Variations in axillary artery branching pattern can lead to iatrogenic injuries during invasive procedures. Knowledge of the same is critical to prevent such events. Multiple bilateral variations were observed in the branching pattern of axillary artery. These variations were noted in a female cadaver, during routine undergraduate dissection in September 2019 in Lady Hardinge Medical College, New Delhi. On the left side, an anomalous branch running with the medial pectoral nerve was found. A common stem arising from the 2nd part of left axillary artery divided to give the lateral thoracic artery, the subscapular artery and an alar artery. Another alar branch arose from the left subscapular artery before it bifurcated into thoraco-dorsal and circumflex scapular arteries. The right axillary artery gave an aberrant branch proximal to the lateral thoracic artery. A common trunk arising from the 2nd part of right axillary branched out to give the posterior circumflex humeral artery, the subscapular artery and an alar artery. The brachial artery divided 13.5 cm proximal to the intercondylar line of humerus on the left and 14.4 cm on the right side. On both sides, the ulnar artery arose proximally and the radial and common inter-osseous arteries continued as a common trunk and divided distally. This case study reports multiple bilateral axillary artery anomalies and complements to the existing knowledge of vascular anomalies. Comprehensive knowledge of these variations is essential from anatomical, radiological and surgical point of view. During surgeries involving axillary and pectoral group of lymph nodes, such variations should be kept in mind.
Case Report
Arterial branching pattern in the upper limbs displays frequent variations. In this case report, multiple bilateral variations were observed in the branching pattern of axillary artery. These variations were observed in a female cadaver, during routine undergraduate dissection in September 2019 at Lady Hardinge Medical College, New Delhi. Cunningham’s Manual of Practical Anatomy was followed for the entire dissection procedure [1]. After the incisions for thoracic dissection were made, (incisions 1-4 in Cunningham’s), the axilla was dissected. Skin, fascia, loose connective tissue, fat, and lymph nodes were removed to expose the axillary artery and other contents of the axilla. The coraco-brachialis and short head of the biceps brachii muscles were exposed. The axillary artery was identified medial to these muscles. The pectoralis minor muscle was cut from its origin and retracted to expose the three parts of the axillary artery and their branches [1].
In this case, the 1st part of the axillary artery on both the sides followed the classical course and branching pattern. The second part of the axillary artery on the left side gave rise to an anomalous branch running with the medial pectoral nerve [Table/Fig-1].
shows 2nd and 3rd part of the left sided AA- Axillary artery. It further divides into TAA- Thoracoacromial artery, AnA1- Artery running with the medial pectoral nerve (MPN), CT- Common trunk which gives the LTA-Lateral thoracic artery and SSA-Subscapular artery (further dividing into TDA- Thoracodorsal artery and CSA- Circumflex scapular artery). The PCHA- Posterior circumflex humeral artery, ACHA- Anterior circumflex humeral artery arise from the 3rd part of the axillary artery. The BA- Brachial artery and its branch, PBA- Profunda brachii artery can been seen.

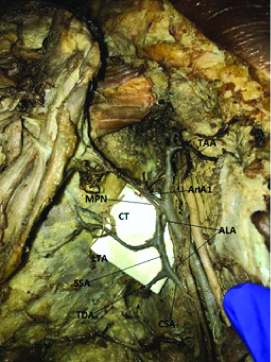
This branch pierced both the pectoralis major and minor muscles. Distal to the above branch, a common trunk from the second part of the axillary artery was noted which gave origin to the lateral thoracic artery and the subscapular artery [Table/Fig-2]. Two other branches (alar thoracic arteries) were found running towards the axilla. One of these branches arose from the common stem and the other branch divided from the subscapular artery proximal to its bifurcation into thoraco-dorsal and circumflex scapular artery [Table/Fig-2]. The brachial artery divided 13.5 cm proximal to the intercondylar line of humerus.
Shows ALA- Two Alar thoracic arteries arising both from the common trunk (CT) and the Subscapular Artery (SSA). Subscapular artery (SSA) further bifurcates into TDA-Thoracodorsal artery and CSA- Circumflex scapular artery. The thoracoacromial artery (TAA), lateral thoracic artery (LTA), anomalous artery (AnA1) running with the medial pectoral nerve (MPN) can be seen.
The left brachial artery divided 13.5 cm proximal to the intercondylar line of humerus [Table/Fig-3]. On the right side, an aberrant artery proximal to the lateral thoracic artery was found. It ran along the lateral border of pectoralis minor and then deep to it supplying the pectoralis minor and the serratus anterior [Table/Fig-4].
Shows left sided- BA- Brachial Artery giving off the, PBA- Profunda brachii artery and proximally dividing into UA- Ulnar artery and RA- Radial artery.

Show shows 2nd and 3rd part of the right axillary artery. Its 2nd part divides into TAA- Thoracoacromial artery, LTA- Lateral thoracic artery, AnA1- Artery proximal to LTA and a CT- Common Trunk which gives the PCHA- Posterior circumflex humeral artery, SSA- Subscapular artery and ALA- Alar artery. The 3rd part gave off ACHA- Anterior circumflex humeral artery. The terminal divisions of the subscapular artery (SSA), i.e., Thoracodorsal artery (TDA) and circumflex scapular artery (CSA) can be seen.

A common trunk for the posterior circumflex humeral artery and the subscapular artery was found [Table/Fig-4].
Proximally this common trunk gave an alar branch which bifurcated and was traced towards the axilla. The brachial artery bifurcated 14.4 cm proximal to the intercondylar line [Table/Fig-5].
Shows right sided- BA- Brachial Artery giving off the, PBA- Profunda brachii artery and high division of the ulnar artery (UA) and radial artery (RA).

This case study is significant because it reports multiple bilateral anomalous branches of axillary artery in a single cadaver.
Discussion
Axillary artery extends from the outer border of the 1st rib to the lower border of Teres major [2]. It is a direct continuation of the subclavian artery and continues as the brachial artery [2]. The Pectoralis minor passes over to divide the artery into 3 parts. Conventionally, six branches arise from the axillary artery [1]. Superior thoracic artery from the 1st part, thoracoacromial and lateral thoracic arteries from the 2nd part and subscapular, anterior circumflex humeral and posterior circumflex humeral arteries from the 3rd part [1]. Twenty three different types of axillary artery on the basis of origin of branches have been described [3]. Literature suggests 5-11 branches arising from the axillary artery [3]. A study by Huelke DF documents 2-7 direct branches of the axillary artery while Kanaka S et al., reported 5-8 branches originating from axillary artery [4,5]. Occasionally, the branches may take origin from a common stem or the sub-branches may arise directly from the main branch [6]. Axillary artery variations were noted to be found in 28% cases by Gaur S et al., and 33% by Ojha P et al., [7,8]. Variations are observed most commonly in the 3rd part of the axillary artery and rarely in the 1st part [7,8]. In the present case, no variations were observed in the 1st part of the axillary artery. However, bilateral variations were observed in 2nd and 3rd part of axillary artery. Nine branches on the left and eight branches on the right were noted.
In this case, an anomalous branch from the 2nd part of the left axillary artery accompanying the medial pectoral nerve was noted. This finding is rare. The artery along with the medial pectoral nerve pierced both the pectoralis major and minor muscles. In typical cases, the trunk of thoraco-acromial artery arises from the 2nd part of axillary artery to give rise to the acromial, deltoid, clavicular and pectoral branches [2]. Studies have shown absence of thoracoacromial trunk (10% cases) and its branches arising directing from the 2nd part of the axillary artery [9]. Pectoral branch can also arise directly from the 2nd part of axillary artery [9]. Jurjus AR et al., reported two pectoral branches from the thoraco-acromial artery, one running with the medial pectoral nerve [10].
Common trunk originating from the 2nd part of axillary artery has been reported in previous studies [4,5,11-14]. Srimathi T in her study reported a common trunk from the 2nd part of axillary artery [11]. The common trunk divided to give the thoraco-acromial artery, the lateral thoracic artery, the subscapular artery and the posterior circumflex humeral artery [11]. In a study by Patil DA et al., a subscapular-thoracoacromial trunk from the 2nd part of axillary artery divided into the subscapular and the thoracoacromial arteries [12]. The lateral thoracic artery (classically originating from the 2nd part of axillary artery) branched out from the subscapular artery along with the circumflex humeral and thoraco-dorsal arteries [12]. A study by Kanaka S et al., reported a common subscapular-thoracoacromial trunk from the 2nd part of axillary artery in 15% cases [5]. Muraleedhar B and Danigond MS reported a common trunk from the 2nd part of axillary artery running posteriorly and dividing into subscapular artery, anterior circumflex Humeral Artery, posterior circumflex Humeral Artery and profunda brachii artery [13]. In a similar case study, Ezzati M et al., reported a common stem from the 2nd part of axillary artery giving the lateral thoracic, subscapular and muscular branches [14].
According to literature, in 4% cases subscapular artery arises from the 2nd part and in 30% cases arises from a common trunk with posterior circumflex humeral artery [7]. Another study reported subscapular artery arising from the 1st part in 0.6% cases, 2nd part in 15.7% cases and 3rd part in 79.2% cases [4]. A subscapular- circumflex humeral trunk from the 3rd part of axillary artery was reported in 3.8% cases by Saeed M et al., [15]. This common trunk branched out to give the subscapular artery, anterior and posterior circumflex arteries [15]. Bhat KM et al., reported a case in which the anterior circumflex humeral artery divided from the 3rd part of axillary artery. A common trunk arising from the 2nd part of axillary artery gave-off the thoraco-acromial artery, the lateral thoracic artery, the subscapular and the posterior circumflex humeral [16].
Shantakumar SR and Rao KGM reported a common trunk from the 2nd part of axillary artery, for lateral thoracic artery and subscapular artery [17]. In the present case, on the left side, a common trunk for the lateral thoracic artery and the subscapular artery was found branching off from the 2nd part of axillary artery. The circumflex humeral arteries originated from the third part without any variations. A common trunk arose from the 2nd part of the right axillary artery. It branched out to give the posterior circumflex humeral artery, subscapular artery and a branch running towards the axilla (alar artery). The lateral thoracic and the anterior circumflex humeral arteries did not show any variation on the right side. According to a study conducted on 420 cadavers, lateral thoracic artery was found in 96.7 % of the specimens, demonstrating morphological variability [18]. According to its origin, six types of lateral thoracic artery were classified. In 67.62% specimens the lateral thoracic artery arose from the thoracoacromial artery (Type I), 17.02% from the axillary artery (Type II), 5% from the thoracodorsal artery (Type III), and 3.93% from the subscapular artery (Type IV). In 3.09% of the specimens multiple lateral thoracic arteries were present (Type V) and in 3.33% specimens lateral thoracic artery was completely absent (Type VI) [l8]. The lateral thoracic artery can become or give rise to a direct cutaneous branch called superficial thoracic artery [2].
In the current case, an anomalous branch proximal to the lateral thoracic artery took origin from the 2nd part of right axillary artery. It coursed along the lateral border and deep to the pectoralis minor. It supplied the pectoralis minor and gave muscular twigs to the serratus anterior.
Alar thoracic artery has been reported in the previous studies [19,20]. Extensive data regarding this uncommon variant is lacking. Gaur S et al., in their study of 50 cadavers, reported extra branches (alar arteries) arising from the 2nd part of axillary artery in 6% of the cases (3/50 cases) [7]. The available literature on the alar thoracic artery, describes it to be originating from the 2nd part or in few cases the 3rd part of the axillary artery [2,21,22]. It is known to supply the axillary lymph nodes, as well as the fat and skin of the axilla [2]. Mugurel reported a case with bilateral alar thoracic artery, on the right originating from the 3rd part of axillary artery and on the left directly from the high radial artery [19]. A thoraco- epigastric artery, with muscular trunk and superficial branches running towards the superficial epigastric artery has been documented [23]. This artery was described as a longer alar thoracic artery, supplemented with muscular branches [19]. In the current case, bilateral alar thoracic arteries were found. The lateral thoracic-subscapular common trunk from the 2nd part of the left axillary artery gave out an alar branch running towards the axilla while a second alar artery originated from the subscapular artery before it bifurcated into thoracodorsal and circumflex scapular arteries. On the right side a single alar artery branched out from the common trunk for the subscapular and posterior circumflex humeral artery (arising from the 2nd part of axillary artery). As mentioned above in most cases the alar artery branches out from the 2nd part of the axillary artery, which is in contrast to the findings in this case. Literature suggests the alar thoracic artery demonstrates peculiarities such as- bilateral presence, bilateral asymmetry, difference in origin on both the sides [19]. These peculiarities were noted in the present case as well.
In most cases, the brachial artery begins at the distal border of the tendon of teres major and ends at the level of the neck of the radius by bifurcating into the radial and ulnar arteries [2]. Brachial artery variations are widely documented. The artery may branch out proximally into two trunks and then rejoin [2]. Quite often the radial branch can arise proximal to the elbow joint, leaving a common trunk for the ulnar and common interosseous arteries [2]. The high origin radial artery is the most common arterial anomaly noted in the upper limb, with an incidence of 14.27% [24]. According to a study on 120 limbs, in typical cases the division of brachial artery into terminal branches was located in the cubital fossa below the intercondylar line of humerus. An 11/120 (9.2%) cases were reported to have high origin of radial artery [25]. In the current case, the ulnar artery arose proximally, and the radial and common interosseous arteries continued as a common trunk and divided distally. The brachial arteries of the left and right sides divided 13.5 cm and 14.4 cm above the intercondylar line of humerus, respectively. A comprehensive knowledge of the upper extremity arterial vascularisation is significant in surgical planning and reconstructive procedures [26].
Embryological Basis
Several hypotheses have been proposed regarding the embryonic basis of the vascular anomalies. As per literature, the lateral branch of the seventh cervical artery grows to form the axial artery of the upper limb and in course of time a network of capillaries develop [27]. Embryonic studies suggest that the capillaries which are destined to regress or remain as capillaries, fail to do so and they persist, enlarge and differentiate leading to arterial variations [27,28]. Variations in the upper limb vessel could also occur if the embryonic vascular network follows an abnormal pathway [27]. Defects in the surrounding tissue are another factor leading to vascular anomalies [27].
Clinical Correlation
Tumors, abscess, trauma, lymph nodes are often encountered in the axillary region [29]. Axillary lymph node dissection needs to be done in certain surgical, cases most important being breast carcinoma [29]. With the increased use of invasive diagnostic and therapeutic procedures in cardiovascular patients, the comprehensive knowledge of the vascular variations is indispensable [30,31]. Reconstructive surgery for cases such as aneurysm and trauma of axillary artery and its branches demand knowledge of these variations [26]. Axillary artery aneurysm is common in baseball pitchers [32]. Constant pressure exerted on the axillary artery in athletes, can cause focal hyperplasia of the tunica intima, aneurysm, segmental dissection predisposing to thrombosis and distal embolism [33]. In cases of chronic shoulder dislocation, the aberrant axillary artery branches are predisposed to bleeding. One should be aware of any abnormal axillary artery branches in chronic shoulder dislocation. Lack of knowledge of the variation can lead to bleeding during surgery [30,31]. Axillary artery is frequently lacerated and ruptured during reduction of old shoulder joint dislocation [34]. Hence the complete knowledge of the variations of axillary artery and the frequency is of utmost clinical significance.
Conclusion(s)
Axillary artery variations are frequently documented in literature. This case report showed multiple bilateral variations in the 2nd and 3rd part of the axillary artery. The report complements to the existing literature on the rare variations such as alar thoracic artery. Comprehensive knowledge of these variants is vital for the clinicians and surgeons to perform surgical procedures involving the axilla.
[1]. Koshi R, Cunningham’s manual of practical anatomy 2017 Volume 116th edOxfordELBS:29-31. [Google Scholar]
[2]. Standring S, Gray’s Anatomy: The Anatomical Basis of Clinical Practice 2016 41st editionPhiladelphiaElsevier limited:827-29. [Google Scholar]
[3]. Garis De, Swartley CF, The axillary artery in white and Negro stocksAm J Anat 1928 41(2):353-97.10.1002/aja.1000410208 [Google Scholar] [CrossRef]
[4]. Huelke DF, Variation in the origins of the branches of the axillary arteryAnat Rec 1959 135(1):33-41.10.1002/ar.1091350105 [Google Scholar] [CrossRef]
[5]. Kanaka S, Eluru RT, Basha MA, Somasekhar R, Kanchanalatha G, Haniman KS, Frequency of variations in axillary artery branches and its surgical importanceInt J Sci Stud 2015 3(6):01-04. [Google Scholar]
[6]. Hollinshead WH, Anatomy for surgeons in general surgery of the upper limb. The back and limbs 1958 Volume 3New YorkA Heber Harper Book:290-300. [Google Scholar]
[7]. Gaur S, Katariya SK, Vaishnani H, Wani IN, Bondre KV, Shah GV, A cadaveric study of branching pattern of axillary arteryInt J Biol Med Res 2012 3(1):1388-91. [Google Scholar]
[8]. Ojha P, Prakash S, Ghanshyam G, A study of variation in branching pattern of axillary arteryInt J Cur Res Rev 2015 7(11):72-75. [Google Scholar]
[9]. Pandey SK, Shukla VK, Anatomical variation in origin and course of thoracoacromial trunk and its branchesNepal Med Coll J 2004 6(2):88-91. [Google Scholar]
[10]. Jurjus AR, Correa-De-Aruaujo Bohn RC, Bilateral double axillary artery: Embryological basis and clinical implicationsClin Anat 1999 12(2):135-40.10.1002/(SICI)1098-2353(1999)12:2<135::AID-CA10>3.0.CO;2-M [Google Scholar] [CrossRef]
[11]. Srimathi T, Abnormal branching pattern of the axillary artery- A case reportInternational Journal of Basic Medical Sciences 2011 2(4):73-76. [Google Scholar]
[12]. Patil DA, Jadhav AS, Katti AS, Anatomical study of axillary artery variationsInt J Anat Res 2016 4(4):3117-21.10.16965/ijar.2016.415 [Google Scholar] [CrossRef]
[13]. Muraleedhar B, Danigond MS, Unilateral variation in branching pattern of third part of axillary artery. A case reportInt J Anat Res 2018 6(3.3):5602-04.10.21760/jaims.v3i3.12905 [Google Scholar] [CrossRef]
[14]. Ezzati M, Nasrabadi HT, Abedelahi A, Bahlakeh G, Kheirjou R, Ataei ML, Variations in the branches of axillary arteryInt J Anat Var 2018 11(3):75-76. [Google Scholar]
[15]. Saeed M, Rufai AA, Elsayed SE, Sadiq MS, Variations in the subclavian axillary arterial systemSaudi Med J 2002 23(2):206-12. [Google Scholar]
[16]. Bhat KM, Gowda S, Potu BK, Rao MS, A Unique branching pattern of the axillary artery in a South Indian male cadaverBratisl Lek Listy 2008 109(12):587-89. [Google Scholar]
[17]. Shantakumar SR, Rao KGM, Variant branching pattern of axillary artery: A case reportCase Rep Vasc Med 2012 2012:97696810.1155/2012/97696823094192 [Google Scholar] [CrossRef] [PubMed]
[18]. Loukas M, du Plessis M, Owens DG, Kinsella CR, Litchfield CR, Nacar A, The lateral thoracic artery revisitedSurg Radiol Anat 2014 36(6):543-49.10.1007/s00276-013-1234-x24281130 [Google Scholar] [CrossRef] [PubMed]
[19]. Rusu MC, Bilateral alar thoracic arteryFolia Morphol (Warsz) 2005 64(1):59-64. [Google Scholar]
[20]. Rustagi SM, Sharma M, Singh N, Mehta V, Suri RK, Rath G, Peripheral communications of intercostobrachial nerve Peripheral communications of the intercostobrachial nerve in relation to the alar thoracic arteryAdv Biomed Res 2015 4(1):5110.4103/2277-9175.15155525802820 [Google Scholar] [CrossRef] [PubMed]
[21]. Patnaik VVG, Kalsey G, Singla RK, Branching pattern of Axillary artery- A morphological studyJ Anat Soc India 2002 51(2):176-186. [Google Scholar]
[22]. Williams PL, Bannister LH, Berry MM, Collins P, Dyson M, Dussek JE, (1999) Gray’s anatomy. In: Gabella G (ed.)Arteries of the limbs and cardiovascular system38th EdLondonChurchill Livingstone:1537-39. [Google Scholar]
[23]. Kogan I, Lewinson D, Variation in the branching of the axillary artery- A description of a rare caseActa Anat 1998 162(4):238-40.10.1159/0000464399831773 [Google Scholar] [CrossRef] [PubMed]
[24]. Pelin C, Zagyapan R, Mas N, Karabay G, An unusual course of the radial arteryFolia Morphol (Warsz) 2006 65(4):410-13. [Google Scholar]
[25]. Astik R, Dave U, Variation in branching pattern of axillary artery: A study in 40 human cadaversJ Vasc Bras 2012 11(1):12-17.10.1590/S1677-54492012000100003 [Google Scholar] [CrossRef]
[26]. Sargon MF, Tanyeli E, Sürücü HS, Yazar F, Arifoğlu Y, A complicated variation of the upper extremity vascularisationKaibogaku Zasshi 1996 71(3):211-14. [Google Scholar]
[27]. Arey LB, Developmental anatomy 1936 3rd EdPhiladelphiaW.B. Saunders Co:312 [Google Scholar]
[28]. Hamilton WJ, Mossman HW, Cardiovascular systemIn: Human embryology 1972 4th EdBaltimoreWilliams and Wilkins:271-90. [Google Scholar]
[29]. Anson BJ, McVay CB, Thoracic walls: Breast or mammary regionIn: Surgical Anatomy. Anson, BJ, McVay, CB (Eds) 1984 6th editionPhiladelphiaSaunders:357 [Google Scholar]
[30]. Decker GAG, du plessis DJ, Lee Mc Gregor’s Synopsis of Surgical Anatomy 1986 12th edMumbaiK.M. Varghese company:451 [Google Scholar]
[31]. Cervicobrachial regionIn: Samuel L Turek’s orthopaedics: Principles and their Applications 1989 Vol 24th edNew DelhiJaypee brothers:913 [Google Scholar]
[32]. Schneider K, Kasparyan NG, Altchek DW, Fantini GA, Weiland AJ, An aneurysm involving the axillary artery and its branch vessels in a major league baseball pitcher: a case report and review of the literatureAm J Sports Med 1999 27(3):370-75.10.1177/0363546599027003180110352776 [Google Scholar] [CrossRef] [PubMed]
[33]. Duwayri YM, Emery VB, Driskill MR, Earley JA, Wright RW, Paletta GA Jr, Positional compression of the axillary artery causing upper extremity thrombosis and embolism in the elite overhead throwing athleteJ Vasc Surg 2011 53(5):1329-40.10.1016/j.jvs.2010.11.03121276687 [Google Scholar] [CrossRef] [PubMed]
[34]. Karambelkar RR, Shewale AD, Umarji BN, Variations in branching pattern of axillary artery and its clinical significanceAnatomica Karnataka 2011 5(2):47-51. [Google Scholar]