Tobacco use is today’s major public health concern in our country, which can be largely reduced solely by primordial and primary prevention. Around more than eight million people lose their lives due to tobacco use and more than seven million of these deaths are because of direct tobacco use and approximately 1.2 million die from second-hand smoke. The burden of tobacco-related illness and death is heaviest in low- and middle-income countries worldwide, where around 80% of the 1.1 billion smokers live [1].
The families of tobacco users face a lot of social and financial problems due to premature death of tobacco users [2]. Globally, around 30% of cancers occur due to tobacco use, and the economic burden due to tobacco-related illnesses is more than total expenditures on health annually in low and middle-income countries [3]. According to National Family Health Survey-4, 44.5% of male and 6.8% of female use any kind of tobacco in India [4]. In view of the public health importance of harmful use of tobacco related consequences, it is important to regularly analyse the pattern and trend of tobacco consumption. One of the co-author has published a study on prevalence and correlates of tobacco use in rural areas of Haryana, present study was carried out to determine the prevalence and socio-demographic determinants of tobacco use in urban area (Rohtak city) of Haryana, India [5].
Materials and Methods
The study was a community based observational study with cross-sectional design. The study was conducted among 15-64 years aged individuals in Rohtak city of Haryana, from September 2013 to October 2014. Department of Community Medicine Pt.BD Sharma PGIMS, Rohtak, Haryana, India, also caters to selected areas of the city as field practice area besides carrying out teaching, training and research activities for medical undergraduate and postgraduate students. Ethical approval to conduct the study was taken from Institution Ethics Committee (IEC).
Sample Size and Sampling Strategy: The sample size as per calculation was 1329 individuals using formula N=4PQ/L2 where, P=Prevalence, Q=1-P and L=Allowable error of P, considering the prevalence of one of the important risk factor of non-communicable diseases i.e., smoking 7% [6] with confidence level of 95% and 20% allowable error. Though the calculated sample size was 1329 individuals but 1440 study participants were selected for the present study to have adequate sample. All the persons of 15-64 years age group willing to participate and who did not fall in exclusion criteria (not willing to participate, migrants, bed ridden patients, pregnant females) were included in the study. For the purpose of ICDS scheme, Rohtak city was divided into eight different circles. Multistage random sampling was carried out including all the anganwadi centres located in these eight different circles. From each circle, two anganwadi centres were selected randomly i.e., total 16 anganwadi centres were selected for the present study.
For selecting individuals from each selected anganwadi, sex wise enumeration was done for all five sub age groups (15-24, 25-34, 35-44, 45-54 and 55-64 years) of the study population from the anganwadi registers of respective anganwadi. From each anganwadi, 90 individuals of 15-64 years age group (subdivided into five sub age groups) were selected by taking 18 individuals (9 males and 9 females) of each age bracket by systematic random sampling. Thus, a sample size of 1440 was included in the study. Only one individual was interviewed from each house. Study subjects were contacted and interviewed through house to house visits by the investigator herself using a pretested, semistructured schedule (based upon Integrated Disease Surveillance Project for non-communicable disease risk factors survey 2007-08). In case, the selected study subject was not available in any house of respective anganwadi area, subsequent house was included in the study. The data were collected regarding socio-demographic variables (age, gender, education, occupation, socioeconomic status), tobacco use (age at which first started, currently using, number of times/day, age at which stopped using, reason for initiation), physical measurements (weight, height, blood pressure, waist circumference, hip circumference). Socio-economic status of study population was assessed using Kuppuswamy’s socio-economic status scale for urban areas [7]. Written and informed consent was obtained from all the subjects before initiating the interview.
Current Smoker/Smokeless Tobacco User was defined as a person who at the time of the survey, smokes/uses tobacco in any forms either daily or occasionally [8].
Statistical Analysis
Collected data was entered in the Excel spreadsheet and analysis was carried out using Statistical Package for Social Studies (SPSS) version 20.0. Pearson’s chi-square test and fisher-exact test were used to evaluate differences between groups for categorised variables. Student’s t-test and logistic regression analysis was done to evaluate factors associated with tobacco intake. All tests were performed at a 5% level of significance, thus an association was significant if the p-value was <0.05.
Results
[Table/Fig-1] shows that all study participants were equally distributed by age and sex. More than half (56.4%), of the subjects were unemployed, which meant they were either pursuing their studies or not physically fit to work being old people or housewives and were not contributing economically to the family, followed by participants of other occupations such as business (22.8%), service (government/private) (16.5%) and labourers (4.3%).
Distribution of study subjects by socio-demographic characteristics (N=1440).
| Characteristics | Frequency | Percentage |
|---|
| Gender |
| Male | 720 | 50% |
| Female | 720 | 50% |
| Age group (in years) |
| 15-24 | 288 | 20% |
| 25-34 | 288 | 20% |
| 35-44 | 288 | 20% |
| 45-54 | 288 | 20% |
| 55-64 | 288 | 20% |
| Occupation |
| None | 812 | 56.4% |
| Labourer | 62 | 4.3% |
| Business | 328 | 22.8% |
| Service | 238 | 16.5% |
| Educational status |
| Illiterate | 24 | 1.7% |
| Primary | 133 | 9.2% |
| Middle | 304 | 21.1% |
| Senior secondary | 505 | 35.1% |
| Graduate and above | 474 | 32.9% |
| Socio-economic status* |
| Upper | 38 | 2.6% |
| Upper middle | 501 | 34.8% |
| Lower middle | 389 | 27.0% |
| Upper Lower | 484 | 33.6% |
| Lower | 28 | 1.9% |
*Modified kuppuswami socioeconomic scale
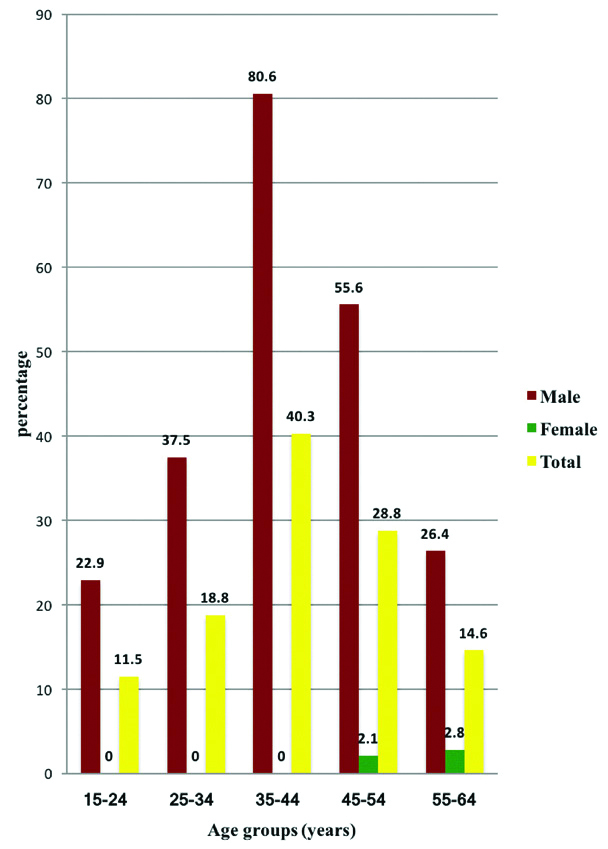
As shown in [Table/Fig-2] overall prevalence of current tobacco-smoking was found to be 22.8% (328/1440) and it was mainly among males (44.6%) and almost negligible among females (1.0%) in the study area. Among males, it increased from 22.9% in 15-24 years age group to 80.6% in 35-44 years age group and then decreased in 45-54 years age group (55.6%) and 55-64 years age group (26.4%). There was an increase in prevalence of tobacco smoking with age in females. Among females, maximum prevalence was seen in 55-64 years age group (2.8%). In 15-24, 25-34 and 35-44 years age group none had reported the current smoking. This difference in age groups was found to be statistically significant among both males (p=0.001) and females (p=0.027) by applying Pearson’s chi-square test.
Prevalence of current tobacco-smoking use among study participants by age groups and gender (N=1440).
[Table/Fig-3] shows the overall prevalence of current smokeless tobacco use was found to be 3.0% (43/1440) and it was only among males (6.0%) while no female was reported to be having smokeless tobacco use. Among males, it increased from 4.9% in 15-24 years age group to 10.4% in 25-34 years age group and none had reported in 55-64 years age group.
Prevalence of current smokeless tobacco use among respondents by age and sex.
| Age group (years) | Current smokeless tobacco users |
|---|
| Male (n=720) | Female (n=720) | Total (N=1440) |
|---|
| 15-24 | 7/144 (4.9) | 0/144 (0.0) | 7/288 (2.4) |
| 25-34 | 15/144 (10.4) | 0/144 (0.0) | 15/288 (5.2) |
| 35-44 | 14/144 (9.7) | 0/144 (0.0) | 14/288 (4.9) |
| 45-54 | 7/144 (4.9) | 0/144 (0.0) | 7/288 (2.4) |
| 55-64 | 0/144 (0.0) | 0/144 (0.0) | 0/288 (0.0) |
| Total | 43/720 (6.0) | 0/720 (0.0) | 43/1440 (3.0) |
| p-value | 0.001* | - | 0.001* |
*Fisher-exact test
(Figures in parentheses indicate percentages)
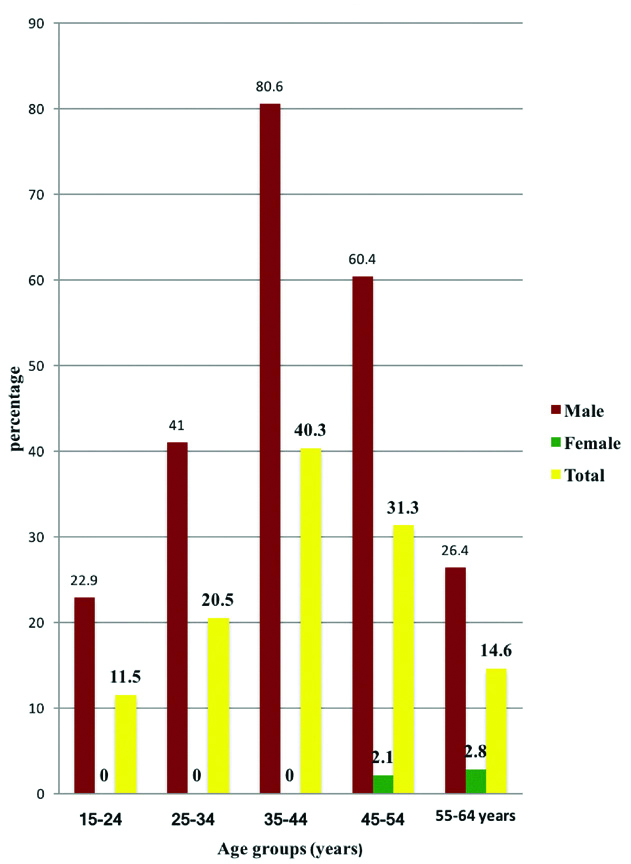
As shown in [Table/Fig-4] overall prevalence of current tobacco use was 23.6% (340/1440) and it was found to be higher among males (46.3%) as compared to females (1.0%). The prevalence of current tobacco use was found to be highest among 35-44 years age group among males (80.6%) and in 55-64 years age group among females (2.8%). The observed difference was statistically significant in age groups among males (p=0.0001) and females (p=0.027) by applying Pearson’s chi-square test.
Prevalence of current tobacco use (smoking + smokeless) among study participants by age groups and gender (N=1440).
Males used tobacco because of curiosity or peer pressure (85%), imitation of other family members (5.0%), relieving acidity/ tiredness (4.3%) and loneliness (3.7%) while females used tobacco for relieving acidity.
The [Table/Fig-5] shows that mean age for initiation of smoking tobacco and smokeless tobacco among study participants was 20.92 and 24.05 years, respectively. The mean age for smoking was observed to be lower among males (20.55 years) as compared to females (41.14 years). There was striking observation of not even a single female indulged in use of smokeless tobacco.
Age of initiation for tobacco among study population.
| Variables | Mean±SD (years) |
|---|
| Age of initiation for smoking |
| Male | 20.55±7.92 |
| Female | 41.14±13.75 |
| Total | 20.92±8.48 |
| Age of initiation for smokeless |
| Male | 24.05±9.03 |
| Female | - |
| Total | 24.05±9.03 |
The [Table/Fig-6] shows that mean number (on a smoking day) of smoking-tobacco, smokeless tobacco among study participants were found to be 13.3 and 4.2, respectively. The mean number of smoking was almost similar for both males and females.
Average frequency of tobacco use on day of use among users.
| Variables | Mean±SD |
|---|
| Average times smoking (on a smoking day) |
| Male | 13.3±12.2 |
| Female | 14.0±7.2 |
| Total (N=328) | 13.3±12.1 |
| Average times smokeless (on the day of use) |
| Male | 4.2±4.1 |
| Female | - |
| Total (N=43) | 4.2±4.1 |
The [Table/Fig-7] shows that the prevalence of current tobacco smoking use with the mentioned socio-demographic variables was found to be statistically significant. Males were 56 times (aOR:56.4, CI:23.51-135.12, p-0.001) more likely to smoke than females. Age was also a very important predictor of current smoking status which showed an increasing trend with 35-44 years age group 3.5 times (aOR:5.16,CI: 2.64-10.09, p-0.001) more likely to occur than in 15-24 years. Business category (aOR: 4.94, CI:2.80-8.74, p-0.001) and lower socio-economic status (aOR:38.04, CI: 14.85-66.87, p-0.001) have also shown a positive association with current smoking status.
Independent association of socio-demographic variables with current tobacco smoking (N=1440).
| Variables | Current smoking | |
|---|
| Prevalence (%) | aOR(C.I.) | p-value |
|---|
| Gender |
| Female | 7/720 (1.0) | Reference | |
| Male | 321/720 (44.6) | 56.36 (23.51-135.12) | 0.001* |
| Age group (years) |
| 15-24 | 33/288 (11.5) | Reference | |
| 25-34 | 54/288 (18.8) | 0.86 (0.45-1.63) | 0.632 |
| 35-44 | 116/288 (40.3) | 5.16 (2.64-10.09) | 0.001* |
| 45-54 | 83/288 (28.8) | 2.33 (1.22-4.43) | 0.010* |
| 55-64 | 42/288 (14.6) | 0.95 (0.49-1.83) | 0.877 |
| Educational status |
| Illiterate | 2/24 (8.3) | Reference | |
| Primary | 38/133 (28.6) | 0.91 (0.10-8.22) | 0.934 |
| Middle | 115/304 (37.8) | 0.61 (0.07-5.38) | 0.658 |
| Senior secondary | 108/505 (21.4) | 0.38 (0.04-3.27) | 0.378 |
| Graduate and above | 65/474 (13.7) | 0.25 (0.02-2.15) | 0.207 |
| Occupation |
| None | 35/812 (4.3) | Reference | |
| Labourer | 22/62 (35.5) | 1.57 (0.069-3.57) | 0.279 |
| Business | 195/328 (59.5) | 4.94 (2.80-8.74) | 0.001* |
| Service | 76/238 (31.9) | 1.93 (1.03-3.63) | 0.040* |
| Socio-economic status |
| Upper | 0/38 (0) | Reference | |
| Upper middle | 110/501 (22.0) | 20.6 (8.47-26.98) | 0.001* |
| Lower middle | 95/389 (24.4) | 22.9 (9.49-37.52) | 0.001* |
| Upper Lower | 114/484 (23.6) | 21.8 (9.80-33.60) | 0.001* |
| Lower | 9/28 (32.1) | 38.4 (14.85-66.87) | 0.001* |
*Logistic Regression analysis
aOR(CI)=Adjusted Odds Ratio (Confidence Interval)
The [Table/Fig-8] revealed that p-value for weight (64.20±14.51 vs 61.34±14.27 kg, p=0.002), height, BMI (23.61±4.70 vs 24.44±5.27 kg/m2, p=0.01), was statistically significant on comparison of current tobacco-smokers to non-smokers.
Comparison of various quantitative variables with current tobacco-smoking use (N=1440).
| Variables | Current tobacco-smoking users (N=328) | Current tobacco-smoking non users (N=1112) | p-value |
|---|
| Weight (kg) | 64.20±14.51 | 61.34±14.27 | 0.002* |
| Height (cm) | 164.59±6.86 | 158.38±9.03 | 0.001* |
| BMI (kg/m2) | 23.61±4.70 | 24.44±5.27 | 0.01* |
| SBP(mmHg) | 128.12±16.31 | 123.40±19.08 | 0.001* |
| DBP(mmHg) | 84.32±10.11 | 80.47±11.3 | 0.001* |
| WC (cm) | 85.67±13.54 | 82.80±14.26 | 0.001* |
| HC (cm) | 91.83±9.13 | 92.91±10.71 | 0.072 |
| Age (years) | 41.25±12.00 | 39.62±15.51 | 0.045* |
*Student t-test
BMI: Body mass index; SBP: Systolic blood pressure; DBP: Diastolic blood pressure; WC: Waist circumference; HC: Hip circumference
No significant difference was observed between Hip Circumference (HC) of current tobacco-smokers and non-smokers (91.83±9.13 vs 92.91±10.71 cm, p=0.072). Waist Circumference (WC) (85.67±.13.54 vs 82.80±14.26; p=0.001), Systolic Blood Pressure (SBP) (128.12±16.31 vs 123.40±19.08 mmHg, p=0.001), Diastolic Blood Pressure (DBP) (84.32±10.11 vs 80.47±11.32 mmHg, p=0.001) was also significantly higher in smokers.
Discussion
Prevalence of Current Tobacco-Smoking Use
In the present study prevalence of current tobacco-smoking was 22.8% and it was more among males (44.6%) and almost negligible among females (1.0%). From the above, it might be inferred that smoking among males is a common phenomenon which is accepted universally in our social norms and socially unacceptable among females. The mean age for smoking was observed to be lower among males (20.55 years) as compared to females (41.14 years), show that male indulged more in these unhealthy habits which could be because of frequent movements, curiosity, experimentation, peer pressure, special occasions like parties, marriage functions etc., and also because of less inhibition due to social and financial independence. Comparison of various studies on current tobacco smoking is shown in [Table/Fig-9] [6,9-18].
Comparison of various studies on prevalence of current tobacco smoking [6,9-18].
| Author name | Publication year | Sample size and study area | Prevalence of current tobacco-smoking | Comparison with current study |
|---|
| Prasad DS et al., [9] | 2012 | 1178, Orissa, India | 27.2% Overall | Similar to present study |
| Kapoor D et al., [10] | 2014 | 8000, Himachal Pradesh, India | 25.4% Overall | Similar to present study |
| Gupta V et al., [11] | 2010 | 1260 urban slum males of Haryana, India | 40.8% in males | Similar findings (This can be attributed to similar behavioural and sociocultural practices in urban areas of Haryana) |
| Yadav S et al., [12] | 2008 | 555 females of Lucknow city, Uttar Pradesh, India | 0% in females | Comparable to present study |
| District Level Household Survey- 4 [13] | 2014 | 14556 household of urban Haryana, India | 0.9% in Haryana urban areas and 1.9% in Rohtak district | Similar findings (This can be attributed to similar behavioural and sociocultural practices in urban areas of Haryana) |
| Anand K et al., [6] | 2007 | 1260 males and 1304 females, Faridabad, India | 36.5% in males and 7% in females. Among males, lowest prevalence was seen in 15-24 years age group (12.0%). Among females, maximum prevalence was seen in 55-64 years age group (24.8%). | Similar to present study |
| Aroor B et al., [14] | 2013 | 1805, Gujarat, India | 12.8% in males | Lower (This was because of different characteristics of subjects) |
| Walia R et al., [15] | 2014 | 2227, urban Chandigarh, India | 7.5% overall | Lower (attributed to more strict legislation and high literacy rate in urban Chandigarh) |
| Raghuvanshi VP and Agrawal R [16] | 2013 | 700, Gujarat, India | 12% Overall | Lower (This was because of different characteristics of subjects) |
| Gilani SI and Leon DA [17] | 2013 | 2291 urban people, Pakistan | 18.2 % (males- 31.4%, females- 1.8%) | Lower (This was because of lower mean age for study population as 34±10 year) |
| Gupta R et al., [18] | 2012 | 6198, India | 6.9% (male-12%, femela-0.5%) | Lower (This was because of different characteristics of subjects) |
Prevalence of Smokeless Tobacco Use
In present study, prevalence of current smokeless tobacco use was found to be only among males (6.0%) while no female was reported to be involved in smokeless tobacco use. Smokeless tobacco consumption is not a routine practice in the urban areas of Haryana. This prevalence could be because of migratory population coming in study area for earning purpose from neighboring states and from states like Uttar Pradesh and Bihar. Comparison of various studies on smokeless tobacco use is shown in [Table/Fig-10] [6,11,13,14,17-21].
Comparison of various studies on prevalence of smokeless tobacco use [6,11,13,14,17-21].
| Author name | Publication year | Sample size and study area | Prevalence of smokeless tobacco use | Comparison with current study |
|---|
| Anand K et al., [6] | 2007 | 1260 males & 1304 females, Faridabad, India | Higher in males (10.2%) as compared to females (2.9%). Among males it increased from 5.6% in 15-24 years age group to 15.0% in 2 5-34 years age group. | Similar findings |
| District Level Household Survey- 4 [13] | 2014 | 14556 household of urban Haryana, India | Male-5.3 %, femal-0.4% in Haryana urban areas and Male-4.7%, femal-0.6% in Rohtak district | In coherence (This can be attributed to similar behavioural and sociocultural practices in urban areas of Haryana) |
| Kaur P et al., [19] | 2007 | 2262 Males, Chennai, India | 4.4% in male employees of industrial unit of Tamil Nadu | Slightly lower; attributed to more educated males, who were more aware about the harmful effects of the tobacco use |
| Pathak NK et al., [20] | 2014 | 896 male, Uttar Pardesh, India | 26.5% in male | Higher |
| Garg A et al., [21] | 2014 | 207 adults, Delhi, India | 12% overall | Higher |
| Gupta V et al., [11] | 2010 | 1263 males & 1326 females of urban Haryana, India | Males- 12%, females- 1.4% | Higher |
| Aroor B et al., [14] | 2013 | 1805, Gujarat | 23.1% in males | Higher |
| Gilani SI and Leon DA [17] | 2013 | 2291 urban people, Pakistan | 10.5% (males- 15.1%, females- 4.6%) | Higher |
| Gupta R et al., [18] | 2012 | 6198, India | 9.8% (male-12.7%, female-6.3%) | Higher |
Prevalence of Tobacco Use (Smoking and Smokeless)
In present study prevalence of current tobacco use was found to be higher among males (46.3%) as compared to females (1.0%). The reason could be as in a few social occasions like marriages etc. hookah and bidi is served and is considered as a token of respect. Males used tobacco because of curiosity or peer pressure (85%), imitation of other family members (5.0%), relieving acidity/ tiredness (4.3%) and loneliness (3.7%) while females used tobacco for relieving acidity. Similar prevalence of current tobacco use was reported by Thankappan KR et al., as 22.6% (43% in males and 2.6% in females) in Kerala, Raghuvanshi VP and Agrawal R in Gujarat as 26.2% and Samuel P et al., (46.5% in males and 1.6% in females) in Tamil Nadu [16,22,23]. Contrary to this higher prevalence of tobacco use was reported by Pathak NK et al., in males as 54.6% (26.5% for smokeless tobacco and 28.1% for smoking) of Uttar Pradesh [20].
Socio-Demographic Variables with Current Smoking Status
The association of occupation, education and socio-economic status with current smoking was found to be statistically significant in present study but the individuals were very less in some of the categories hence the association of smoking habits could not be clearly established with these demographic variables. The overall prevalence of current smoking was highest among married (25.4%) followed by unmarried (15.5%) and widowed (9.5%). This might be attributed to maximum number of married participants in the study. While observing the association with educational, it was seen higher in graduates and above (13.7%) as compared to illiterates (8.3%). This was due to very less number of illiterates (24) as compared to graduate and above (474). Comparison of various studies on socio-demographic variables with current smoking status is shown in [Table/Fig-11] [17,18,21,24-26].
Comparison of various studies on socio-demographic variables with current smoking status [17,18,21,24-26].
| Author name | Publication year | Sample size and study area | Socio-demographic variables with current smoking | Comparison with current study |
|---|
| Rooban T et al., [24] | 2012 | Secondary data analysis of the National Family Health Survey-3, India | Higher among ever married males (71.1%) as compared to unmarried (28.9%).Highest in those who had business as occupation (Sales- 20.4%, manual worker- 41.6%) and lowest in those who had no occupation (7.74%). | In accordance with present study |
| Garg A et al., [21] | 2014 | 207 adults, Delhi, India | Highest in those who had business as occupation (28.9%) and lowest in those who had no occupation (9.6%)Highest among lower socio-economic status (33.9%) followed by upper-lower (24.9%), lower-middle (19.0%), upper-middle (12.5%) and upper socio-economic status (0.0%). | Similar to present study |
| Gupta R et al [18] | 2012 | 6198, India | Lower overall prevalence of current smoking in less educated individuals (6.1%) and unemployed (5.1%) as compared to high educated individuals (14.9%) and who had professional occupation (12.5%). | In accordance with present study |
| Palipudi KM et al., [25] | 2012 | 209,027 respondents, Global Adult Tobacco Survey (GATS) | Decreased with increasing level of education (highest of 44.6% in illiterate or less than primary and lowest of 18.3% among graduate or above). | Contrast to present study |
| Reddy KS et al., [26] | 2007 | 19973, employees and their families of India | Decreased with increasing level of education as 77.3%, 42.1% (illiterate to primary), 26.5%,1.6% (more than secondary to graduate) and 19.8%, 1.2% (Postgraduate or above) in males and females, respectively. | Contrast to present study |
| Gilani SI and Leon DA [17] | 2013 | 2291 urban people, Pakistan | Decreased with increasing level of education. After taking Illiterate as reference category, odds of current cigarette smoking in up to primary level category was 0.84 (aOR: 0.84; 95% CI: 0.45-1.57) and in graduate/postgraduate/professional education category was 0.35 (aOR: 0.35; 95% CI: 0.18-0.67) after adjusting for other socio demographic characteristics. | Contrast to present study |
Limitation(s)
This was a cross-sectional study. The study subjects were not followed up after a single visit. There was still a possibility that the subjects may have started tobacco use in coming months.
For tobacco use information given by study subjects was considered as such, authentication of that could not be verified.
Prevalence of smokeless tobacco use was very low in study area, so only current smoking was compared with socio-demographic variables.
Conclusion(s)
Present study highlighted that male indulged in tobacco use at an early age and more frequent as compared to females. The present study revealed that the main reason for initiation of tobacco use in males is curiosity or peer pressure while females used tobacco for relieving acidity. Waist circumference and blood pressure levels were higher in tobacco smokers. Lower socio-economic status also showed a positive association with current smoking status. As tobacco use is an important risk factor for non-communicable diseases, so more strict rules and regulation should be implemented for prevention of development of such unhealthy habits in people of the country.
*Modified kuppuswami socioeconomic scale
*Fisher-exact test
(Figures in parentheses indicate percentages)
*Logistic Regression analysis
aOR(CI)=Adjusted Odds Ratio (Confidence Interval)
*Student t-test
BMI: Body mass index; SBP: Systolic blood pressure; DBP: Diastolic blood pressure; WC: Waist circumference; HC: Hip circumference