Secondary Vesical Calculus caused by Transmigration of Intrauterine Device: A Case Report
Akshay Bahadur1, Yanshul Rathi2, Om Yadav3
1 Head, Department of Surgery, Dr. Hedgewar Arogya Sansthan, Karkardooma, Delhi, India.
2 Senior Resident, Department of Surgery, Dr. Hedgewar Arogya Sansthan, Karkardooma, Delhi, India.
3 Senior Resident, Department of Surgery, Dr. Hedgewar Arogya Sansthan, Karkardooma, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Yanshul Rathi, House No. B-109, Ganga Vihar, Delhi, India.
E-mail: dryanshulrathi@gmail.com
Intrauterine Contraceptive Device (IUCDs) are among the popular methods having results comparable to tubal ligation contraception method among the women. Some; not common but serious complications by its insertion may be encountered in the clinical practice like uterine perforation which may lead to its migration to adjacent organs which in turn leads to bladder stone formation being one among them. An uncommon case of a 45-year-old female patient presented with a stone formation around a migrating intrauterine device (Copper-T). The lady presented with a 4-year history of irritative voiding symptoms and occasional terminal haematuria for which she received treatment from time to time but her symptoms persisted. She had a history of a Copper-T inserted 18 years ago in one of the primary health centre in Punjab. She also gave history of tubal ligation 3 years after the insertion of Copper-T. Her X-ray Kidney Uretere and Bladder (KUB) showed a large radio-opaque vesical calculus with a part of T loop IUCD protruding through it. Ultrasonogram of the pelvis revealed a bladder calculus. Suprapubic cystolithotomy was performed and a vesical calculus with embedded Copper-T was retrieved. The postoperative period was uneventful. Awareness about proper insertion of intrauterine device through trained persons, its time of insertion (chances of uterine perforation being more during puerperium), proper counselling in patients going for IUCD insertion (the significance of missing thread) and the use of newer contraceptive device causing less complication is overemphasised in the present case report.
Bladder stone, Copper-T, Intravesical migration
Case Report
A 45-year-old multiparous female patient was referred from a private Gynaecologist with a 4-year history of on and off lower abdominal pain, irritative voiding symptoms and occasional terminal haematuria with no obstructive features. She had no associated fever, vaginal discharge, irregular vaginal bleeding or retention of urine.
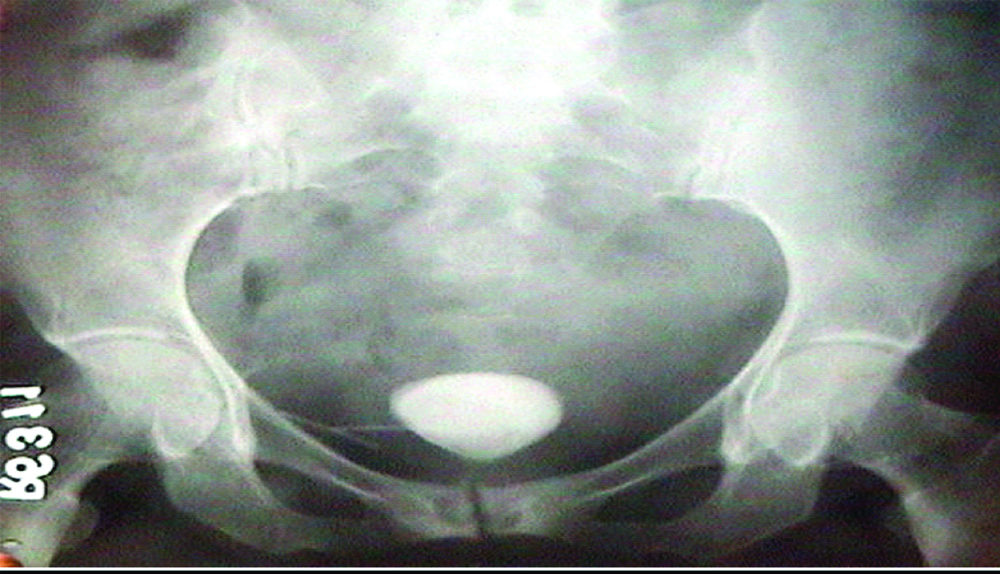
The patient had a Copper-T inserted 18 years ago in a primary health centre of District Cathal, Punjab. She never went to any doctor for the follow-up of IUCD. The patient underwent tubal ligation 3 years after the insertion of copper-T concealing her history of contraceptive device insertion throughout. For 14 years, after insertion of the Copper-T, she remained asymptomatic. For the past four years, however, she received treatment for urinary tract infection for her symptoms but it did not get subsided. Physical examination of the patient revealed a female of average built with mild pallor. Abdominal examination revealed suprapubic sensitivity with no palpable abdominal mass. On per vaginal examination no Copper-T thread was seen, uterus being anteverted, cervix was soft with no discharge. Per rectal and proctoscopy revealed no abnormalities, no foreign body (Copper-T) seen. Her haemogram showed normocytic normochromic anaemia. Her blood urea, blood sugar and serum electrolytes were within normal limits. Urine analysis showed pus cells and micro-haematuria. Urine culture and sensitivity showed the species of Klebsiella sensitive to Gentamycin and Ofloxacin. X-ray KUB showed a large radio-opaque vesical calculus with a part of T loop of IUCD protruding from it [Table/Fig-1]. Suspecting it to be a IUCD because of its T-shaped structure on eliciting the history patient admitted the fact of undergoing Copper-T insertion. A pelvic ultrasonography revealed a urinary bladder calculus. Patient was subjected to suprapubic cystolithotomy and a stone of 4.5 cm × 4.0 cm size with protruding T loop of intrauterine device was retrieved [Table/Fig-2]. There were no fibrous adhesions between the urinary bladder and the uterus and no obvious fistula connecting the uterus to the bladder was found. No growth or diverticula were seen in the bladder. Primary closure of the bladder was done and the patient made an uneventful postoperative recovery.
X-ray image of kidney, ureter and bladder region showing the presence of single large stone with a linear opaque extension suspicious of foreign body (which might acted as a nidus for stone formation).
Postoperative image of the retrieved vesical calculus (of size 4.5*4 cm), formed around the vertical limb of intrauterine contraceptive device.

Discussion
Intrauterine contraceptive device is considered to be an effective and reliable method of achieving contraception for family planning in developing countries. The efficacy is comparable to tubal ligation in terms of pregnancy rate. Copper containing intrauterine devices produce both morphological and biochemical changes in the reproductive tract [1]. They induce a sterile inflammatory response in the endometrium and modify various enzymes needed for implantation. They also bring some changes in the DNA cellular content, glycogen metabolism and uptake of oestrogens by the endometrium [1].
Intrauterine devices have been plagued by many early and late complications, including uterine perforation and migration into adjacent structures, bowel perforation and vesicouterine fistula formation [2]. Complications such as pregnancy, uterine perforation and migration into adjacent organs like peritoneum, omentum, appendix, colon and wall of iliac vein have been reported [2]. However, migration of an intrauterine device into the urinary bladder with secondary vesical stone formation is a rare complication [3]. Migration both, within months and years after its insertion has been reported [4,5].
Although perforation of the uterus by an intrauterine device ranges from less than 1 in 1000 to no more than 9 in 1000 i.e., Uterine perforation has been reported in 0.1% of cases [6]. Intravesical migration to urinary bladder with secondary stone formation is a rare complication. The explanations regarding the migration have been given differently by different learned people. These can be summarised as an iatrogenic uterine perforation which was overlooked, uterine contraction suddenly and spontaneously, involuntary bladder contraction, gut peristalsis and movement of the peritoneal fluid [7]. In this reported case, the mechanism and timing of the migration cannot be ascertained.
Recurrent urinary tract infection viz., cystitis here, which in turn invoked due to the presence of the migrated contraceptive device in the bladder promoted stone formation. Factors contributing to the possibility of uterine perforation are incompetent insertion or positioning, fragility of the uterine wall due to recent birth, abortion, or pregnancy [8].
There are few similar case report which shows that the IUCD (Copper-T) migrated into the urinary bladder leads to calculus formation [9]. Satta S et al., reported a series of 10 women in whom an intrauterine contraceptive Copper-T device migrated from the uterus to the bladder and resulted in the formation of a stone. Cystoscopy was performed which shows, among nine cases there was the partial intravesical position of the intrauterine contraceptive device and in one case an entire intravesical intrauterine contraceptive device with the formation of calculus (all cases). Endoscopic lithotripsy of the stone with the extraction of the intrauterine contraceptive device was performed in all patients [10].
Pre-operative counselling in patient going for intrauterine device insertion including the significance of missing thread should be the priority of health worker. Contraceptive device which is new and causing a smaller amount of complication, like lower-dose oral contraceptive pills, new oral progestogens, progestogen implants, a progestogen-bearing intrauterine device and polyurethane female condoms may be favoured to Copper containing intrauterine device.
Conclusion(s)
A female patient with persistent or refractory urinary tract symptoms should be asked the history of any contraceptive device insertion particularly copper-based, like in the present case it was copper-T. Although the intravesical migration of the contraceptive device may remain asymptomatic for many years; maybe for decades. A high index of suspicion is necessary to avoid the long term morbidity and litigations. The purpose of presenting this case is to highlight the significance of following-up even asymptomatic women with IUCDs.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jan 17, 2020
Manual Googling: Feb 18, 2020
iThenticate Software: May 29, 2020 (14%)
[1]. Oster GK, Reaction of metallic copper with biological substrate natureFebril steril 1971 234:25310.1038/234153a04942679 [Google Scholar] [CrossRef] [PubMed]
[2]. Moore PJ, Bowel perforation by the multiload Cu 250 intra-uterine contraceptive deviceS Afr Med J 1982 62(14):489-90. [Google Scholar]
[3]. De Silva WSL, Kodithuwakku KASUA, Aponsu GUE, Rathnayake RMM, Rajasegaram E, A large bladder stone caused by the intravesical migration of an intrauterine contraceptive device: A case reportJ Med Case Rep 2017 11(1):29310.1186/s13256-017-1461-629058619 [Google Scholar] [CrossRef] [PubMed]
[4]. Maskey CP, Rahman M, Sigdar TK, Johnsen R, Vesical calculus around an intra-uterine contraceptive deviceBr J Urol 1997 79(4):654-55.10.1046/j.1464-410X.1997.00165.x9126106 [Google Scholar] [CrossRef] [PubMed]
[5]. Dietrick DD, Issa MM, Kabalin JN, Bassett JB, Intravesical migration of intra-uterine deviceJ Urol 1992 147(1):132-34.10.1016/S0022-5347(17)37159-8 [Google Scholar] [CrossRef]
[6]. Rowlands S, Oloto E, Horwell DH, Intrauterine devices and risk of uterine perforation: current perspectivesOpen Access J Contracept 2016 7:19-32.10.2147/OAJC.S8554629386934 [Google Scholar] [CrossRef] [PubMed]
[7]. Shin DG, Kim TN, Lee W, Intrauterine device embedded into the bladder wall with stone formation: Laparoscopic removal is a minimally invasive alternative to open surgeryInternational Urogynecology Journal 2012 23(8):1129-31.10.1007/s00192-011-1632-822189515 [Google Scholar] [CrossRef] [PubMed]
[8]. Junceda Avello E, Gonzalez Torga L, Lasheras Villanueva J, De Quiros A GB, Uterine perforation and vesical migration of an intrauterine device. Case observationActa Ginecol (Madr.) 1977 30(2):79-86. [Google Scholar]
[9]. Aggarwal S, Jindal RP, Deep A, Intravesical migration of intrauterine contraceptive devices with stone formationJ Family Med Prim Care 2014 3(4):449-51.10.4103/2249-4863.14814725657964 [Google Scholar] [CrossRef] [PubMed]
[10]. Sataa S, Sami BR, Sabeur R, Karim C, Ali H, Bladder calculus resulting from the migration of an intrauterine contraceptive device: A report of ten casesInt J Nephrol Urol 2011 3:54-61. [Google Scholar]