Variations of Biceps Brachii Muscle and its Clinical Importance
Jolly Agarwal1, Krishna Gopal2
1 Assistant Professor, Department of Anatomy, Government Doon Medical College, Dehradun, Uttarakhand, India.
2 Professor, Shri Ram Murti Smarak Institute of Medical Sciences, Bareilly, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Jolly Agarwal, Assistant Professor, Department of Anatomy, Government Doon Medical College, Dehrakhas, Dehradun-248001, Uttarakhand, India.
E-mail: drjolly21177@gmail.com
Introduction
Biceps brachii is one of the functionally important muscles of front of the arm. As the name indicates biceps brachii is having two heads of origin and it inserts on the posterior surface of radial tuberosity. Variations may be present in the form of additional heads of origin or they may be present at its insertion. These variations may affect action of muscle and may cause compression of nearby neurovascular structures.
Aim
To determine the variation in anatomy of biceps brachii with respect to its origin, insertion and its nerve supply.
Materials and Methods
The present osteological study was conducted on 32 arms of embalmed cadavers (including both right and left) of Department of Anatomy, SRMS IMS, Bareilly, Uttar Pradesh, India from 2015-2018 period. The dissection of arm was done according to standard guidelines and biceps brachii muscle was cleaned. The origin, insertion and nerve supply of biceps brachii muscle was observed and noted for any variation.
Results
In the present study an additional head of origin of biceps on right and left side of two cadavers were found. In present study inferomedial origin of biceps brachii was found. The present study also showed the presence of musculotendinous slip at its insertion. This slip was going towards the muscle belly of pronator teres.
Conclusion
There are numerous variations seen in biceps brachii which can put a surgeon in dilemma and it may result in iatrogenic injuries. Hence, it is important to have a knowledge about its variations so that such injuries can be prevented.
Arm, Head, Muscles, Nerve
Introduction
Biceps brachii is one of the muscles of the front of arm [1]. As the name indicates biceps brachii is having two heads of origin–long head of biceps arises from supraglenoid tubercle and capsule of shoulder joint and short head arises from tip of coracoid process of the scapula. It inserts on the posterior surface of radial tuberosity, after giving bicipital aponeurosis. This muscle is supplied by the musculocutaneous nerve. It performs screwing movement and supination at radioulnar joints. It partially flexes the elbow joint [1]. Variations are not usual findings in biceps brachii muscle.
If variations are present then they may affect action of muscle. The action of muscle may become weak or strong [2]. Presence of extra heads may be injured by surgeons during surgeries which may cause injury to neurovascular structure of upper limb [3]. Additional heads may cause bone displacement after fracture. Sometime musculotendinous slips from muscle may insert at more than one place, then it may result in independent function of each part of the muscle [4]. These variations are important and surgeons should keep in mind during surgeries.
Embryologically, the development of the biceps brachii muscle may affect the course and the branching pattern of musculocutaneous nerve [5,6]. The bulky third head causes compression of the musculocutaneous nerve which leads to variable clinical symptoms. So, importance of these variations lies during surgical operations of the arm and in searching the nerve injuries [7].
Therefore, the clinical importance of biceps muscle motivates us to carry out this study with an aim to determine variation of biceps brachii with respect to its origin, insertion and its nerve supply.
Materials and Methods
The present observational osteological study was conducted on 32 arms of embalmed cadavers irrespective of age and sex (including both right and left) of Department of Anatomy, SRMS IMS, Bareilly, Uttar Pradesh, India from June 2015- April 2018 period after taking Ethical clearance from Institutional ethics Committee (Ref. No. SRMSIMS 2016-17/99B). The dissection of arm was done according to standard guidelines [8].
Inclusion criteria: Cadavers with no anomaly or traumatic and fractured limb were included.
Exclusion criteria: Cadavers with congenital anomaly, traumatic limbs and fractures were excluded from study. A longitudinal incision was given from the front of the arm to the acromion process of scapula to a point 2.5 cm below the level of elbow joint [8]. Then, at both ends of the longitudinal incision a horizontal incision was given. Fat present below the skin was removed and both superficial and deep fascia was removed [8]. Biceps brachii muscle was cleaned and carefully observed. The origin, insertion and nerve supply of biceps brachii muscle was observed and noted for any variation. Photographs were taken for the purpose of record and reference.
Results
The most common variation of biceps brachii muscle was the presence of third head of biceps brachii but its incidence was 6.25% in present study. Two additional heads were present; One was on right side [Table/Fig-1] and one on left side i.e., in two cadavers [Table/Fig-2]. These additional heads of biceps brachii were supplied by the musculocutaneous nerve. In present study 93% cadavers biceps was having two head of origin.
Depicts presence of additional head (arrow) taking origin from anterior surface of humerus, long head (single star) and short head (double star) on the right side.
Depicts presence of additional head (arrow) taking origin from anteromedial surface of humerus, long head (single star) and short head (double star) on left side.

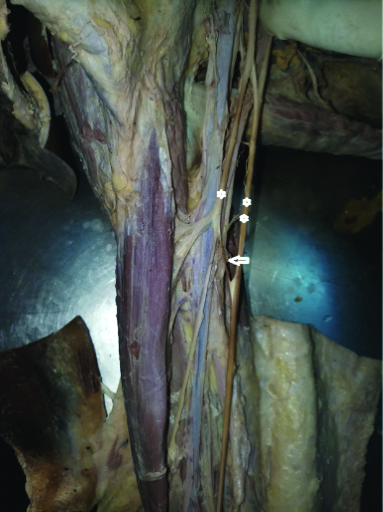
Present study also reveals the presence of communicating branch which communicates the musculocutaneous nerve with the median nerve [Table/Fig-3].
Depicts presence of communicating branch (white arrow) from musculocutaneous nerve (single star) to median nerve (double star).
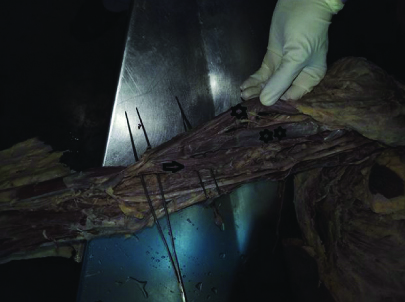
The present study also showed the presence of musculotendinous slip at its insertion. This slip is going towards the muscle belly of pronator teres. This musculotendinous slip was present superficial to brachial artery and the median nerve. The tendon of short head ends in musculotendinous slip which was going towards muscle belly of flexor carpi radialis and tendon of short head do not insert on radial tuberosity. Short head did not fuse with the long head and was fused with the slip. The biceps muscle and musculotendinous slip is supplied by musculocutaneous nerve [Table/Fig-4].
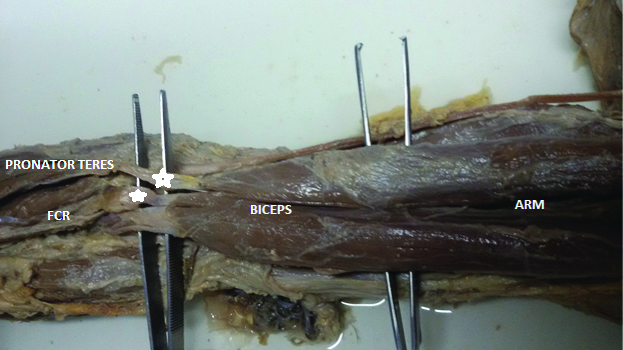
Depicts musculotendinous slips (star) from biceps brachii at its insertion to pronator muscle belly and Flexor Carpi Radialis (FCR) muscle belly.
Discussion
In present study, the most common variation of biceps brachii muscle is presence of third head of biceps brachii but its incidence was 6.25% in present study. Percentage of incidence of extra third head of origin of biceps brachii is described in [Table/Fig-5] [2,6,9-13]. One rare type of finding in the insertion of biceps was also observed. The insertion of biceps tendon was dividing into three distinct parts. The tendon of long head of biceps was inserted on radial tuberosity and this tendon the musculotendinous slip to muscle belly of pronator teres. This musculotendinous slip was present superficial to brachial artery and median nerve. While the tendon of short head ends in musculotendinous slip which was going towards muscle belly of flexor carpi radialis and it did not insert on radial tuberosity. Biceps brachii muscle is supplied by the musculocutaneous nerve. Such type of variation was not reported earlier. Such type of variation should be kept in mind to avoid pitfalls while performing reconstructive surgeries of tendon and repair in cases of avulsion.
Comparison of percentage of incidence of extra third head of origin of biceps brachii [2,6,9-13].
| Authors | Incidence of extra heads of origin of biceps brachii muscle |
|---|
| Avadhani R and Chakravarthi KK [9] | 16.66% |
| Ambali Manoj P et al., [10] | 11.53% |
| Cheema P and Singla R [11] | 2.3% |
| Kervancioglu P and Orhan M [12] | 8.33% |
| Kumar H et al., [6] | 3.3% |
| Lokanadham S and Subhadra Devi V [2] | 5% |
| Bharambe VK et al., [13] | 13.3% |
| Present study | 6.25% |
Paval J and Mathew JG reported a case in which main tendon was inserted on the radial tuberosity, while few of its fibres from the medial side, below the middle of arm created muscle belly. Its tendon is divided into medial and lateral slip. Medial slip was inserted on the medial supracondylar ridge of humerus and the lateral slip merged with the fascial covering of flexor carpii ulnaris and found superficial to brachial artery and median nerve [14].
Embryologically, the upper limb develops from somites that migrate to form the limb bud. By differential growth and apoptosis, under higher molecular regulation somites lead to muscle formation. Due to unevenness in the expression of Hoxgenes and process the variations of the muscle arise usually, therefore resulting in absence, presence or abnormal orientation of the muscle or its part [15].
Avadhani R and Chakravarthi KK observed three headed biceps brachii, and in these heads the third head was of humeral origin, which was also inserted into the radial tuberosity by forming common tendon with the long and short heads [9]. They found incidence of third head of biceps brachii and similar type of variation i.e., three headed biceps brachii was reported in present study. The incidence of additional head of origin of biceps brachii is to be as much as 10% as reported by Gray’s Anatomy [1]. These findings are similar to the findings of present study.
According to their position the supernumerary heads of biceps brachii muscle are classified into superior, infero-medial and infero-lateral heads [16]. Testut L reported Acromial, labial and pectoral heads of supernumerary heads of biceps brachii [17]. In present study, inferomedial origin of biceps brachii was observed. The supernumerary bicipital head originated from the anteromedial surface of the humerus just below the insertion of coracobrachialis as observed by Abu-Hijleh MF [18]. These findings also endorsed present study findings. Gupta C and D’souza S found that the three headed biceps brachii was present unilaterally in three male cadavers, one belonging to the left side and two to right side [8]. While in present study, equal incidence of presence of additional head on the right and left side was observed. Sweiter MG and Carmichael SW reported that the incidence of the third head of the biceps was more on the right side as compared to left side [19], while equal incidence of presence of additional head of biceps brachii on the right and left side was fond in present study.
Musculocutaneous nerve passing between supernumerary heads, or supernumerary heads pierced by musculocutaneous nerve has been reported. This intramuscular course of musculocutaneous nerve is usually reported to be associated with its interconnection with median nerve [20]. In present study, additional heads of biceps brachii which are supplied by musculocutaneous nerve was found. The presence of communicating branch connecting musculocutaneous and the median nerve was also observed.
Hsu JC et al., reported a small case series of injuries of this nerve with varied mechanism ranging from strenuous exercise to weight lifting, throwing of football etc., [21]. Biceps brachii will be useful as a component of flap surgery. In such cases the knowledge of the innervation of accessory head as well as the compression of vasculature will be very much required by surgeons [22].
Limitation(s)
The present study may include larger number of cadavers but it depends upon availability of cadaver. More studies are needed to observe communicating branch between median and musculocutaneous nerve.
Conclusion(s)
The additional heads of biceps brachii may be significant in producing the strong flexion as well as supination of forearm. They may cause compression of brachial artery and median nerve. Variation of biceps brachii may confuse a surgeon who operates on the arm and which may lead to iatrogenic injuries. Presence of communicating branch between musculocutaneous and median nerve may be at risk of intermuscular compression which may result in various neural symptoms like tingling, weakness of movements, etc. The musculotendinous slip which was superficial to median nerve and brachial artery may compress these structures. The additional head may be injured in shoulder joint surgeries. Care should be taken for the same.
Author Declaration:
Financial or Other Competing Interests: None
Was Ethics Committee Approval obtained for this study? Yes
Was informed consent obtained from the subjects involved in the study? No
For any images presented appropriate consent has been obtained from the subjects. No
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: May 25, 2020
Manual Googling: Jun 03, 2020
iThenticate Software: Jun 06, 2020 (16%)
[1]. Standring S, The Anatomical Basis of Clinical Practice 2008 40th editionSpainElsevier Churchill Livingstone:825 [Google Scholar]
[2]. Lokanadham S, Subhadra Devi V, Unusual presentation of supernumerary head of biceps brachii muscle in South Indian populationWorld J Med Sci 2011 6(3):115-20. [Google Scholar]
[3]. Aggarwal A, Kaur H, Sahni D, Aggarwal A, Four-headed biceps brachii muscle with variant course of musculocutaneous nerve: Anatomical and clinical insightInt J Anat Var 2009 2:127-30. [Google Scholar]
[4]. Eames MH, Bain GI, Fogg QA, Van Riet RP, Distal biceps tendon anatomy: A cadaveric studyJBJS 2007 89(5):1044-49.10.2106/JBJS.D.0299217473142 [Google Scholar] [CrossRef] [PubMed]
[5]. Warner JJ, Paletta GA, Warren RF, Accessory head of the biceps brachii. Case report demonstrating clinical relevanceClinical Orthopaedics and Related Research 1992 (280):179-81.10.1097/00003086-199207000-00022 [Google Scholar] [CrossRef]
[6]. Kumar H, Das S, Rath G, An anatomical insight into the third head of biceps brachii muscleBratislavské Lekárske Listy 2008 109(2):76 [Google Scholar]
[7]. Roberts WH, Anomalous course of the median nerve medial to the trochlea and anterior to the medial epicondyle of the humerusAnnals of Anatomy-Anatomischer Anzeiger 1992 174(4):309-11.10.1016/S0940-9602(11)80290-6 [Google Scholar] [CrossRef]
[8]. Gupta C, D’souza S, A morphological study of third head of biceps brachii in human cadavers with its clinical implicationsSaudi Journal for Health Sciences 2014 3(3):12910.4103/2278-0521.142316 [Google Scholar] [CrossRef]
[9]. Avadhani R, Chakravarthi KK, A study on morphology of the biceps brachii muscleNitte University Journal of Health Science 2012 2(3) [Google Scholar]
[10]. Ambali Manoj P, Jadhav Surekha D, Patil Raosaheb J, Doshi Megha A, Roy Priya P, Extra heads of biceps brachii: A cadaveric studyNational Journal of Basic Medical Sciences 2012 2(3):274-78. [Google Scholar]
[11]. Cheema P, Singla R, Low incidence of the third head of the biceps brachii in the North Indian populationJournal of Clinical and Diagnostic Research 2011 5(7):1323-26. [Google Scholar]
[12]. Kervancioglu P, Orhan M, An anatomical study on the three-headed biceps brachii in human foetuses, and clinical relevanceFolia Morphologica 2011 70(2):116-20. [Google Scholar]
[13]. Bharambe VK, Kanaskar NS, Arole V, A study of biceps brachii muscle: Anatomical considerations and clinical implicationsSahel Medical Journal 2015 18(1):3110.4103/1118-8561.152156 [Google Scholar] [CrossRef]
[14]. Paval J, Mathew JG, A rare variation of the biceps brachi muscleIndian Journal of Plastic Surgery 2006 39(01):65-67.10.4103/0970-0358.26907 [Google Scholar] [CrossRef]
[15]. Mooney EK Loh C. Hand Embryology Gross Morphologic Overview of Upper Limb Development. Source – http://emedicine.medscape.com/article/1287982-overview [Google Scholar]
[16]. Rodríguez-Niedenführ M, Vázquez T, Choi D, Parkin I, Sañudo JR, Supernumerary humeral heads of the biceps brachii muscle revisitedClinical Anatomy: The Official Journal of the American Association of Clinical Anatomists and the British Association of Clinical Anatomists 2003 16(3):197-203.10.1002/ca.1006012673814 [Google Scholar] [CrossRef] [PubMed]
[17]. Testut L, Signification anatomique du chef humeral du muscle bicepsBulletins Memories de la sciete d’ Anthroplogic De Paris 1883 6:238-45. [Google Scholar]
[18]. Abu-Hijleh MF, Three-headed biceps brachii muscle associated with duplicated musculocutaneous nerveClinical Anatomy: The Official Journal of the American Association of Clinical Anatomists and the British Association of Clinical Anatomists 2005 18(5):376-79.10.1002/ca.2010015971222 [Google Scholar] [CrossRef] [PubMed]
[19]. Swieter MG, Carmichael SW, Bilateral three headed biceps brachii muscleAnatomisher Anzeiger 1980 148(4):346-49. [Google Scholar]
[20]. Vazquez T, Rodríguez-Niedenführ M, Parkin I, Sañudo JR, A rare case of a four-headed biceps brachii muscle with a double piercing by the musculocutaneous nerveSurgical and Radiologic Anatomy 2003 25(5-6):462-64.10.1007/s00276-003-0146-613680180 [Google Scholar] [CrossRef] [PubMed]
[21]. Hsu JC, Paletta Jr GA, Gambardella RA, Jobe FW, Musculocutaneous nerve injury in major league baseball pitchers: A report of 2 casesThe American Journal of Sports Medicine 2007 35(6):1003-06.10.1177/036354650629753817293466 [Google Scholar] [CrossRef] [PubMed]
[22]. Mas N, Pelin C, Zagyapan R, Bahar H, Unusual relation of the median nerve with the accessory head of the biceps brachii muscle: An original case reportInt J Morphol 2006 24(4):561-64.10.4067/S0717-95022006000500007 [Google Scholar] [CrossRef]