Dental appearance, Fixed prosthodontics, Occlusion, Vertical dimensions
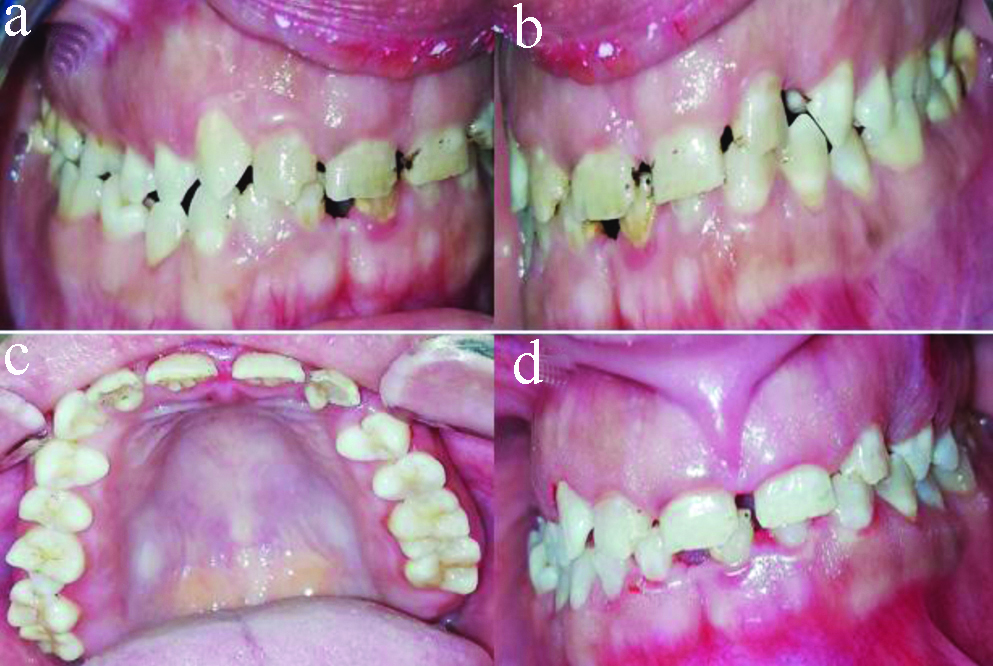
A 23-year-old female patient presented to the Outpatient Clinic of Conservative Dentistry Department, Alexandria University, Egypt. The patient complained of poor facial and dental appearance and mobility of lower incisors. Patient history did not reveal any current medical conditions or a family history, any previous injury or trauma and no previous interventions were made to treat the patient. With extraoral examination, no TMJ dysfunction, muscle pain, or tenderness was found. Analysis of facial appearance was performed using photos, no horizontal or vertical asymmetry was noted, and the patient presented a class I skeletal pattern. Intraoral examination detected abnormal shape and size of teeth with spaced anterior teeth and low labial frenum attachment that greatly impaired aesthetics while the enamel had normal opacity and texture which led to excluding amelogenesis and dentinogenesis imperfecta [Table/Fig-1]. Smile analysis revealed a wide smile zone and a gummy smile. Probing depth was ≥5 mm for anterior teeth and ≥2 mm for posterior teeth with thick gingival biotype.
(a-d) Preoperative view of the patient teeth.
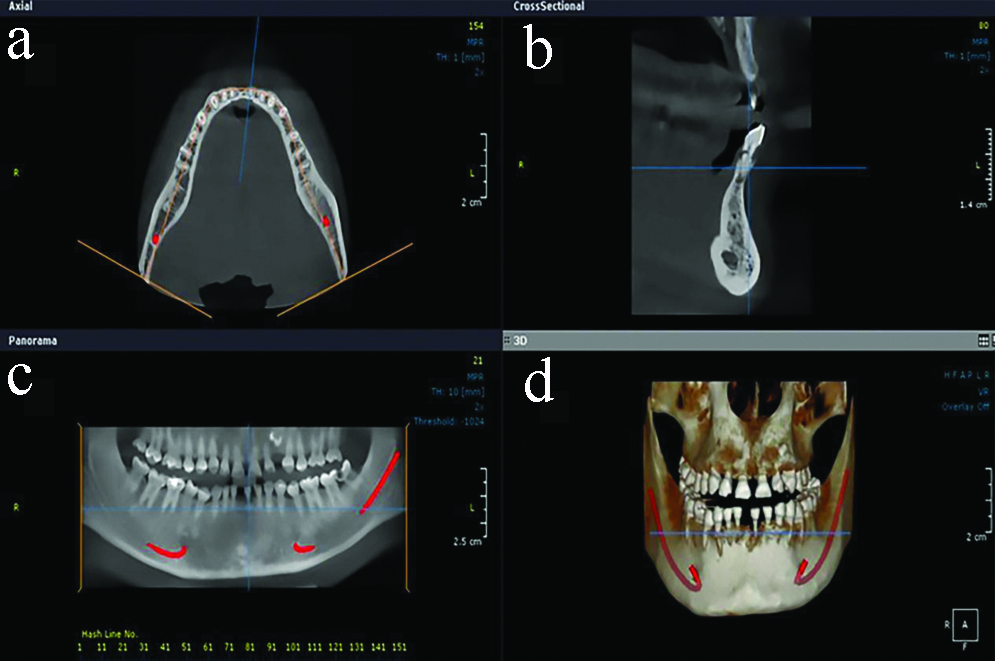
Panoramic radiograph and cone beam tomography cross-sectional view confirmed a severe horizontal bone loss, PDL widening of mandibular incisors and oblique fracture of lower left central incisor. The radiographs also detected an impacted upper left canine [Table/Fig-2].
Preoperative cone beam tomography image showing impacted canine for the patient: (a) axial view; (b) cross-sectional view; (c) panoramic view; (d) 3D view.
The patient had severe trauma from occlusion causing wear and mobility of lower incisors. Occlusal analysis revealed that no disocclusion of incisors during lateral excursive movements and absence of proper anterior guidance (canine or group function protection) leading to an abnormal overload of lower incisors, mobility, periodontal damage and fracture of teeth [1].
An assessment of vertical dimension was performed. Facial sagittal view of the patient displayed mandibular pseudo-prognathism which might be a sign of vertical dimension loss. In addition, the vertical dimension was measured at rest and in occlusion as the distance between two fixed points at the tip of the nose and the chin using a metal gauge. The subtraction of the two values revealed a loss of the vertical dimension with increased inter-occlusal space up to 4 mm [2].
The treatment plan decided was to extract the lower incisors, and restoring them with monolithic zirconia fixed partial denture with canines and premolars as abutments. In addition, to extract the impacted canine and restoring it with monolithic zirconia fixed partial denture with upper left central, lateral and first premolar as abutments, and restoring the rest of teeth with monolithic zirconia single crowns. The treatment plan was explained to the patient along with the possible alternative procedures as implant replacement of incisors and orthodontic extrusion of impacted canine instead of extraction. The patient preferred the first plan considering the time frame of the treatment and the choice to avoid surgery. Informed consent was obtained for the treatment plan as well as for the possible publication of the case.
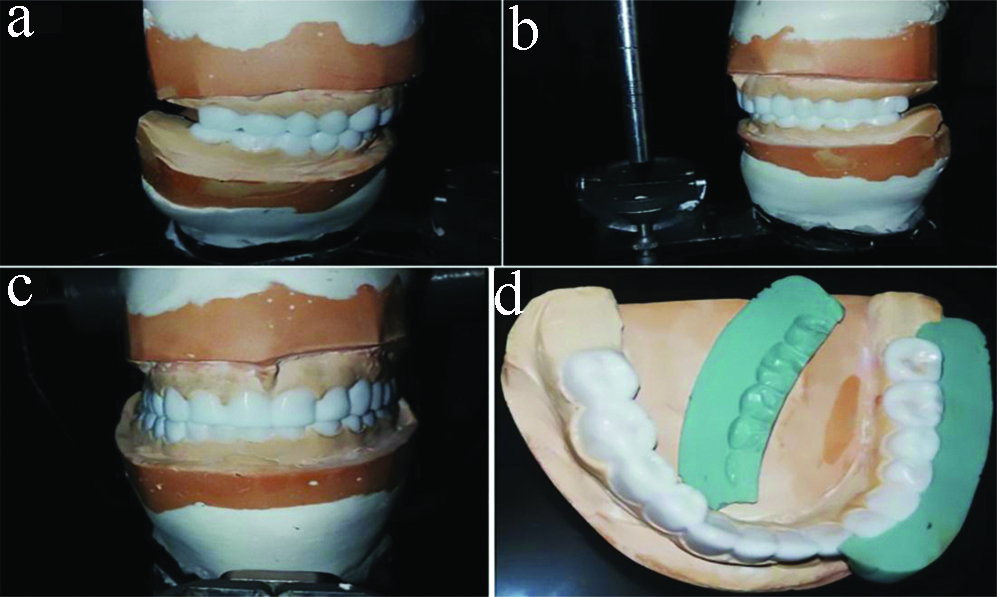
The high labial frenum attachment was repositioned surgically to provide a space for a planned surgical crown lengthening and to improve the aesthetics. Face bow record (Hanau Wide-Vue, Whip Mix, USA), centric relation record and eccentric records were used to mount diagnostic casts to the semi-adjustable articulator (Hanau Wide-Vue, Whip Mix, USA). The incisal pin was raised 3 mm and the diagnostic wax-up was made, the lower occlusal plan was adjusted in the wax using the Broadrick flag method and a putty index [Table/Fig-3] [3].
(a-d) Diagnostic wax-up. Occlusal plane analysis was done using the Broadrick flag method and a putty index.
The wax-up was duplicated onto stone casts (Elite Stone, Zhermack, Italy) and vacuform matrices were fabricated from thermoplastic sheets (Patterson Tray Material, Patterson Dental, USA). Surgical crown lengthening was performed using the vacuform matrices as a guide. A functional mock-up was fabricated using the vacuform matrices and light cure composite (Te-Econom Plus, Ivoclar Vivadent, Germany), enamel was roughened with a diamond point followed by acid etching and bonding, the vacuform matrices were filled with composite, seated on the teeth and light-cured for 40 seconds from each tooth aspect, then finished and polished, occlusion was checked in centric and eccentric using articulating paper. The purpose of the mock-up was to motivate the patient, raise the vertical dimensions and keep the bite raised when preparing the teeth as each quadrant was prepared and temporised in a separate visit to avoid patient exhaustion [Table/Fig-4].
(a-d) Upper and lower vacuform sheets used as a guide for aesthetic crown lengthening and as external surface form for composite functional mock-up immediately done following the aesthetic crown lengthening.

After the teeth of both arches were prepared and temporised, the patient could wear the temporary restorations for 3 months, and the patient was instructed to perform all functional activities like chewing, speech, avoid biting hard objects and perform oral hygiene measures. The patient was informed to expect discomfort and pain during the first weeks due to raised vertical dimension. After 3 months the final impressions were taken to fabricate the final restorations for molars of both sides. Impressions for both arches were taken using monophase polyether impressions (3M Monophase, 3M Deutschland GmbH, Neuss, Germany). Facebow and centric records were obtained while the bite and VD were stabilised by the provisional restorations on premolars and anterior teeth. The working casts were poured, mounted using facebow record and centric record and scanned using a laboratory scanner (Ceramill map 400, Amann Girrbach AG, Austria). CAD/CAM Monolithic zirconia crowns were fabricated (Ceramill zolid fx multilayer, Amann Girrbach AG, Austria), the crowns were tried-in for seating and proximal and centric occlusal contacts before glaze. A custom incisal table was fabricated from alginate impressions (Chromaclone, Ultradent Products, USA) over the provisional restorations of both arches to replicate the anterior guidance of the temporary restorations. This custom incisal table was used to readjust the occlusal morphology and cusp angle of the fabricated CAD/CAM crowns for the molars before final glaze and cementation [Table/Fig-5]. After cementation of final crowns for molars, final impressions were taken to fabricate anterior crowns and fixed partial dentures using monolithic zirconia using the same workflow applied for fabrication of the posterior crowns. All final restorations were bonded using zirconia primer (Z-Prime Plus, Bisco, Inc., USA) and resin cement (TheraCem, Bisco, Inc., USA) [Table/Fig-6].
Custom incisal table for adjusting the crowns for molars.

(a-d) The monolithic zirconia restoration after insertion.

The patient accommodated to the new vertical dimensions and displayed no complains during a 1-year follow-up period, in addition, clinical and radiographic examinations revealed excellent results [Table/Fig-7a,b].
(a-b) Incisal guidance established in the zirconia restorations and group function occlusion.

Monolithic zirconia is a novel ceramic material introduced to overcome the problem of veneer chipping in porcelain fused to zirconia restorations in addition to excellent aesthetics and strength [4].
The alternative treatment option was to extract the lower incisors with ridge augmentation and implants, and to extrude the impacted canine orthodontically followed by fixed zirconia restoration for both arches to re-establish vertical dimension, aesthetics, and occlusion. This alternative was refused by the patient as it would take a longer period of treatment. While the executed plan was less traumatic, consumed less time and the patient was satisfied with the results. However, long term studies about the clinical success of monolithic zirconia mainly fixed partial dentures are rare in the literature which necessitates a long follow-up for this case [5].
Group function occlusion in lateral excursions was created in this case because the patient had a short canine which will also serve as an abutment for the lower fixed partial denture [6].
Monolithic multilayered zirconia was selected in this case to achieve adequate strength and aesthetics mainly for the long span of lower anterior fixed partial denture [4]. Few clinical reports described the use of monolithic zirconia for long span and full-arch cases, two studies by Amin S et al. and Fisselier F et al. reported a case of full-mouth rehabilitation with monolithic zirconia prosthesis, the treatment showed similar results to the current case report [7,8].
Long-term follow-up for the case was planned for abutments and long-span fixed partial denture re-evaluation. Monolithic zirconia can be used successfully for such cases requiring aesthetic and functional rehabilitation.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Apr 27, 2020
Manual Googling: May 15, 2020
iThenticate Software: Jun 26, 2020 (6%)
[1]. Sapkota B, Gupta A, Pattern of occlusal contacts in lateral excursions (canine protection or group function)Kathmandu Univ Med J 2014 12(45):43-47.10.3126/kumj.v12i1.1363725219993 [Google Scholar] [CrossRef] [PubMed]
[2]. Abduo J, Lyons K, Clinical considerations for increasing occlusal vertical dimension: A reviewAust Dent J 2012 57(1):02-10.10.1111/j.1834-7819.2011.01640.x22369551 [Google Scholar] [CrossRef] [PubMed]
[3]. Lynch CD, McConnell RJ, Prosthodontic management of the curve of Spee: Use of the Broadrick flagJ Prosthet Dent 2002 87(6):593-97.10.1067/mpr.2002.12517812131879 [Google Scholar] [CrossRef] [PubMed]
[4]. Han JS, Yeo IS, Application of monolithic zirconia ceramics in dental practice: A case history reportInt J Prosthodont 2016 29(4):511-13.10.11607/ijp.477227611758 [Google Scholar] [CrossRef] [PubMed]
[5]. Schriwer C, Skjold A, Gjerdet NR, Øilo M, Monolithic zirconia dental crowns. Internal fit, margin quality, fracture mode and load at fractureDent Mater 2017 33(9):1012-20.10.1016/j.dental.2017.06.00928662859 [Google Scholar] [CrossRef] [PubMed]
[6]. Thornton LJ, Anterior guidance: group function/canine guidance. A literature reviewJ Prosthet Dent 1990 64(4):479-82.10.1016/0022-3913(90)90048-H [Google Scholar] [CrossRef]
[7]. Amin S, Weber HP, Kudara Y, Papaspyridakos P, Full-mouth implant rehabilitation with Monolithic Zirconia: Benefits and LimitationsCompend Contin Educ Dent 2017 38(1):e01-04. [Google Scholar]
[8]. Fisselier F, Comut AA, Contemporary management and full mouth rehabilitation of a patient with Sjögren syndromeJ Prosthet Dent 2018 120(1):05-08.10.1016/j.prosdent.2017.10.01529258693 [Google Scholar] [CrossRef] [PubMed]