Lagophthalmos- A Rare Presenting Sign in a Case of Childhood Pontine Glioma
N Gayathri1, G Premnath2, S Kiruthika3, Manoj Vasudevan4, Geeta Anusha Loya5
1 Senior Resident, Department of Ophthalmology, Chettinad Academy of Research and Education, Chennai, Tamil Nadu, India.
2 Associate Professor, Department of Ophthalmology, Chettinad Academy of Research and Education, Chennai, Tamil Nadu, India.
3 Senior Resident, Department of Ophthalmology, Chettinad Academy of Research and Education, Chennai, Tamil Nadu, India.
4 Director and Senior Consultant, Department of Ophthalmology, Janu’s Eye Clinic, Chennai, Tamil Nadu, India.
5 Postgraduate, Department of Ophthalmology, Chettinad Academy of Research and Education, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: G Premnath, Associate Professor, Department of Ophthalmology, Chettinad Academy of Research and Education, Kelambakkam, Chennai-603103, Tamil Nadu, India.
E-mail: drpremn18@yahoo.co.in
Brain stem glioma is a rare central nervous system tumour arising from glial cells which occur mostly in children. Diffuse Intrinsic Pontine Gliomas (DIPG) and Focal glioma are the two types of pontine glioma. DIPGs are highly aggressive. The clinical features are not the same in every child. It commonly has a grave prognosis as most children die within 18 months of diagnosis. Hereby, Authors present a case of 10-year-old male child complaining of watering from the left eye for four days. There was no history suggesting involvement of any other cranial nerves and there was no episode of any seizure or similar history. On examination patient was found to have left lagophthalmos. Magnetic Resonance Imaging (MRI) of brain showed features of pontine glioma with mass effect. To prevent exposure keratopathy, the child was started on lubricating drops/gel and lid taping and referred immediately to a cancer centre for further management. Patients with pontine gliomas usually complain of gait disturbance, headache, limb weakness and double vision. To Authors’ knowledge no other documented case has presented with lagophthalmos. This case is presented for the rarity of the presenting symptom and to stress the importance of picking early ophthalmic signs.
Childhood brain tumours, Eye watering, Ophthalmic sign
Case Report
A 10-year-old male child presented with complaints of watering from his left eye since the past four days. He had no associated history of double vision, headache, hearing loss, fever, facial asymmetry and difficulty in swallowing or speech. There was no episode of any seizure or similar complaints reported in the past.
On examination, his visual acuity was 6/6 in both the eyes and intra ocular pressure was within normal limits. Hirschberg’s test revealed orthophoria and extra ocular movements were full and free and a horizontal gaze nystagmus was noted in primary position. Left eye demonstrated lagophthalmos with good Bell’s phenomenon and no corneal exposure [Table/Fig-1]. Corneal sensations were not reduced. Direct and consensual pupillary reflexes were normal. Dilated fundus examination was normal with no evidence of papilloedema. Right eye was normal.

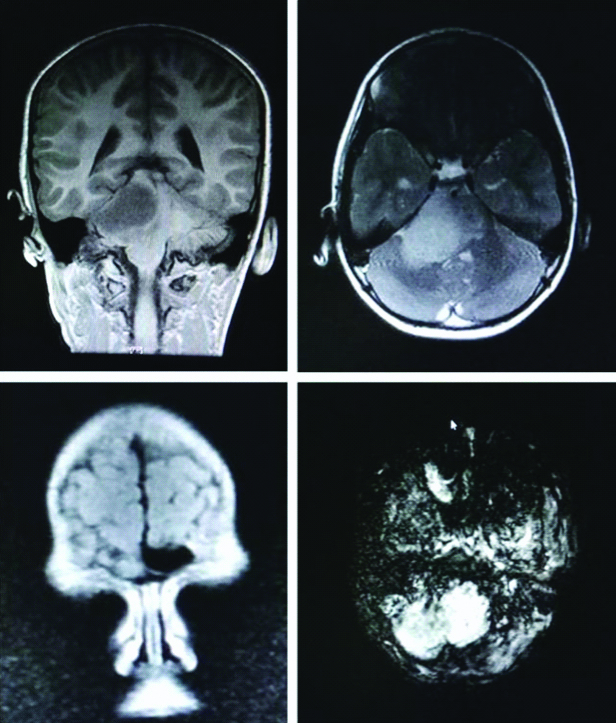
Expert opinions from a paediatrician and a neurologist were obtained. Neurologist reported a Glasgow Coma Scale (GCS) of 15/15 and no demonstrable facial nerve palsy except lagophthalmos. Also, the plantar reflexes were extensor bilaterally. After three days the patient developed left sided ataxic gait. He was advised for MRI of the brain [Table/Fig-2] which showed a fairly defined, T2 hyperintense lesion measuring 39×39×33 mm centered at right paramedian aspect of pons causing distortion and partial effacement of fourth ventricle and mass effect over the tip of cerebellar tonsil.
MRI showing T2 hyperintense lesion at right paramedian aspect of pons.
As a prophylactic measure for corneal exposure keratopathy, the patient was started on lubricating eye drops and eye gel at night followed by lid taping and was referred to a cancer centre for further management. Inspite of early referral the child succumbed to the disease after three months of external beam radiation.
Discussion
Brain stem gliomas are tumours formed from glial cells which affect the midbrain, pons and medulla. They comprise 10% of all childhood brain tumours, the usual age of presentation being 14 years of age [1]. Around 75-80% of the tumours are located in the pons [1,2]. As the brain stem controls vital functions such as respiration, heart rate, blood pressure, the nerves and muscles; signs and symptoms depend on where the tumour is located in the brain stem; its size and its rapidity in growth. Brain stem gliomas are of two types. Most common are DIPGs which occur in childhood and they arise from pons [3]. Focal gliomas form in the other parts of the brain stem. DIPG is considered the most severe childhood tumour with no remarkable progress in treatment in last five decades [4].
DIPG has grave prognosis when compared with focal gliomas. Pontine glioma patients usually report with the classic triad of cranial nerve palsies, long tract signs and ataxia [2]. Among cranial nerves sixth and seventh nerves are most commonly affected [2], but often overlooked in children. Lachi PK et al., studied 48 children and Laghari AA et al., studied 18 children but none of them presented with lagophthalmos [5,6]. One study found that brain stem glioma patients present with gait disturbance (61%), headache (44%), weakness of the limbs (42%), and diplopia (10%) [5]. Das S had reported a case with sixth nerve palsy as the presenting sign [7]. None of them had presented with lagophthalmos. PubMed search for lagophthalmos as a presenting sign in pontine gliomas revealed no results.
The case primarily presented at the ophthalmology clinic with watering, on skillful examination revealed lagophthalmos. In such cases, careful evaluation with MRI of the brain at the earliest [8,9] can identify the tumour and early diagnosis is an important prognostic factor. The radiologic features of DIPG vary from case to case. They can be expansible masses with no enhancement or necrosis and surrounding infiltrative growth or central necrosis and peripherally enhancing masses with significant mass effect but minimal surrounding T2/FLAIR hyperintensity [10]. Conditions such as acute demyelinating encephalomyelitis, tuberous sclerosis, neurofibromatosis type I, Langerhan cell histiocytosis, hamartoma, medulloblastoma and ependymoma should be considered as radiological differential diagnosis. Low grade brain stem gliomas are effectively managed by external beam radiotherapy [11], however high grade tumours result in high fatality [12]. Surgical excision and chemotherapy have been found to have fewer roles.
Conclusion(s)
Childhood mid brain gliomas are rare brain tumours with a poor survival rate with lagophthalmos being one of the rarest presentations. This case is presented for the rarity of the presenting symptom and to stress the importance of picking early ophthalmic signs. ‘Eyes are the window of the central nervous system’ is once again proved.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: May 05, 2020
Manual Googling: May 14, 2020
iThenticate Software: Jul 31, 2020 (6%)
[1]. Ueoka DI, Nogueira J, Campos JC, Maranhäo Filho P, Ferman S, Lima MA, Brainstem gliomas-Retrospective analysis of 86 patientsJ Neurol Sci 2009 281(1-2):20-23.10.1016/j.jns.2009.03.00919345380 [Google Scholar] [CrossRef] [PubMed]
[2]. Hennika T, Becher OJ, Diffuse intrinsic pontine glioma: Time for cautios optimismJ Child Neurol 2016 31:1377-85.10.1177/088307381560149526374787 [Google Scholar] [CrossRef] [PubMed]
[3]. Donaldson SS, Laningham F, Fisher PG, Advances toward an understanding of brainstem gliomasJ Clin Oncol 2006 24:1266-72.10.1200/JCO.2005.04.659916525181 [Google Scholar] [CrossRef] [PubMed]
[4]. Castel D, Philippe C, Calmon R, Le Dret L, Truffaux N, Boddaert N, Histone H3F3A and HIST1H3B K27M mutations define two subgroups of diffuse intrinsic pontine gliomas with different prognosis and phenotypesActa Neuropathol 2015 130:815-27.10.1007/s00401-015-1478-026399631 [Google Scholar] [CrossRef] [PubMed]
[5]. Lachi PK, Irrakula M, Ahmed SF, Joseph D, Pamidighantam S, Rao Naidu KVJ, Clinical profile and outcomes in brainstem glioma: An institutional experienceAsian J Neurosurg 2015 10(4):298-302.10.4103/1793-5482.16270926425160 [Google Scholar] [CrossRef] [PubMed]
[6]. Laghari AA, Baig MZ, Bari E, Darbar A, Mushtaq N, Abdullah UEH, Pediatric brainstem gliomas: An institutional experienceAsian J Neurosurg 2019 14(4):1144-50.10.4103/ajns.AJNS_101_1931903354 [Google Scholar] [CrossRef] [PubMed]
[7]. Das S, Sixth nerve palsy-Window to a dreaded brain tumour in children (pontine glioma)Kerala J Ophthalmol 2017 29:247-49.10.4103/kjo.kjo_69_17 [Google Scholar] [CrossRef]
[8]. Fisher PG, Breiter SN, Carson BS, Wharam MD, Williams JA, Weingart JD, A clinicopathologic reappraisal of brain stem tumour classification. Identification of pilocystic astrocytoma and fibrillary astrocytoma as distinct entitiesCancer 2000 89:1569-76.10.1002/1097-0142(20001001)89:7<1569::AID-CNCR22>3.0.CO;2-0 [Google Scholar] [CrossRef]
[9]. Wietelmann D, Schumacher M, Muendel J, Hirnstammgliom. Brain stem gliomaRadiologe 1998 38(11):904-12.10.1007/s0011700504419861650 [Google Scholar] [CrossRef] [PubMed]
[10]. Aboian MS, Solomon DA, Felton E, Mabray MC, Villanueva-Meyer JE, Mueller S, Imaging characteristics of pediatric diffuse midline gliomas with histone H3 K27M mutationAJNR Am J Neuroradiol 2017 38(4):795-800.10.3174/ajnr.A507628183840 [Google Scholar] [CrossRef] [PubMed]
[11]. Brower JV, Indelicato DJ, Aldana PR, Sandler E, Rotondo R, Mendenhall NP, A treatment planning comparison of highly conformal radiation therapy for pediatric low-grade brainstem gliomasActa Oncol 2013 52(3):594-99.10.3109/0284186X.2013.76747423421953 [Google Scholar] [CrossRef] [PubMed]
[12]. Edwards MS, Prados M, Current management of brain stem gliomasPediatr Neurosci 1987 13:309-15.10.1159/0001203493332719 [Google Scholar] [CrossRef] [PubMed]