Bilateral Accessory Central Cusp on Permanent Mandibular Second Molars: An Unusual Occurrence
Paras Mull Gehlot1, Jumana Haseen2, Veena Jayadevan3, BM Annapoorna4
1 Reader, Department of Conservative Dentistry and Endodontics, JSS Dental College and Hospital, JSS Academy of Higher Education and Research, Mysore, Karnataka, India.
2 Postgraduate Student, Department of Conservative Dentistry and Endodontics, JSS Dental College and Hospital, JSS Academy of Higher Education and Research, Mysore, Karnataka, India.
3 Postgraduate Student, Department of Conservative Dentistry and Endodontics, JSS Dental College and Hospital, JSS Academy of Higher Education and Research, Mysore, Karnataka, India.
4 Professor and Head, Department of Conservative Dentistry and Endodontics, JSS Dental College and Hospital, JSS Academy of Higher Education and Research, Mysore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Paras Mull Gehlot, Reader, Department of Conservative Dentistry and Endodontics, JSS Dental College and Hospital, JSS Academy of Higher Education and Research, S S Nagara, Mysore, Karnataka, India.
E-mail: dr.parasmullj@jssuni.edu.in
Anomaly like central cusp is accessory cusp which is similar to Dens Evaginatus (DE) in premolars. Such accessory occlusal/central cusps are rarely being reported in mandibular molars. The presence of these structures can be a cause of concern when they interfere with occlusion, get fractured or pulp is exposed. This report presents an unusual case of 21-year-old male patient with bilateral accessory cusp in permanent mandibular second molars, the left with Occlusal central cusp (7-cusp anatomy) and the right with a prominent expression of tuberculum sextum (5-cusp anatomy). The patient reported with sensitivity on lower left second molar. Radiograph did not reveal any pulpal extension in both the teeth. Buccal caries on left second molar was restored with composite resin and the accessory cusp was incrementally grinded. The patient reported on follow-up visit after 6 months and was asymptomatic. Early identification of supernumery occlusal central cusp and proper treatment can avoid pulpal complications.
Anomaly, Dens evaginatus, Supernumerary, Tuberculum sextum
Case Report
A 21-year-old male patient reported to the Department of Conservative Dentistry and Endodontics, with a chief complaint of sensitivity and food lodgement in lower left side of the jaw for two weeks. The patient was well built and had no history of congenital anomalies or medical problems. Family history was not significant. Intraoral examination revealed hypoplastic carious mandibular left first premolar (#34) with proximal caries. The right mandibular second molar (#47) exhibited large cusp extending from distal margin ridge to the centre of occlusal surface. Deep buccal pit caries was noted on the left mandibular second molar. Further, it was noted that the left mandibular second molar (#37) exhibited prominent supernumery occlusal cusp [Table/Fig-1a-c] and these occlusal cusps were separated from the remaining cusps by deep developmental grooves. Teeth were nontender on percussion and responded normal to vitality tests.
Clinical features of various cusps [1].
Intraoral view: (a) #47 with prominent occlusal cusp on right mandibular second molar; (b) Mandibular occlusal view with bilateral occlusal accessory cusps on second molars; (c) #37 with occlusal central cusp and tuberculum intermediate,\ buccal pit deep caries; (d) #47, Intraoral periapical radiograph; (e) #37, Intraoral periapical radiograph; (f) Buccal pit restored with composite resin
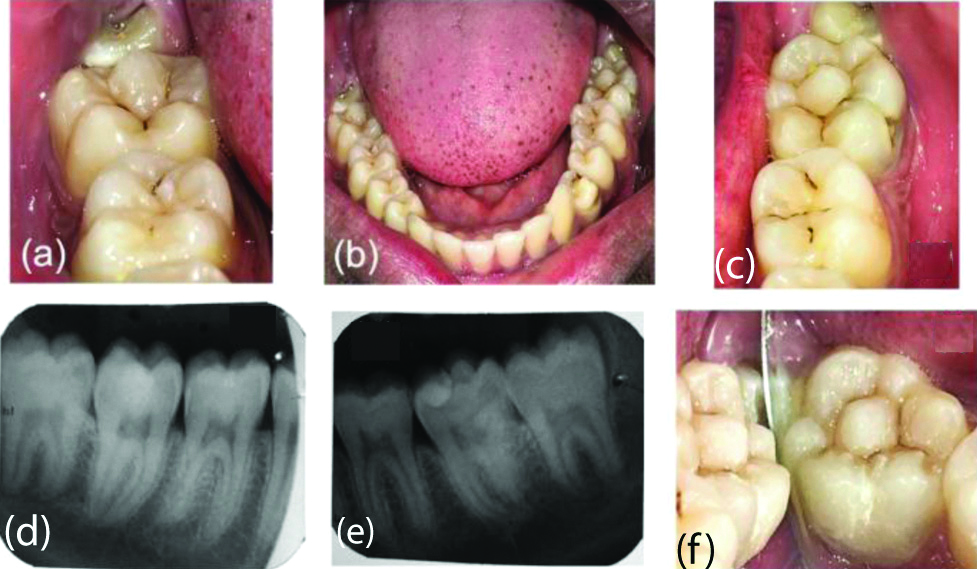
Intraoral periapical radiograph did not show any extension of pulp into the accessory cusps for both the teeth. An radio-opacity in the centre of the crown occlusally was noted for left mandibular second molar and two separate roots were also noted distally [Table/Fig-1d-e].
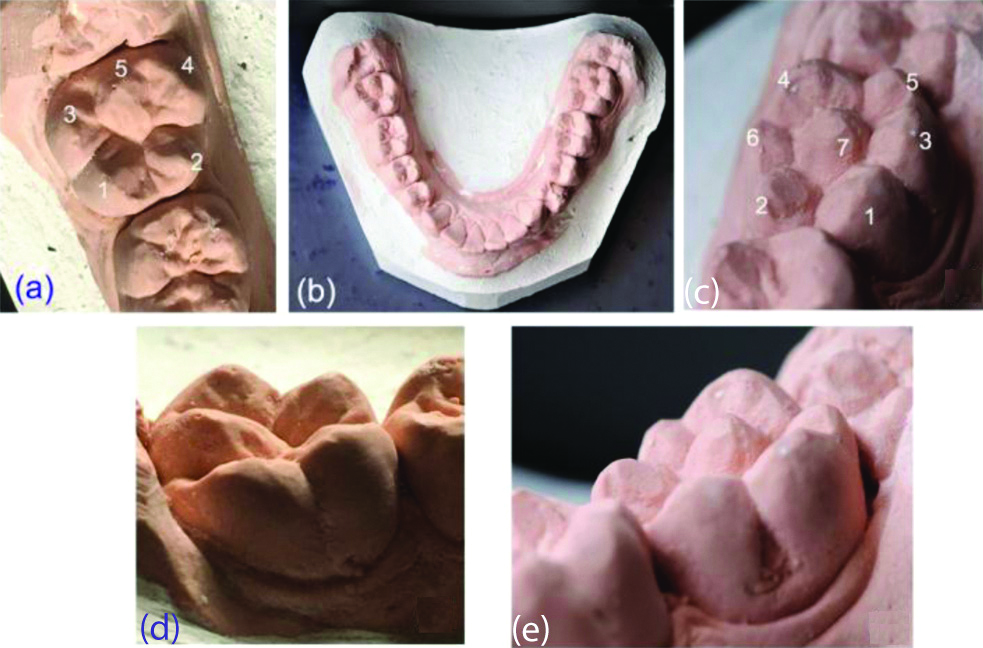
Details of the various cusps are presented in a [Table/Fig-2] [1]. Cast were made with dental stone (Kalabhai Karson Pvt., Ltd., Mumbai, India). The dimensions of the accessory cusps were recorded with a digital Caliper (CD-6” CSX, Mitutoyo Corp., Kawasaki, Japan). The central cusp on left mandibular second molar (#37) had a rhomboid base with tip slightly lower than the distolingual cusp, but 1 mm above the level of the remaining cusps [Table/Fig-3a-e]. This led to malocclusion and open bite [Table/Fig-4]. On mandibular right second molar (#47), the distal cusp (Cusp 5) was higher than all the other cusps. The cusp tips had evidence of mild attrition.
Details of the various cusps [1].
| Tooth | Cusp numbers and names | Details of accessory cusp |
|---|
| Lower left second molar (# 37)(Total Cusps: 7)[Table/Fig-1c,3c,3e] | Buccal cusps(1) Mesiobuccal (Protoconid)(3) Distobuccal (Hypoconid)(5) Distal (Hypoconulid)Lingual cusps(2) Mesiolingual (Metaconid)(4) Distolingual (Entoconid), and(6) Tuberculum intermedium (metaconulid) | (7) Central cusp located as a prominent elevation in the centre, separated from buccal and lingual cusps by development grooves.• Dimension:Width 4.5 mm × 5 mmHeight 4 mm• Surface smooth• Type 5 (Schulze) |
| Lower right second molar (#47)(Total Cusps: 5)[Table/Fig-1a,3a,3d] | Buccal cusps(1) Mesiobuccal (Protoconid)(3) Distobuccal (Hypoconid)Lingual cusps(2) Mesiolingual (metaconid)(4) Distolingual (entoconid) | (5) Tuberculum sextum or entoconulid located on the distal marginal ridge separated from distobuccal and distolingual cusps by development grooves.• Dimension:Width 6 mm × 4.5 mmHeight 5 mm• Surface smooth |
Cast model of mandibular arch (a) Occlusal view of tooth # 47 indicating: 1-Mesiobuccal cusp, 2-Mesiolingual cusp, 3-Distobuccal cusp, 4-Distolingual cusp and 5-Tuberculum sextum. (b) Occlusal view of full lower arch and (c) Occlusal view of tooth # 37, indicating: 1-Mesiobuccal cusp, 2-Mesiolingual cusp, 3-Distobuccal cusp, 4-Distolingual cusp, 5-Distal cusp, 6-Tuberculum intermedium and 7-Central cusp. (d) Buccal view of tooth #47 and (e) Buccal view of tooth #37.
Buccal view of Left side posterior occlusion. (arrow indicating malocclusion due to central cusp).

Under rubber dam isolation, the buccal caries on #37 was excavated and final restoration was done with light cured composite resin (Tetric N-ceram, Ivoclar Vivadent, Germany) [Table/Fig-1a-f]. The proximal caries in #34 was excavated and restored with composite resin. The central occlusal cusp tip on left and right second molars were gradually reduced about 0.2 mm per visit at an interval of 3-4 weeks for a span of three months, with a fine grit bur using high speed airotor handpiece with adequate coolant to minimise premature occlusal contacts. A 100μ articulating paper (Bausch Progess, Bausch Articulating papers, Inc., Nashua. USA) was used as a guide to achieve the desired enamel reduction. No reduction was done for the adjacent remaining cusps, since they did not interfere with occlusion. Most of the tooth reduction was done in Enamel and minimal dentin was exposed. A fluoride containing desensitising toothpaste was prescribed to manage any tooth sensitivity (Over topical fluoride application). At 6-months follow-up, the patient was reported asymptomatic.
Discussion
Supernumerary cusps or cusp-like structures are considered developmental anomaly, which occur due to the disturbance in the advanced bell stage. The common variations reported include carabelli cusp of molar, talon cusp in anterior teeth and DE of the premolar [2,3].
Kocsis GS et al., termed occlusal supernumery cusps as “Central cusps”. Accordingly, these are positioned between the buccal and lingual cusp tips on the occlusal surface of the posteriors, and on the lingual surface of anteriors [4]. These central cusp are defined by Kocsis GS et al., as a “supernumerary macrostructure of the tooth surface, representing a cusp formation on the occlusal surface of premolars and molars, and on the lingual surface of canines and incisor teeth [4]. Accessory cusp on occlusal surface of posterior teeth has been described in literature by various names; however, currently DE is the recommended term according to Oehlers F et al., and is preferred in literature extensively [5].
The prevalence of DE varies from less than 1% to approximately 8% [6]. DE is mostly found in people of Asian descent like Chinese, Thai, Malay, Japanese, Filipino, and Indian with estimates ranging from 0.5 to 4.3%, based on the population [4]. There are only few cases of bilateral occlusal central cusp reported in literature. Nagarajan S et al., reported bilateral central cusp in primary mandibular second molars [3], and Yan-gang R et al., reported bilateral DE in permanent maxillary molars [7]. The present paper reports a rare case of bilateral occurrence of occlusal central cusp in permanent mandibular second molars.
It is believed that the PAX9 (Paired box) and MSX1 (Muscle segment homeobox 1) genes are responsible for the abnormal shape of the teeth [8]. Leigh RW was the first person who described and reported a case of an enamel tubercle on the maxillary molar of an American Eskimo skull [9]. Histologically, accessory cusp or the DE may be composed of enamel, dentin and with or without pulpal projection into them. Based on histological appearance of pulp, Oehlers F et al., proposed the classification of evagination as: (i) With wide pulp horns (34%); (ii) Narrow pulp horns (22%); (iii) Constricted pulp horns (14%); (iv) Isolated pulp horn remnants (20%); and (v) No pulp horn (10%) [5].
Nagaveni NB and Umashankara KV reported a rare case of accessory cusp formation on a maxillary third molar in an Indian population [2]. A rare case report of DE in permanent mandibular molar was reported by Karuna YM et al., in Indian population [10].
Presence of additional cusps may pose dental problems like caries in the pits or developmental grooves between the accessory cusp and the tooth, sensitivity or pulp necrosis due to fracture or attrition of the protruded portion of the cusp [4,11]. Malocclusion with the opposing tooth is another possibility as the involved teeth erupt into the dental arches [11]. From anthropological aspect, the presence of these additional cusps is significant because their frequencies differ among various populations. Identification of such cusp is of clinical significance and their occurrence is common in some anomalies or syndromes [4].
Management of these cusps include, reduction of the tubercle followed by direct pulp capping and restoration, or reinforce the tubercle itself with resin [12]. However, a more conservative approach is to eliminate premature contacts if present, and place the patient under routine follow-up to monitor the attrition and pulp vitality [11]. Prophylactic sealing of deep grooves surrounding the cusp is also recommended in paediatric patients [2].
Conclusion(s)
Bilateral occlusal central cusps are non-metric dental trait. Early diagnosis of these occlusal central cusps in molars can avoid caries, pulpal complication and malocclusion. After prophylactic and preventive treatment, patients should be placed under periodic follow-up including monitoring of the pulp vitality.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? No
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: May 06, 2020
Manual Googling: Jul 03, 2020
iThenticate Software: Jul 28, 2020 (14%)
[1]. Danish G, Hedge U, Mull P, Nabeel S, Dental cusps: Normal, supernumerary and cusp-like structure- An overviewJ Orofac Res 2014 4(3):161-68.10.5005/jp-journals-10026-1150 [Google Scholar] [CrossRef]
[2]. Nagaveni NB, Umashankara KV, Maxillary molar with dens evaginatus and multiple cusps: Report of a rare case and literature reviewInt J Oral Health Sci 2013 3(2):92-97.10.4103/2231-6027.135979 [Google Scholar] [CrossRef]
[3]. Nagarajan S, Sockalingam MP, Mahyuddin A, Bilateral accessory central cusp of 2nd deciduous molar: An unusual occurrenceArch Orofac Sci 2009 4(1):22-24. [Google Scholar]
[4]. Kocsis GS, Marcsik A, Kokai EL, Kocsis KS, Supernumerary occlusal cusps on permanent human teethActa Biol Szeged 2002 46(1-2):71-82. [Google Scholar]
[5]. Oehlers F, Lee K, Lee E, Dens evaginatus (evaginated odontome): Its structure and responses to external stimuliDent Pract Dent Rec 1967 17:239-44. [Google Scholar]
[6]. Dankner E, Harari D, Rotstein I, Dens evaginatus of anterior teeth: Literature review and radiographic survey of 15,000 teethOral Surg Oral Med Oral Pathol Oral Radiol Endod 1996 81(4):472-75.10.1016/S1079-2104(96)80027-8 [Google Scholar] [CrossRef]
[7]. Yan-gang R, Li-yang G, Tao HU, Multiple dens evaginatus of premolars and molars in Chinese dentition: A case report and literature reviewInt J Oral Sci 2010 2(3):177-80.10.4248/IJOS1005221125795 [Google Scholar] [CrossRef] [PubMed]
[8]. Sedano HO, Ocampo-Acosta F, Naranjo-Corona RI, Torress-Arellano ME, Multiple dens invaginatus, mulberry molar and conical teeth. Case report and genetic considerationsMed Oral Patol Oral Cir Bucal 2009 14(2):E69-72. [Google Scholar]
[9]. Leigh RW, Dental pathology of the EskimoDent Cosmos 1925 67(9):884-98. [Google Scholar]
[10]. Karuna YM, Datta S, Rao A, Dens evaginatus on a permanent mandibular molar-report of a first caseIndian Journal Public Health Res Dev 2018 9(11):139-41.10.5958/0976-5506.2018.01440.7 [Google Scholar] [CrossRef]
[11]. Levitan ME, Himel VT, Dens evaginatus: Literature review, pathophysiology, and comprehensive treatment regimenJ Endod 2006 32:01-09.10.1016/j.joen.2005.10.00916410059 [Google Scholar] [CrossRef] [PubMed]
[12]. Morinaga K, Aida N, Asai T, Tezen C, Ide Y, Nakagawa KI, Dens evaginatus on occlusal surface of maxillary second molar: A case reportThe Bulletin of Tokyo Dental College 2010 51(3):165-68.10.2209/tdcpublication.51.16520877163 [Google Scholar] [CrossRef] [PubMed]