Role of Radiologist in Diagnosis of Neonatal Small Left Colon Syndrome: A Case Report
Ibrahim Haruna Gele1, Muhammad Baba Sule2, Sadisu Mohammed Maaji3, Abubakar Musa4, Muhammad Abacha5
1 Consultant Radiologist, Department of Radiology, Usmanu Danfodiyo University Teaching Hospital (UDUTH), Sokoto, Nigeria.
2 Lecturer and Consultant, Department of Radiology, Usmanu Danfodiyo University Teaching Hospital (UDUTH), Sokoto, Nigeria.
3 Department of Radiology, Usmanu Danfodiyo University Teaching Hospital (UDUTH), Sokoto, Nigeria.
4 Department of Radiology, Usmanu Danfodiyo University Teaching Hospital (UDUTH), Sokoto, Nigeria.
5 Lecturer, Department of Radiology, Usmanu Danfodiyo University Teaching Hospital (UDUTH), Sokoto, Nigeria.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Ibrahim Haruna Gele, Usmanu Danfodiyo University Teaching Hospital (UDUTH), PMB 2370 Sokoto, Nigeria.
E-mail: ihgele@yahoo.com
Neonatal small left colon syndrome is a well-defined functional disease of the lower colon and it results in signs and symptoms of intestinal obstruction. It is an uncommon cause of neonatal intestinal obstruction characterised by an abrupt transition of intestinal caliber at or near the splenic flexure. More than 50% of affected patients are born to mothers with diabetes. Authors hereby report a case of five-day-old neonate who presented with abdominal distension and vomiting diagnosed to have small left colon syndrome by contrast enema. Patient had surgical resection of the narrowed segment and anastomosis with subsequent resolution of symptoms.
Contrast enema, Gestational diabetes, Meconium, Neonate
Case Report
A five-day-old male neonate presented to emergency paediatric unit of a tertiary care center with 5 days history of progressive abdominal distension and vomiting. Patient was noticed to have gradual abdominal distension from day of birth, followed 3 days later with bilous vomiting. There was history of delayed passage of meconium, which was passed on the 3rd day after delivery. There was no history of fever. Neonate was the second child in a monogamous setting. There was no history of neonatal intestinal obstruction in the family. The antenatal period was uneventful except for gestational diabetes for which the mother was on oral hypoglycaemic drugs. Baby was born at term through unsupervised vaginal delivery at home.
On examination, the baby was alert but in mild respiratory distress. Patient was afebrile, not pale, and anicteric. Neonate weight was 3.1 kg. The abdomen was grossly distended but soft. There was normal anal opening. Digital rectal examination was unremarkable. No obvious congenital anomalies were seen. Initial investigation showed normal complete blood count but there was mild hyponatraemia. Clinical assessment of neonatal intestinal obstruction secondary to Hirschsprung disease was made and patient was referred to radiology department for barium enema.
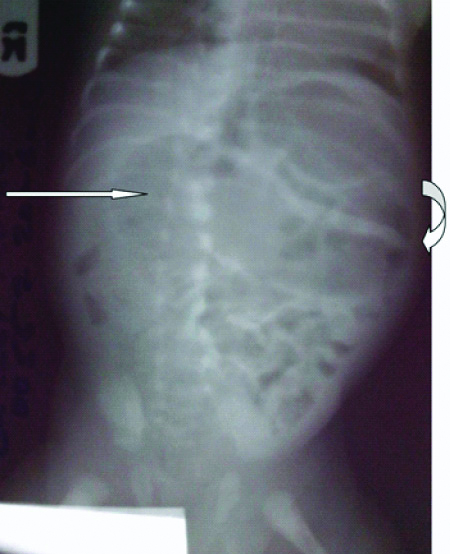
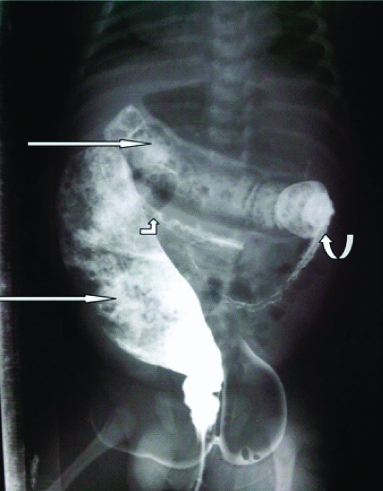
Plain abdominal radiograph in supine Antero-Posterior (AP) view showed bilateral flank fullness with gas distended large bowel loops in the upper abdomen. There was paucity of bowel gas shadows in the pelvis. No features of pneumoperitoneum were demonstrated [Table/Fig-1]. The contrast enema series was done with gastrografin after 1:1 dilution with normal saline. It showed a long segment of narrowing involving the descending colon from the splenic flexure to the proximal sigmoid colon with abrupt caliber transition at its ends. However, annular areas of constrictions were noted due to preserved haustration. There was gross distension of the demonstrated transverse colon due to partial obstruction at the narrowed distal colon. The recto/sigmoid index was reserved. Multiple mottled filling defects were demonstrated in the [Table/Fig-2]. With the above clinical and radiological features a diagnosis of neonatal small left colon syndrome was made with Hirchsprung’s disease as a differential. Patient symptoms failed to resolved following contrast enema and conservative management. Patient later had surgical resection of the narrowed colonic segment with subsequent anastomosis. Histopathology report of the resected segment showed normal ganglionic cells in the submcosa. Patient did well with no postoperative complication. Patient was discharged with no history of recurrence of symptoms on follow-up visits up to 3 months.
Plain abdominal radiograph supine showing flank fullness (curved arrow) and gas dilated large bowel loops in the upper abdomen (straight arrow).
Contrast enema antero-posterior view showing small caliber descending colon with abrupt transition at the splenic flexure (curved arrow) and sigmoid colon (bent-up arrow). There is gross distention of the transverse colon and rectum with contrast medium and meconium (straight arrows).
Discussion
Neonatal small left colon syndrome is defined as a functional disease of the lower colon which produces typical signs and symptoms of intestinal obstruction [1,2]. It is an uncommon cause of neonatal intestinal obstruction characterised by an abrupt transition of intestinal caliber at or near the splenic flexure [1,2]. It mainly affects the sigmoid and descending colon and is isolated to meconium inspissation or agangliosis [2,3]. It is believed to be due to a relative immaturity of bowel innervations and motility in full term infants [1] and the cause of intestinal obstruction in 1.5% of the cases [3,4]. More than half of the neonates with neonatal small left colon syndrome are born to diabetic mothers [3,5] as in the presented case here. Wood K et al., and Kang ZL et al., in United Kingdom and Singapore, respectively also reported similar cases in diabetic mothers in preterm neonates [6,7]. Numerous other influencing factors are eclampsia, fetal hypoglycemia and sepsis. Hypoglycaemia stimulates the sympathetic nervous system which causes decreased peristalsis in the left colon and the vagal stimulation results in increase in motility to the level of the splenic flexure. Hyperglucagonaemia which is the outcome from hypoglycaemia or sepsis also results in decreased peristalsis in the left colon which leads to increased absorption of water from the colon, which eventuates in the formation of abnormal meconium [5].
Neonates with small left colon syndrome typically present with history of non passage of meconium in the first 24 hours after birth, progressive abdominal distension and vomiting as seen in the presented case here. Unusual late complications include bowel perforation and peritonitis [5]. These were not observed in this case probably due to early presentation.
The diagnosis of this condition is by plain radiograph of the abdomen and contrast enema. Plain radiograph shows features of intestinal obstruction. Supine AP view shows dilated bowel loops while the supine lateral view showed distended loops of bowel with air fluid levels. Complicated cases with perforation show features of pneumoperitoneum such as Rigler’s sign (air outlining both walls of bowel) on supine AP radiograph and free air under the anterior abdominal wall on supine view. Contrast enema is diagnostic feature and may also be therapeutic. It shows a dilated ascending and transverse colon with abrupt change in caliber (transition) at the splenic flexure and a small caliber left colon as demonstrated in this case. In addition, gross dilatation of the rectum and distal part of the sigmoid colon was observed in this case which was absent in reported cases [6,7]. A large mucous plug which is seen as area of filling defect may be present in the splenic flexure and may be dislodged proximally during colonic filling in contrast enema. The recto-sigmoid index (normal neonatal rectum is of greater caliber than sigmoid colon) is preserved [1].
The differential diagnosis include Hirschsprung’s disease with a splenic flexure transition zone, meconium inspissations and colonic atresia [8,9]. In Hirschsprung’s disease the rectum is abnormally narrowed with reversal of the recto-sigmoid index. Almost all cases of meconium inspissations or ileus are associated with cystic fibrosis. Contrast enema in colonic atresia demonstrate a blind-ending colon with a convex distal border at the atretic site [1,8,9].
Small left colon syndrome is usually a self limiting condition with the contrast enema acting as a stimulus for subsequent passage of meconium and gradual improvement in clinical symptoms [4,6,7]. In case of intestinal perforation and if resolution of obstruction following contrast enema distribution does not occur then such cases are indicated for surgical operation [1,3]. This patient’s obstruction failed to resolve after the contrast enema and he subsequently had surgical resection and anastomosis.
After colonic resection surgical complications may arise post operative which includes surgical site infection, anastomotic leakage, intraabdominal abscess and bleeding [10]. These complications have influence on the outcome of the surgery. There were no such postoperative complications in the index case. Other complications that can occur following colonic resection include short bowel syndrome characterised by poor absorption of some nutrients and water [10].
Conclusion(s)
Neonatal left colon syndrome is a rare anomaly but with the use of basic radiographic techniques like plain abdominal radiograph and contrast enema; diagnosis of patients presenting with signs and symptoms of neonatal left colon syndrome becomes easy and it helps in its early diagnosis and treatment.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Nov 20, 2019
Manual Googling: Jan 14, 2020
iThenticate Software: Jun 25, 2020 (18%)
[1]. Karen ET, Catherine MO, The paediatric abdomen. In: Sutton DA textbook of Radiology and imaging 2003 17th edLondonChurchil-livingstone:861 [Google Scholar]
[2]. Skarsgard E, Small left colon syndrome 2013 <emedicine.medscape.com/ article/ 937183-overview.html> (accessed online on 2nd August, 2015) [Google Scholar]
[3]. Sharma S, Sharma BB, Chamaria K, Bansal K, Neonatal small left colon syndrome- Radiological diagnosis by Gastrografin contrast studyIndian J child Health 2015 2(1):29-30.10.32677/IJCH.2015.v02.i01.010 [Google Scholar] [CrossRef]
[4]. Ellis H, Kumar R, Kostyrka B, Neonatal small left colon syndrome in the offspring of diabetic mothers- an analysis of 105 childrenJ Paediatr Surg 2009 44(12):2343-46.10.1016/j.jpedsurg.2009.07.05420006023 [Google Scholar] [CrossRef] [PubMed]
[5]. Leung A KC, Wong AL, Kao CP, Small left colon syndrome in infants. Consultantlive 2002 <www.consultantlive.com/articles/small-left-colon-syndrome-infants> (accessed online on 2nd August 2015) [Google Scholar]
[6]. Wood K, Jinadatha A, Agrawal K, Narayanan S, Neonatal small left colon syndrome (NSLCS): Rare but important complication in an infant of diabetic motherBMJ Case Rep 2018 2018:bcr-2017-22345610.1136/bcr-2017-223456 [Google Scholar] [CrossRef]
[7]. Kang ZL, Ravanna KG, Abdulhaium AA, Sriram B, Neonatal small left colon syndromeBMJ Case Rep 2015 2015:bcr-2015-2422810.1136/bcr-2015-21122826443091 [Google Scholar] [CrossRef] [PubMed]
[8]. Hajivassiliou CA, Intestinal obstruction in neonatal/paediatric surgerySemin Paediatr Surg 2003 12(4):241-53.10.1053/j.sempedsurg.2003.08.00514655163 [Google Scholar] [CrossRef] [PubMed]
[9]. Juang D, Snyder CL, Neonatal bowel obstructionSurg Clin North Am 2012 92(3):685-711.10.1016/j.suc.2012.03.00822595716 [Google Scholar] [CrossRef] [PubMed]
[10]. Kirchhoff P, Clavien P, Hahnloser D, Complications in colonic surgery, risk factors and preventive strategiesPatient Saf Surg 2010 4(5):1-13.10.1186/1754-9493-4-520338045 [Google Scholar] [CrossRef] [PubMed]