Celiac disease is a type of chronic disease that endures in those carrying halotype DQ2/DQ8 in the body [1]. The initial representation of celiac disease was given by Gee in 1888 [2]. After ingestion of gluten, an afflicted individual observes painful symptoms that appear instantly. The clinical features are abdominal bloating, anaemia, fatigue, abdominal pain, vomiting, skin rashes, diarrhea, failure to thrive, delayed growth, vitamin levels, anxiety, depression, etc., [3]. The manifestations differ from patient to patient and depend upon ppm (parts per million) gluten intake. During the world war, when wheat grain lessens in specific countries, it leads to a decline in certain celiac symptoms [4,5]. So, the notion of gluten-less products was prefaced to grab the celiac disease [6,7]. European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) guidelines [6] assures the tTG-IgA test for celiac diagnosis and if any ambiguous consequence, then proceeds with biopsy procedure for the confirmation of celiac disease. Gut damage is commonly seen in celiac patients with biopsy testing. An individual is also said to be celiac if the HLA DQ2/DQ8 genes is present in the body with gastrointestinal symptoms.
The concept of fuzzy logic was given by Zadeh LA to deal with the problem of intermediate values or non-linear problems in 1965 [8]. A fuzzy system is a type of inference system which-takes input in the form of crisp data and evaluates them by comparing rules stored in the fuzzy database [9]. Mamdani and Sugeno fuzzy types of models can be used for producing a fuzzy knowledge base with different types of the membership function. Triangular and trapezoidal member functions are ordinarily used functions for the formation of fuzzy rules. Subsequently, the process of de-fuzzification produces an output value as the single probable value which is a prediction in terms of health applications [10]. Fuzzy logic is consistently used in recognising chronic diseases such as dental, cholera, liver diagnosis, viral infection, lung diseases, kidney diseases, etc., effectively and accurately. Alongside this, a lot of research has been done on the celiac disease with the help of clinical testing procedures in different countries. Researchers did exceptionally well to accomplish submissions in diagnosing celiac disease with multiple clinical examinations as Tissue transglutaminase (tTG), Endomysial Antibody (EMA), Biopsy and Genetic Testing procedure [11-17].
So, this study was aimed to design a fuzzy logic inference system to predict celiac disease based on individual symptoms in North-Indian patients. The proposed system will abandon a fruitful consequence for entities and physicians for celiac disease disclosure in few seconds without any painful testing strategy.
Materials and Methods
A wheat allergy Camp was organised on 7th April 2019, at DAV College, Amritsar, Punjab, India with the permission of Principal, Dr. Rajesh Kumar and under the guidance of three Gastrointestinal Physicians. The survey was conducted using a questionnaire on 700 individuals, using a random sampling technique. The questionnaire consisted of all the common gastrointestinal symptoms often seen by celiac patients. tTG clinical testing was done for the confirmation of celiac disease under the guidance of three gastrointestinal physicians [6]. The Body Mass Index (BMI) evaluation was also done, along with relevant family and medical history.
Sample size calculation: The sample size considered was based on the area of the population. The population of Amritsar is 11.3 lacs given in Census report published in 2011. So, Cochrane’s sample size calculation was:
x= ((Z2* pop(1-pop))/er2)/ (1+(Z2 * pop(1-pop))/er2 No.), where,
x, is the total sampling unit to be taken,
Z, is the confidence level of up to 95% (Z=1.96),
Pop, is the sample population with 0.5 approximation
Er, is the error rate with 0.05 approximation
No. is the total population of the area to be examined.
x=((1.962*0.5(1-0.5))/0.052)/(1+(1.962*0.5(1-0.5))/0.052*1132383)
x=384.029
It requires only approx. 400 records for the dataset, but 700 instances were collected to develop a fuzzy system with optimisation.
Inclusion criteria: Participants who were willing to be a part of this survey under the guidance of three gastrointestinal physicians.
Exclusion criteria: Participants with other existing chronic diseases were excluded from the study.
All the participants were subjected to general physical examination such as height, weight, BMI (as weight in kg, height in meter2) and the same was recorded in the questionnaire. For BMI, individuals were divided into groups as Underweight (17.0-18.4 kg/m2), Healthy Normal (18.5-24.9 kg/m2), Overweight (25.0-29.9 kg/m2), and Obese (≥30 kg/m2).
The detail of celiac patients with values as never, mild, moderate, and severe were presented in the questionnaire for abdominal pain, abdominal bloating, anaemia, diarrhea, acidity, etc.
The questionnaire also consisted of a question on awareness concerning the celiac disease with three formal inputs as Aware, Not Aware, and Somewhat Aware.
Statistical Analysis
The data was analysed using Statistical Package for the Social Sciences (SPSS) software with principal component analysis and factor analysis for diminishing uncommon symptoms. For the implementation of a fuzzy celiac inference system, Python software was used to get the single probabilistic value with multiple predefined modules. To check the performance of the system, 700 records to be fed up to the fuzzy system to obtain sensitivity and specificity.
Results
From the questionnaire data, the primary objective was to classify the most common symptoms among all in celiac patients to formulate a fuzzy logic predictive system. A total of 700 individuals who participated in the survey, with 134 celiac patients were confirmed. The mean age was found to be 21.72, with a standard deviation of 10.685.
[Table/Fig-1] shows symptomatic values given by celiac patients. The most common symptoms were abdominal pain, diarrhea, anaemia, vomiting, and weight loss reported by celiac patients from the survey.
Analysis of celiac symptoms with attributes.
| Symptoms (Existing patients) | Never | Mild | Moderate | Severe |
|---|
| Abdominal pain | 0 | 12 | 25 | 97 |
| Abdominal bloating | 40 | 66 | 12 | 17 |
| Anaemia | 1 | 4 | 57 | 72 |
| Diarrhea | 3 | 8 | 24 | 99 |
| Acidity | 66 | 58 | 8 | 2 |
| Headache | 60 | 66 | 7 | 1 |
| Bone or joint pain | 76 | 45 | 8 | 5 |
| Defective tooth enamel | 81 | 40 | 10 | 3 |
| Vomiting | 3 | 27 | 43 | 61 |
| Fatigue (Weakness) | 3 | 25 | 48 | 58 |
| Constipation | 77 | 46 | 7 | 4 |
| Irritability | 59 | 48 | 18 | 9 |
| Anxiety | 60 | 61 | 7 | 6 |
| Skin rash | 77 | 28 | 15 | 14 |
| Weight loss | 0 | 8 | 126 |
| Delayed growth | 16 | 48 | 38 | 32 |
The 0-18 age-group attained a maximum number of 104 celiac patients from overall 134 celiac patients. It registers the early intake of wheat and breastfeeding, a vital role for the ingredients in the diet. Few celiac patients were also confirmed in other age-groups, as depicted in [Table/Fig-2].
Celiac patient record with age-groups.
| Age group (years) | Total |
|---|
| 0-18 | 18-35 | 35-60 | 60-100 |
|---|
| Celiac patient | No | 172 | 326 | 64 | 4 | 566 |
| Yes | 104 | 10 | 15 | 5 | 134 |
| Total | 276 | 336 | 79 | 9 | 700 |
It is also noteworthy to focus on celiac patient’s gender-wise records. From the survey data, 75 female celiac patients were found against 59 males, as shown in [Table/Fig-3].
Celiac patients with gender records.
| Celiac patient | Total |
|---|
| No | Yes |
|---|
| Gender | Female | 232 | 75 | 307 |
| Male | 334 | 59 | 393 |
| Total | 566 | 134 | 700 |
Finally, the survey settled with the awareness level of celiac disease in Punjab, represented in [Table/Fig-4]. Majority (46.71%) of the patients were not aware of celiac disease.
Awareness with age-groups.
| Age group (years) | Total |
|---|
| 0-18 | 18-35 | 35-60 | 60-100 |
|---|
| Awareness | Not aware | 111 | 168 | 47 | 1 | 327 |
| Somewhat aware | 31 | 84 | 3 | 0 | 118 |
| Aware | 134 | 84 | 29 | 8 | 255 |
| Total | 276 | 336 | 79 | 9 | 700 |
Based on these symptomatic conclusions, the idea of developing a fuzzy logic system was proposed to diagnose celiac disease using intelligent rather than a clinical approach. The development of a fuzzy logic system to detect celiac disease was implemented in PyCharm by importing various existing modules for evaluation and fuzzy graphical notation. The collections of symptoms were analysed from the SPSS tool to find out the most common symptoms achieved from the survey. The selection of vital parameters defined in the proposed system with six input parameters as anaemia, diarrhea, abdominal pain, vomiting, BMI, weight loss with a relevant range. The evaluation of all the input parameters defined using the triangular membership function for the fuzzy inference system. Crisp inputs were devised based on symptomatic nature using fuzzy values that differ according to the range. The fuzzy database constitutes of fuzzification process with a fuzzy if-then rule-based environment. Every input in the system is in the fuzzy act as antecedent and its outcome in the form of the consequent.
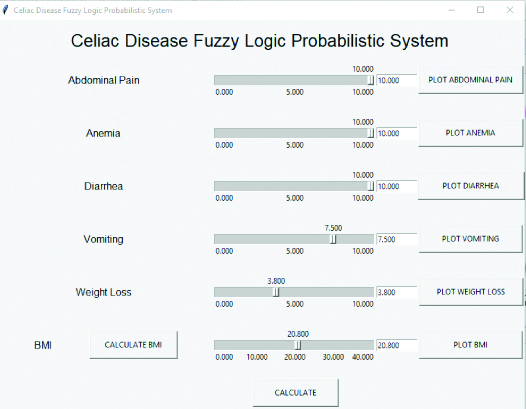
The scenario renders information with crisp values in numerical notation input to the fuzzy system as abdominal pain, anaemia and diarrhea to 10 points, vomiting to 7.5 with BMI 20.8, weight loss as 3.8 to the fuzzy logic probabilistic system as presented in [Table/Fig-5]. The input variables that have been practiced in the order, executed using a triangular membership function. It consists of multiple crisp values for each fuzzy variable, as abdominal pain with crisp values range; Mild (0-4), Moderate (1-9) and Severe (6-10). The entire range of severity of disease with symptoms is stewarded from 0-10 using triangular evaluation.
Celiac disease fuzzy logic inference system.
The outcome was 95.53873% according to the input given by an individual portrayed in [Table/Fig-6] with recommendations. The outcome signifies an individual with a strong chance of celiac disease based on the output. The output from the fuzzy system using the de-fuzzification technique accompanies the ESPGHAN guidelines by weightage given to every symptom [6]. It also prescribes the strong chance of celiac disease to avoid gluten in the diet and for the final confirmation must proceed with the tTG-IgA test.
Celiac disease fuzzy logic outcome.

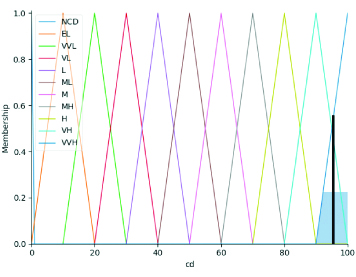
The fuzzy graph outline in [Table/Fig-7] betokens fuzzy rules matched at the maximum with the entire fuzzy database. The process of de-fuzzification based on the area of maximum using different AND, OR combinations. Through the fuzzy logic system, it is possible to predict celiac disease with symptomatic information.
Celiac disease fuzzy logic graph.
NCD: Non-celiac disease; EL: Extremely-low; VVL: Very-very-low; VL: Very-low; L: Low; ML: Medium-low; M: Medium; MH: Medium-high; H: High; VH: Very-high and VVH: Very-very-high
To check the accuracy of the fuzzy logic proposed system, every record obtained from the survey feed up to the system. The fuzzy logic system produced accuracy 98.8%, sensitivity 98.5% and specificity 98.39% with minimal error rate as depicted in [Table/Fig-8]. The outcome performance leads and helps physicians to use this proposed system to avoid clinical testing confirmation in comparison with existing fuzzy systems.
Confusion matrix for performance evaluation.
| Actual celiac disease (+) | Actual celic disease (-) |
|---|
| Predicted celiac disease (+) | 132 (TP) | 6 (FP) |
| Predicted celiac disease (-) | 2 (FN) | 560 (TN) |
TP: True positive; FP: False positive; FN: False negative; TN: True negative
Discussion
Fuzzy logic is consistently used in recognising chronic diseases effectively and accurately. Various researchers deal with similar predictive systems with identical diseases using a fuzzy logic approach. Adeli M and Zarabadipour H fetched samples from the University of California, Irvine, (UCI) Machine Learning Repository and obtained 80% accuracy in detecting chronic diseases using the pattern recognition routine with fuzzy logic [18]. Parewe AM et al., admitted the hybrid fuzzy logic system with dental disease detection, achieved 82% accuracy [19]. Uduak A and Mfon M offered cholera diagnosis using fuzzy logic in 2013 with Matrix Laboratory (MATLAB) tool to prophesy the disease [20]. Liver diagnosis has been reported using fuzzy logic by Hashmi A and Khan MS, with three diverse types of liver diseases been realised by the fuzzy system [21]. Kaur R et al., proposed viral infection recognition using fuzzy logic with six different parameters to automate the system [22]. The symptomatic study has been characterised by Manikandan T et al., with the prediction of lung diseases using fuzzy logic with 95% accuracy of the system [23]. Recently in 2018, Zarandi MH and Abdolkarimzadeh M aimed a fuzzy expert system for diagnosing kidney disease in Iran on 400 specimens to differentiate chronic kidney or non-chronic disease patients having 80% accuracy [24]. So, there is a necessity to compose such intelligent systems to investigate diseases based on symptoms [25-27].
Limitation(s)
The limitation of the fuzzy system is that it is based on six input parameters with a specific range of every sign. Alongside this, the total number of instances for a more accurate system can be formulated with data from other geographical locations to get more accurate awareness and prevalence levels of celiac disease.
Conclusion(s)
The fuzzy logic system produced 98.8% accuracy, 98.5% sensitivity and 98.39% specificity with minimal error rate. The prevalence of celiac disease obtained a 1:19 ratio from the survey in Punjab with 134 celiac patients. The collected set of data from the survey elucidates that the female ratio carrying celiac disease is much more as compared to males. Few parameters like abdominal pain and varied BMI having vital inputs for the system as it resembles with all present celiac patients. As multiple expert systems accessible everywhere in the world for diagnosis of various diseases, fuzzy logic will be satisfactory to diagnose celiac disease. Due to sharpness in every specialty of medicine, fuzzy logic is associated with formulating intelligent machines for the determination of diseases. In this proposed system, it is ostensible that celiac disease can be foretold with symptoms. In the future, the system can be expanded with more than six parameters to predict celiac disease with a more precise nature as symptoms might vary in sophisticated individuals.
TP: True positive; FP: False positive; FN: False negative; TN: True negative