caninesAm J Orthod Dentofacial Orthop 1994 106(4):419-27.10.1016/S0889-5406(94)70064-8 [Google Scholar] [CrossRef]
[11]. Plaza SP, Orthodontic traction of a transmigrated mandibular canine using mini-implant: A case report and reviewJ Orthod 2016 43(4):314-21.10.1080/14653125.2016.122453927805872 [Google Scholar] [CrossRef] [PubMed]
[12]. Jiang Q, Yang R, Mei L, Ma Q, Wu T, Li H, A novel approach of torque control for maxillary displaced incisorsAm J Orthod Dentofacial Orthop 2019 155(6):860-70.10.1016/j.ajodo.2017.11.04531153507 [Google Scholar] [CrossRef] [PubMed]