Ectopic Ureter in Single System Kidney in Association with Anorectal Malformation in Male Patient
MD Mokarram Ali1, Amit Kumar2, Rashi3, Amit Kumar Sinha4, Bindey Kumar5
1 Senior Resident, Department of Paediatric Surgery, AIIMS, Patna, Bihar, India.
2 Senior Resident, Department of Paediatric Surgery, AIIMS, Patna, Bihar, India.
3 Senior Resident, Department of Paediatric Surgery, AIIMS, Patna, Bihar, India.
4 Associate Professor, Department of Paediatric Surgery, AIIMS, Patna, Bihar, India.
5 Professor, Department of Paediatric Surgery, AIIMS, Patna, Bihar, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Md Mokarram Ali, Department of Paediatric Surgery, Second Floor, OPD Building, AIIMS, Patna-801507, Bihar, India.
E-mail: mohdmokarramali1990@gmail.com
Anorectal Malformations (ARM) are known to be associated with urogenital abnormalities. However, the incidence of ectopic ureter in these patients is rare. This report is about a two-year-old male child with ARM. The patient presented after a failed Posterior Sagittal Anorectoplasty (PSARP). The presenting complaint was urinary leak from rectum. Subsequently, the patient was taken up for redo-PSARP. During surgery, bilateral ectopic ureters were identified, incidentally. Surgeons operating on the patients of ARM should be vigilant about this rare association of ectopic ureter with ARM, so as to avoid its injury during perineal dissection.
Cystoscopy, Redo surgery, Urinary leak
Case Report
A two-year-old male child presented to the outpatient clinic with chief complaints of leakage of urine from anal opening for 1 year. Patient was born with absent anal opening for which he underwent sigmoid loop colostomy on day 2 of life and PSARP at the age of 10 months. Both procedures were performed in a private hospital. After PSARP, patient was asymptomatic for 2 months. He was voiding urine per urethra and was continent for urine. Later on, the patient developed the problem of urinary leak from rectum.
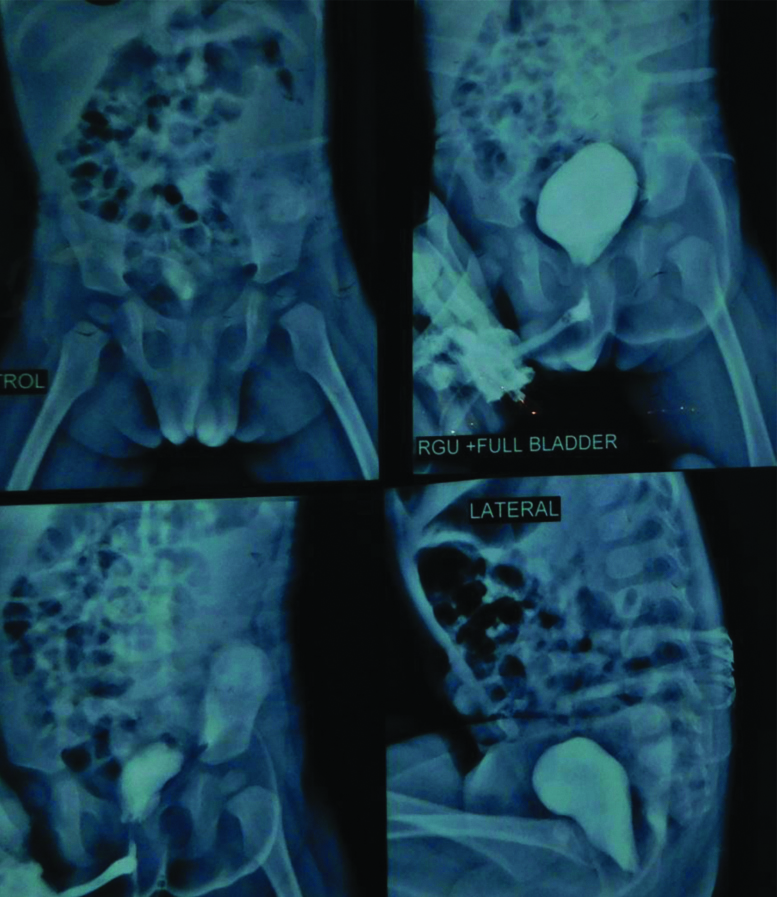
On perineal examination, the anal opening was found to be stenosed. Perianal area was soiled with urine. Other systemic examination was normal. Blood investigations were within normal limits. Ultrasonography of urinary tract was reported as normal. Retrograde urethrogram with Voiding Cystourethrogarphy (VCUG) was done in which no obvious communication of urethra with colon was seen [Table/Fig-1]. There was no evidence of vesicoureteric reflux. Patient was subsequently taken up for cystoscopy and redo PSARP.
Retrograde urethrogram with micturating cystourethrogram.
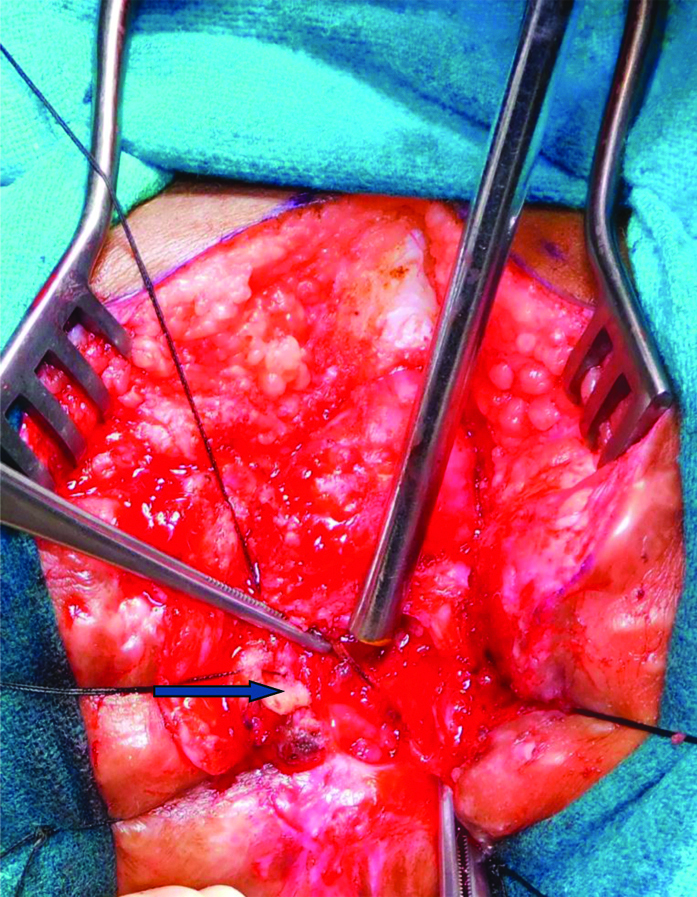
On cystoscopy, a fistulous opening was seen in posterior urethra distal to veru montanum. A guide wire passed through this fistulous opening which could be negotiated into the rectum. Thus, there was a remnant of original recto-urethral fistula through which there was leaking urine. On per rectal examination, anal opening was stenosed which could admit 6/7 Hegar’s dilator with difficulty. Patient was turned in prone position for PSARP. On perineal dissection, while dissecting rectum from lateral pelvic wall, a tubular structure was seen in right side which was inadvertently transected during dissection [Table/Fig-2]. This structure had a lumen and on introducing infant feeding tube in this structure, urine could be aspirated. On this basis, a diagnosis of right ectopic ureter was confirmed. This ectopic ureter was repaired over double J stent with absorbable suture. Rectum was further dissected away from posterior urethra. Recto urethral fistula was identified, divided and urethral end of the fistula repaired with absorbable sutures in two layers. Anorectoplasty was completed by placing the mobilised rectum in sphincter complex and suturing with skin.
Intraoperative picture showing transected ectopic ureter.
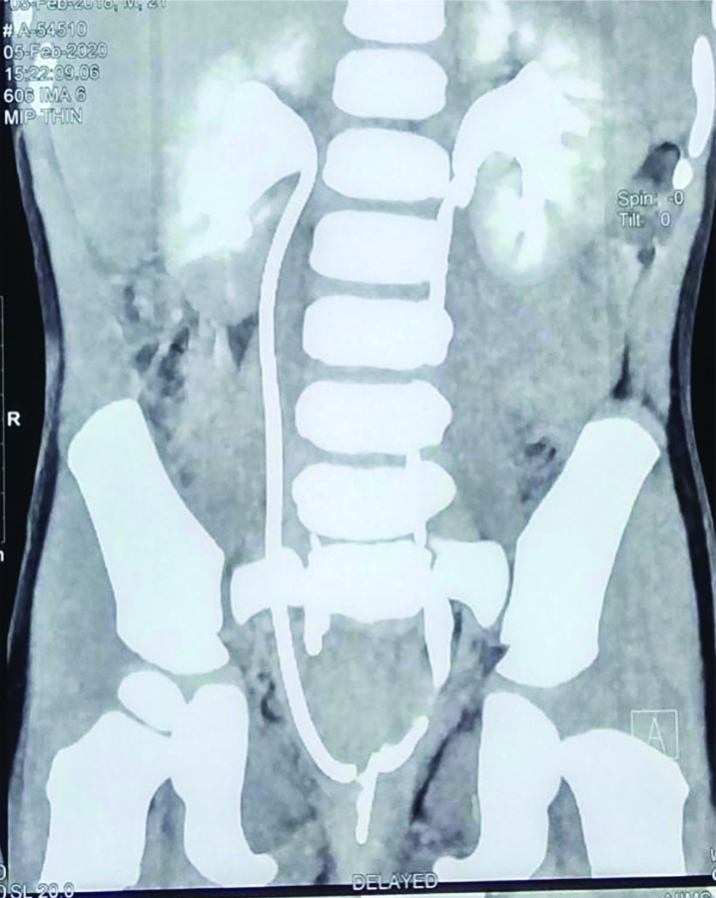
During the postoperative period, patient was further evaluated with Computed Tomographic (CT) urography which proved bilateral single system kidney with ectopic ureters on both sides opening into the bladder neck [Table/Fig-3]. This finding was confirmed by cystoscopy which was done after one month of surgery. On cystoscopy, double J stent on right side was seen entering into bladder near bladder neck.
CT urography demonstrating bilateral ectopic ureters.
Patient was subsequently discharged and is doing well at 6 months follow-up.
Discussion
An ectopic ureter draining a single system kidney is an uncommon congenital malformation. The ectopic ureteric orifice may open intravesically at level of bladder neck or extravesically into the urethra. ARM is known to be associated with other congenital anomalies in variable range. Congenital genitourinary malformations are seen in upto 50% of cases of ARMs with more severe malformations associated with high variant [1].
The incidence of bilateral ectopic ureters in non-duplicated system kidney is exceptionally rare [2]. Incidence of ectopic ureters is two to four times more in females as compared to males [3]. Majority of males with ectopic ureter have non duplicated kidneys [4]. Although, ARM is associated with congenital urogenital tract abnormalities in 50-60% cases, incidence of ectopic ureters in these patients is extremely rare [5]. The literature depicting the presence of ectopic ureter in ARM is limited. Hecht S et al., in their study concluded that overall incidence of ectopic ureter in patients with ARMs was 3.5% with 33% of ectopic orifices found in bladder neck [6]. In the present case too, the orifice of ectopic ureter was seen in bladder neck on cystoscopy.
Patients with more severe ARMs have a higher incidence of urogenital abnormalities, with ectopic ureters being commonly found in girls with long common channel cloaca and boys with recto bladder neck fistula [7]. In boys, opening of ectopic ureters may lie in the bladder neck, posterior urethra, or mesonephric duct derivatives (vas deferens, seminal vesicle, or epididymis) [8]. In girls, ectopic ureters may open into the bladder neck, upper urethra, vagina, vestibule, or less commonly the cervix or uterus [9]. Iatrogenic injury to the genitourinary tract has been explained in the anorectal surgical literature. Hong AR et al., in their study noted that surgical repair of ARM is associated with significant urologic injuries [10]. It is more so in patients who undergo surgery without an adequately performed distal cologram.
The surgical repair of ARMs entails dissection of the posterior urethra in males or separation of the bladder from the vagina in females, thus suspecting ectopic ureters and knowing their common locations may prevent iatrogenic ureteral damage. In the present case, patient was already operated at some other centre and presented with complication of urinary leak through anal opening. With a clinical doubt of remnant of original fistula, the patient was planned for redo PSARP. However, due to previous surgery, there was extensive fibrosis in perineal area. Plane of dissection could not be identified clearly. Thus, during the dissection, the presence of right side ectopic ureter was missed, which was accidentally transected. Subsequently, it was repaired over double J stent.
Conclusion(s)
Incidence of bilateral ectopic ureter in non-duplicated kidney in patients with ARM is extremely rare. However, they may be encountered during surgery, especially in cases of high ARMs. There should be high index of suspicion and surgeon should be vigilant while doing perineal dissection in such patients.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes (from parents)
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Apr 29, 2020
Manual Googling: Jun 11, 2020
iThenticate Software: Jul 28, 2020 (11%)
[1]. Peña A, Anorectal malformationsSemin Pediatr Surg 1995 4(1):35-47. [Google Scholar]
[2]. Zuniga ZV, Guzzo T, Docimo SG, Bilateral single system ectopic ureters in a male infantUrology 2005 66(2):43210.1016/j.urology.2004.07.02816051321 [Google Scholar] [CrossRef] [PubMed]
[3]. Malek RS, Kelalis PP, Stickler GB, Burke EC, Observations on ureteral ectopy in childrenJ Urol 1972 107(2):308-13.10.1016/S0022-5347(17)61012-7 [Google Scholar] [CrossRef]
[4]. Ahmed S, Barker A, Single-system ectopic ureters: A review of 12 casesJ Pediatr Surg 1992 27(4):491-96.10.1016/0022-3468(92)90345-8 [Google Scholar] [CrossRef]
[5]. McLorie GA, Sheldon CA, Fleisher M, Churchill BM, The genitourinary system in patients with imperforate anusJ Pediatr Surg 1987 22(12):1100-04.10.1016/S0022-3468(87)80717-0 [Google Scholar] [CrossRef]
[6]. Hecht S, Hall J, Ketzer J, Walker J, Trecartin A, Wilcox D, Ectopic ureters in anorectal malformationsPediatr Surg Int 2019 35(9):1005-08.10.1007/s00383-019-04517-x31278478 [Google Scholar] [CrossRef] [PubMed]
[7]. Rich MA, Brock WA, Peña A, Spectrum of genitourinary malformations in patients with imperforate anusPed Surgery Int 1988 :2-3.:110-13.10.1007/BF00182762 [Google Scholar] [CrossRef]
[8]. Johnston JH, Davenport TJ, The single ectopic ureterBr J Urol 1969 41(4):428-33.10.1111/j.1464-410X.1969.tb09944.x5808729 [Google Scholar] [CrossRef] [PubMed]
[9]. Greene LF, Ureteral ectopy in femalesClin Obstet Gynecol 1967 10(1):147-54.10.1097/00003081-196703000-000136021009 [Google Scholar] [CrossRef] [PubMed]
[10]. Hong AR, Acuña MF, Peña A, Chaves L, Rodriguez G, Urologic injuries associated with repair of anorectal malformations in male patientsJ Pediatr Surg 2002 37(3):339-44.10.1053/jpsu.2002.3081011877644 [Google Scholar] [CrossRef] [PubMed]