Thyroid carcinoma is one of the most frequent endocrine tumours at present. Different factors: both cellular and molecular plays a role in its development and progression. Loss or decreased expression of cell adhesion molecules such as E-cadherin and CD56 have been identified in thyroid tumourigenesis, invasion and metastasis [1,2].
The prognosis of thyroid carcinoma is influenced by the histological type, gender, extent of tumour and occurrence of distant metastasis [3]. Papillary carcinoma is the most common thyroid neoplasm, representing about 80% of all thyroid malignancies [1]. The incidence of this tumour is rapidly increasing around the world. In India, the southern state Kerala has reported highest incidence of PTC. It is characterised by a distinctive set of nuclear features [4]. But frequently diagnosis and differentiating from benign lesions/adenoma may be difficult; as there are a good number of histological variants and borderline condition. At times, some of them are completely encapsulated [5].
In these situations, evaluation of the expression of adhesion molecules like E-cadherin and CD56 are useful in confirming the diagnosis. E-cadherin is a transmembrane glycoprotein with a role in cell polarity, cell-cell adhesion and tissue architecture formation [6]. Loss of its expression correlates with malignant potential and lymph node metastasis [7]. CD56 is a neural cell adhesion molecule which regulates cell motility and migration capacity of tumour cells [2]. CD56 is expressed at higher levels in normal thyroid tissue and benign follicular lesions of the thyroid like Follicular adenomas and Hyperplastic nodules while it is absent in PTC [8].
E-cadherin and CD56 are two cell adhesion molecules with important role in the pathogenesis of PTC, so in this study the immunohistochemical expression of both were evaluated. The objectives of this study were to evaluate the expression of E-cadherin and CD56 in PTC, its adjacent normal thyroid tissue, as well as in non-neoplastic thyroid lesions. The effect of reduced E-cadherin expression in prognosis was also evaluated.
Materials and Methods
This was a descriptive study conducted over a period of 18 months from January 2018 to June 2019 at Amala Institute of Medical Sciences, Thrissur. The sample size was calculated by the following formula:
z1-α=0.05=1.96; Power=90%=1.28; P1= proportion of E-cadherin/CD 56 among non-neoplastic thyroid; P2=proportion of E-cadherin/CD 56 among PTC; n=30; 15 in each group; Minimum sample size=30.
A total of 76 (38 PTC cases and 38 Non-neoplastic lesions) Thyroidectomy specimens were studied after getting approval from the Institutional Research and Ethical Committee (IEC No- AIMSIEC/59/2017).
Inclusion criteria: All cases of histologically diagnosed PTC and equal number of non-neoplastic thyroid tissue specimens received in the Department of Pathology, Amala Institute of Medical Sciences, Thrissur were included in the study.
Exclusion criteria: Those cases in which there was no adequate normal thyroid tissue along with carcinoma, Cases where prior treatment had been given for PTC, Cases where radiation and chemotherapy for other primary malignancy had been administered and NIFTP (Non-Invasive Follicular Thyroid neoplasms with Papillary like nuclear features) were excluded from the study. The details of the patients were collected from Histopathology requisition forms and case sheets. Formalin-fixed paraffin embedded tissue sections were used (thickness 4-5 μm). All 76 samples were subjected to immunohistochemical staining with E-cadherin (NCH-38 mouse clone, Dako) and CD56 (123C3 clone, Dako) mouse monoclonal antibodies. IHC staining was done manually using standardised technique.
Procedure for Immunohistochemical Staining
Antigen retrieval was done in Ethylenediaminetetraacetic Acid (EDTA) buffer. Following which washed in Phosphate Buffered Saline (PBS) buffer
Endogenous peroxidase activity was blocked by treatment with peroxidase block for 10 minutes and again washed in PBS buffer.
Non-specific protein binding in tissues was prevented by incubating with power block for 10 minutes at room temperature.
Next, the tissue was incubated with primary antibody along with their positive and negative controls and after 1 hour washed with PBS buffer.
Then, secondary antibody (Polymer Horse Radish Peroxidase (HRP) for 30 mins) was added and washed in PBS buffer. The section was covered with chromogen to produce crisp brown colour at the site of target antigen.
Washed in PBS buffer followed by wash in Distilled water; then dipped in Haematoxylin stain.
Washed with water & dehydrated using graded alcohol.
Finally, clearing was done in xylene and mounted using Dibutylphthalate Polystyrene Xylene (DPX)
Evaluation
Semi-quantitative scoring was done as positive and negative under light microscopy based on the cytoplasmic and membranous staining for CD56. Under this semi-quantitative scoring, focal reactivity of up to 10% (cytoplasmic and membranous) was considered negative [6].
Scoring system for E-cadherin was as 0(<5%, none), 1(5%-25%, mild), 2(25-50%, moderate) or 3 (>50%, severe) based on the rate and intensity of cytoplasmic membranous staining. The scores 0, 1 and 2 were considered negative and 3 was positive [6]. Invasive ductal carcinoma breast tissue was used as a positive control for E-cadherin and normal thyroid tissue was used as a positive control for CD56. Similar scoring method was employed to assess the staining pattern in adjacent normal thyroid tissue of PTC and non-neoplastic lesions.
Statistical Analysis
For statistical analysis, the data was entered into Excel worksheets and coded accordingly. The data was done using IBM SPSS Version 23.0 statistical software. Qualitative data were presented using the frequency and related percentage. Comparison of qualitative variables between groups was done using the Chi-square test and Fisher’s exact test. Sensitivity, specificity, positive and Negative Predictive Values (NPV) was calculated for the examined markers. A p-value of <0.05 was considered as significant.
Results
In this study, age of the patients with PTC ranged from 19-70 years with mean age of 45.71 years. In patients with non-neoplastic lesions, age ranged from 21 to 65 with mean age of 45.13 years.
PTC: Of the 38 PTC cases, 30 (78.9 %) were females and 8 (21.1%) were males, whereas in the other group, i.e., Non-neoplastic lesions, 36 (94.7%) were females and 2 (5.3 %) were males. Majority of PTC cases (42.1%, n=16) involved the right lobe. Left lobe was involved in 28.9% (n=11) cases. 23.7% (n =9) cases showed involvement of both lobes. Isthmus was involved in 5.3% (n=2) cases. In this study, 39.5% (n=15) were conventional PTC [Table/Fig-1], 13 (34.2%) were Papillary Microcarcinoma (PMC) and 6 (15.8%) were Follicular variant of PTC. Special variants of PTC such as oncocytic, clear cell, tall cell and hobnail accounted for 1 each.
Conventional papillary thyroid carcinoma (H&E stain, X40).

Seventeen cases had multiple foci of lesion, 7 showed capsule invasion and 3 cases had extrathyroidal spread. Majority of cases (81.6%, n=31) belonged to Stage I. Less than one-fourth of the cases (15.8%, n=6) were in Stage II. Only a single case was in Stage III (2.6%). Lymph node metastasis was noted in 9 out of 19 cases for which lymph node dissection was done.
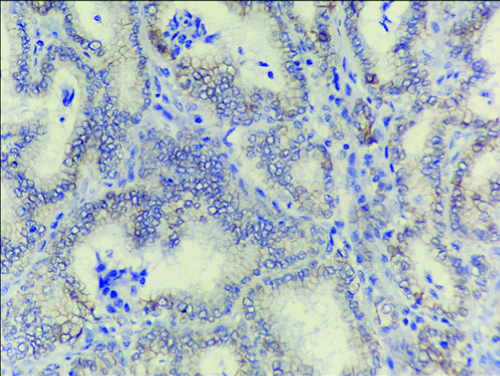
E-cadherin expression: Score of 0 (<5%) was present in 8 cases of PTC. Fourteen cases showed a score of 1 (5-25%). Fifteen cases had a score of 2 (25-50%). Thus, 37 cases showed negative expression for E-cadherin [Table/Fig-2]. The case with preserved expression was conventional PTC [Table/Fig-3]. CD56 expression was uniformly negative in all the PTC cases [Table/Fig-4]. Tall cell variant was negative for both, E-cadherin and CD56 [Table/Fig-5a-c].
Papillary microcarcinoma with negative E-cadherin expression (Score2) in tumour (X400).
Conventional Papillary thyroid carcinoma showing positive E-cadherin expression in tumour and adjacent tissue (IHC, X100).

Conventional PTC negative for CD56 expression in tumour area (IHC, X400) and positive for adjacent thyroid tissue (inset, IHC, X40).
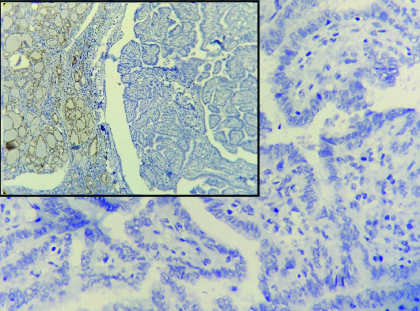
a) Tall cell variant PTC (H&E stain X100); b) Tall cell variant with negative E-cadherin expression (IHC, X400); c) Tall cell variant with negative CD 56 expression (IHC, X400).
Among 38 the PTC cases, there were 7 cases with capsular invasion and all of them showed loss of IHC staining with E-cadherin. Similarly, of the 9 cases with lymph node metastasis 8 cases (88.89%) showed loss of E-cadherin IHC staining. All the 17 cases (100%) with multiple foci and 3 of 3 cases (100%) with extrathyroidal spread showed loss of staining for E-cadherin IHC marker. There were 25 cases with tumour size >1 cm and out of which 24 (96%) cases showed loss of E-cadherin expression.
Status of Adjacent Thyroid Tissue
Of the 38 cases, 14 (36.8%) had colloid goiter. Thyroiditis accounted for 15 (39.5%) cases; of which 9 (23.7%) were lymphocytic thyroiditis and 6 (15.8%) were Hashimoto thyroiditis. Rest of the 9(23.7%) cases had normal thyroid parenchyma. In the adjacent thyroid tissue, E-cadherin expression was positive with a score of 3 in 33 (86.8%) cases. Rest of the cases, 13.2% (n=5) showed an E-cadherin expression of Score 2.
In majority of cases (n=21, 55.2%), CD56 expression was positive. The remaining cases (n=17, 44.8%) were negative for CD56. These observations were statistically significant with a p-value of 0.015 [Table/Fig-6].
Relation between CD56 expression and adjacent normal thyroid tissue.
| Adjacent thyroid tissue of PTC | CD56 (Adjacent) | Total |
|---|
| Negative | Positive |
|---|
| Normal | 8 | 1 | 9 |
| Colloid goitre | 3 | 11 | 14 |
| Lymphocytic thyroiditis | 4 | 5 | 9 |
| Hashimoto thyroiditis | 2 | 4 | 6 |
| Total | 17 | 21 | 38 |
Fisher’s-exact test p-value=0.015; PTC- Papillary thyroid carcinomas
Non-neoplastic Thyroid Lesions
Of the 38 non-neoplastic thyroid cases, majority 22 (57.9%) were Nodular Colloid Goiter (NCG) and 5 (13.1%) cases were Hyperplastic nodule. Hashimoto and Lymphocytic thyroiditis accounted for 8 (21.1%) and 2 (5.3%) cases, respectively. A single case of NCG with papillary hyperplasia (2.6%) was present. E-cadherin was positive for 36 cases, of which 22 were NCG [Table/Fig-7]. There were 8 cases of Hashimoto thyroiditis, 4 cases of Hyperplastic nodule and 2 of Lymphocytic thyroiditis with Score 3 expression. 1 case each of NCG with Papillary hyperplasia and Hyperplastic nodule showed a score of 2. This observation was statistically significant with a p-value of 0.021 [Table/Fig-8].
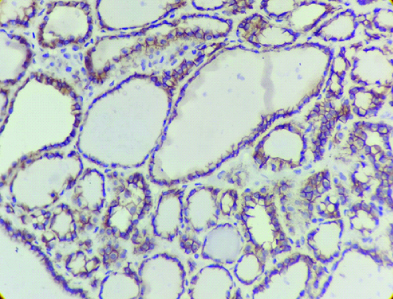
Nodular colloid goiter with positive E-cadherin expression (IHC, X400).
Study of E-Cadherin expression in non-neoplastic thyroid lesions.
| Microscopic diagnosis | E-cadherin | Total |
|---|
| Score 2 | Score 3 |
|---|
| NCG | 0 | 22 | 22 |
| Hashimoto thyroiditis | 0 | 8 | 8 |
| NCG with papillary hyperplasia | 1 | 0 | 1 |
| Hyperplastic nodule | 1 | 4 | 5 |
| Lymphocytic thyroiditis | 0 | 2 | 2 |
| Total | 2 | 36 | 38 |
Fisher’s-exact test p-value=0.021; NCG: Nodular colloid goiter
CD56 expression: A total of 34 (89.4%) cases were CD56 positive, of which 22 were NCG [Table/Fig-9], 7 were Hashimoto thyroiditis, 3 were Hyperplastic nodule and 2 were Lymphocytic thyroiditis. Four (10.6%) cases with negative expression were distributed among cases with NCG with papillary hyperplasia (1), Hyperplastic nodule (2) and Hashimoto thyroiditis (1). This observation was statistically significant with a p-value of 0.011 [Table/Fig-10].
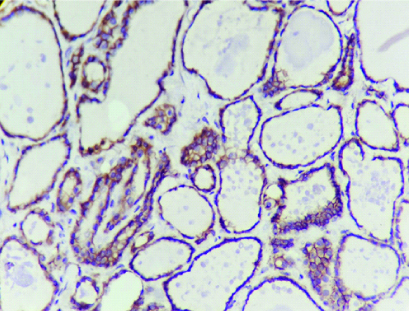
Nodular colloid goiter with positive CD56 expression (IHC, X400).
Study of CD 56 expression in non-neoplastic thyroid lesions.
| Microscopic diagnosis | CD56 | Total |
|---|
| Negative | Positive |
|---|
| Nodular colloid goitre | 0 | 22 | 22 |
| Hashimoto thyroiditis | 1 | 7 | 8 |
| NCG with papillary hyperplasia | 1 | 0 | 1 |
| Hyperplastic nodule | 2 | 3 | 5 |
| Lymphocytic thyroiditis | 0 | 2 | 2 |
| Total | 4 | 34 | 38 |
Fisher’s-exact test p-value=0.011
In summary, 37 PTC cases were negative for E-cadherin. Only two non-neoplastic lesions were negative for E-cadherin. The difference was statistically significant with a p-value of 0.0001. All the cases of PTC showed negative CD56 expression. A total of 34 out of 38 Non-neoplastic cases showed positive CD56 staining. The observation was statistically significant (p=0.011). CD56 showed higher specificity (100%) than E-cadherin in this study, but the latter was more sensitive (94.7%). The Positive Predictive Value (PPV) for CD56 was 100% and for E-cadherin was 97.2%.
E-cadherin loss and CD56 negativity were statistically significant with a p-value of 0.0001 [Table/Fig-11].
Sensitivity, Specificity, Positive Predictive Value (PPV) and Negative Predictive Value (NPV) of E-cadherin and CD56 (Chi-square test).
| Parameters | E-cadherin loss | CD56 negativity |
|---|
| Sensitivity (%) | 94.7 | 89.4 |
| Specificity (%) | 97.3 | 100 |
| PPV (%) | 97.2 | 100 |
| NPV (%) | 94.8 | 90 |
| Accuracy (%) | 96 | 94.7 |
| p-value | 0.0001 | 0.0001 |
Discussion
Even though PTC is the most common thyroid malignancies worldwide as well as in India but difficulty in accurate diagnosis can occur [2]. Ancillary tests like Immunohistochemistry can be helpful in such instances.
In the current study, 37 PTC cases showed negative E-cadherin expression (97.3%). However, within this group low and heterogeneous expression of E-cadherin was observed. Only one PTC case showed positive staining pattern. In the adjacent thyroid tissue, E-cadherin expression was positive in 86.8% cases (n=33). This is similar to the study by Ozolins A et al. They demonstrated that there was a significant reduction in E-cadherin expression in PTC compared to the adjacent thyroid tissue [6]. The low and heterogeneous expression of E-cadherin in PTC in the present study is comparable with the results of Soares P et al., and Mitselou A et al., [3,9].
In the present study, 36 out of 38 cases of non-neoplastic thyroid lesions showed positive E-cadherin expression (94.7%). Eidelman S et al., first reported that E-cadherin was expressed in normal thyroid tissues [10]. Similarly in a Japanese study by Naito A et al., E-Cadherin was preserved in all 60 samples of normal thyroid specimens [7].
There are data in literature supporting the association of reduced E-cadherin expression with poor prognosis in thyroid carcinomas. Scheumman GF et al., had identified the clinical significance of E-cadherin as a prognostic marker in thyroid carcinomas [1]. Similar conclusions were obtained by Erdem H et al., where they found the presence of E-cadherin in tumour epithelium, correlated with the absence of metastasis and local invasion [2]. However, in the present study, the lack of statistically significant association could be due to the reduced sample size.
In our study, all PTC cases showed negative CD56 expression. However, in the adjacent thyroid tissue, 55.3% showed positive CD56 expression. This is similar to the series published by Demellawy D et al., who reported 100% negativity in PTC [11]. Ozolins A et al., concluded that PTC showed an extremely low expression of CD56 compared with the surrounding tissue [6]. Similar results were obtained by Ceyran AB et al., [8]. In the present study, the special variants included Hobnail, Tall cell, Clear cell and Oncocytic types which were uniformly negative for CD56.
In this study, among the Non-neoplastic lesions, 89.4% of cases showed CD56 positivity. This observation was statistically significant with a p-value of 0.011. Golu I et al., noted that 93.3% of Non-neoplastic cases showed CD56 positivity which was statistically significant [12]. In a study conducted by Durmus SE et al., all cases of nodular hyperplasia showed positive CD56 expression [13]. Similar observations were obtained by Demellawy D et al., Nechifor-Boila A et al. and Alshenawy HAS [11,14,15].
In the present study, E-cadherin loss and CD56 negativity were statistically significant with a p-value of 0.0001. This is similar to the study done by Ozolins A et al., where the specificity and PPV for CD56 were 100%. Its sensitivity and NPV were around 80% [6]. The present study is in concurrence with the study by Ceyran AB et al., who also noted that CD56 is the marker with the highest specificity. They also concluded that the marker with the highest sensitivity and specificity was CD56 [8].
Pyo JS et al., in a meta-analytic study, concluded that the rate of loss of CD56 expression were significantly higher in malignant thyroid tumours especially PTC than in other benign lesions like benign follicular nodules and Hashimoto thyroiditis. Thus, they elucidated that in thyroid lesions CD56 as a single marker can be useful for differentiating PTC from Follicular adenoma in daily practice [16]. Dunderovic D et al., also compared the value of a single IHC marker and panels in differentiating benign from malignant thyroid lesions. Their data supported that CD56 is the most specific marker among single IHC marker [17]. Comparison of the expression of IHC markers E-cadherin and CD56 in this study and various other studies were done [Table/Fig-12,13] [6-8,11-15,18-20].
Immunohistochemical expression of E-Cadherin; comparison with other studies [6-8,18,19].
| Author | Year | Country | Antibody | Total PTC cases | E-cadherin loss (%) |
|---|
| Naito A et al., [7] | 2001 | Japan | HECD-117 (Takaro Shazo) | 53 | 79% |
| Kapran Y et al., [18] | 2002 | Turkey | NCH-38 (Dako) | 41 | 80% |
| Ozolins A et al., [6] | 2010 | Latvia | NCH-38 (Dako) | 25 | 92% |
| Ceyran AB et al., [8] | 2015 | Turkey | GMO16 (Genemed) | 101 | 92.1% |
| Harb OA et al., [19] | 2019 | Egypt | BZSB (Beijing) | 40 | 62.5% |
| Present study | 2020 | India | NCH-38 (Dako) | 38 | 97.3% |
(NCH-38 is for E-cadherin)
Immunohistochemical expression of CD56; comparison with other studies [6,11-15,20].
| Author | Year | Country | Antibody | Total PTC cases | CD56 negativity (%) |
|---|
| El-Demellawy D et al., [11] | 2008 | Canada | 123C3 (Zymed) | 72 | 100 % |
| Ozolins A et al [6] | 2010 | Latvia | 123C3 (Dako) | 101 | 91.1% |
| Nechifor-Boila A et al., [14] | 2014 | Romania | 123C3 (Dako) | 11 | 81.8% |
| Alshenawy HAS [15] | 2014 | Egypt | 123C3 (Dako) | 22 | 86.3% |
| Radu TG et al., [20] | 2015 | Romania | 123C3 (Dako) | 27 | 100% |
| Durmus SE et al., [13] | 2016 | Turkey | 123C3 (Thermo) | 47 | 68.08% |
| Golu I et al., [12] | 2017 | Romania | 1B6 | 25 | 76% |
| Present study | 2020 | India | 123C3 (Dako) | 38 | 100% |
(123C3 is for CD56)
The present study shows that E-cadherin and CD56 IHC markers are useful in differentiating PTC from benign thyroid lesions and predicting the prognosis.
Limitation(s)
This study could not prove association between E-cadherin expression and prognostic variables because of the limited sample size.
Conclusion(s)
PTC was characterised by decreased or absent expression of cell adhesion molecules like E-cadherin and CD56 compared to the expression in the adjacent thyroid tissue. Among these, the marker with higher specificity was CD56 (100%). In thyroid lesions, CD56 can be used as a single marker for differentiating PTC from other follicular patterned lesions. The non-neoplastic lesions preserved expression of E-cadherin and CD56. CD56 negativity and E-cadherin loss can assist in the decision making.
(NCH-38 is for E-cadherin)
(123C3 is for CD56)