The Carpal Tunnel Syndrome (CTS) is a neurological condition resulting from compression of the median nerve at the wrist due to increased pressure within the carpal tunnel [1]. Neural gliding is a treatment technique that may improve symptoms related to CTS by increasing median nerve excursion. There are few quality studies analysed to prove therapeutic efficacy of neural mobilisation and nerve and tendon gliding in patients of CTS [2]. To the best of our knowledge, there are no studies which compare the effect of neural mobilisation and nerve and tendon gliding exercises in CTS.
Hence, this study was undertaken to find whether these are effective on pain and functional status in individuals diagnosed with CTS and to find which treatment technique is more effective. Primary aim of this study was to find whether the neural mobilisation and nerve and tendon gliding exercises are effective in treating CTS and secondary aim was to find which technique is superior in treating CTS.
Materials and Methods
The present study was carried out in a tertiary care hospital in Gujarat state of India. Ethical clearance (HREC/fct/48/session3/7) was obtained from Institutional Human Research and Ethical Committee of Shree Krishna Hospital and Research Center, Karamsad. Participants were recruited from Physiotherapy Out Patient Department after referral from Orthopaedic Department of the hospital. The data were collected from October 2014 to April 2015. Written informed consent was taken from each participant.
Sample size was calculated on basis of effect size that is 0.2 [3]. Power of study was set at 0.80.
Inclusion criteria: In case of bilateral involvement of any subject, the hand with more symptom severity was included.
Exclusion criteria: Pregnancy induced CTS, Operative case of CTS, recurrent CTS following previous surgery, obvious thenar atrophy were excluded.
[Table/Fig-1] shows CONSORT diagram. Sixty hands diagnosed with CTS reporting at Shree Krishna hospital physiotherapy OPD were included in the study. Subjects were assessed prior (1st day) and post (end of 4 weeks) treatment. Physical examination of each patient were included in terms of tinel’s sign, phalen’s sign, two point discrimination with help of compass esthesiometer, grip strength and pinch strength with help of Jamar hand held dynamometer and pinchometer. Subjective outcome measures were Symptom severity score [4] and Functional severity score [5].
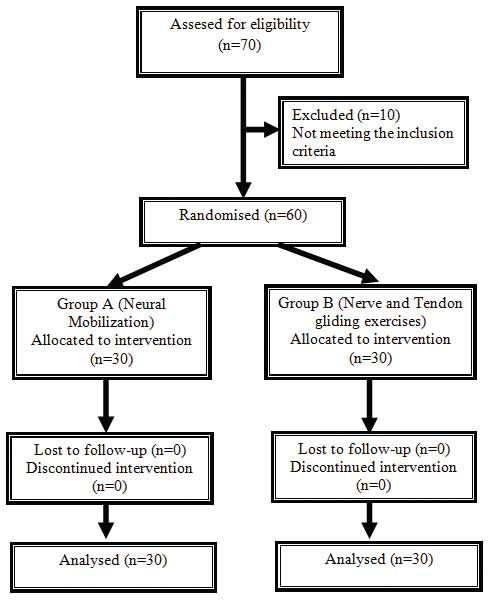
Computer based randomization method was followed for group allocation of participants into Group A and B. Being a single blind study, the outcome assessor was not aware of the patient group. The treatment and assessment were done by two different physiotherapists.
The Boston Questionnaire includes Functional Status Scale, which consists of eight common tasks involving the hands and Symptoms Severity Scale for eleven items. Each question is answered on a scale of 1 to 5 [5]. The patients rated their pain on VAS. Digital dynamometer was used for Grip strength assessment. It was started with right hand followed by left hand. The process was repeated four times; mean of the highest value was recorded.
Both the groups were given ultrasound therapy (pulsed ultrasound-1:4 was given over carpal tunnel with frequency of 1 MHz, intensity of 1.0 W/cm2 for duration of 5 minutes [6]. Three sessions were given per week for a period of 4 weeks) and night splinting. Night splint kept the wrist in neutral position with finger and thumb extended [7].
Subjects in group A were given neural mobilisation along with ultrasound and night splinting. Sensory testing with the monofilaments began with filament in the normal threshold level and progressed to filaments of increasing pressure until the patient felt touch. Sites for median nerve monitoring were the tip of the thumb, index and proximal index. [Table/Fig-2] shows, sequence for Median Nerve Neuromobilisation Technique: A) Shoulder Depression and abduction (110°); B) Wrist extension; C) Supination; D) Shoulder lateral rotation; E) Elbow Extension; F) Neck lateral bending to opposite side. 3 sets of 10 repetitions were given thrice a week for 4 weeks [7].
Neural Mobilisation Technique.
https://www.dynamicchiropractic.com/mpacms/dc/article.php?id=18110
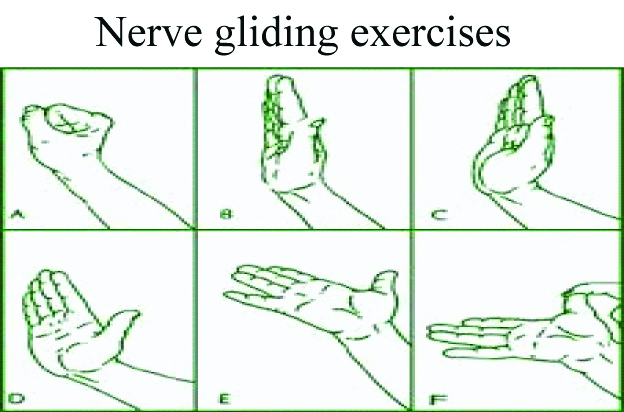
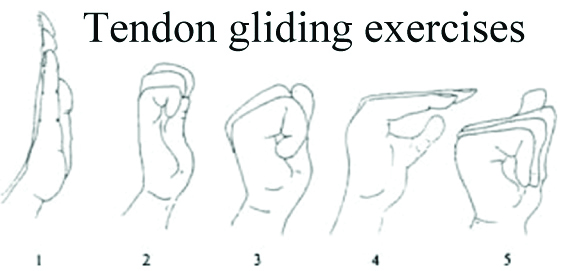
The subjects in group B were given nerve and tendon gliding exercises along with ultrasound and night splinting. [Table/Fig-3] shows tendon gliding exercises included six discrete positions of fingers like straight hand, hook, fist, table top and straight fist. In addition, the median nerve was mobilised by putting hand and wrist through six positions. Each position was maintained for 7 seconds and repeated five times at each session, with a total of 3 to 5 sessions per day for a period of 4 weeks [8].
Tendon gliding exercises.
https://www.dynamicchiropractic.com/mpacms/dc/article.php?id=18110
Six Discrete Positions of Hand and Wrist for Mobilising the Median Nerve [
8]:
1. Wrist neutral with fingers and thumb in flexion.
2. Wrist in neutral with fingers and thumb extended.
3. Wrist and finger in extension with thumb in neutral.
4. Wrist, finger and thumb in extension.
5. Wrist, finger and thumb in extension with forearm in supination.
6. Wrist, finger in extension, forearm in supination with other hand pulling the thumb in hyperextension.
Statistical Analysis
Statistical Package for the Social Sciences (SPSS) version 17.0 was used for statistical analysis. Kolmogorov-Smirnov test was used to check normalcy of data. Baseline homogeneity for outcome measures was established by unpaired t-test. Paired t-test was used for intra-group analysis and unpaired t-test was used for inter-group analysis and p-value was set at less than 0.05. Statistical power was set at 0.80.
Results
There were 26 females and 4 males in the study. Demographic details are shown in [Table/Fig-4]. Paired t-test was used for within group comparison and unpaired t-test for between group comparisons at 95% confidence interval i.e., p-value less than 0.05. As shown in [Table/Fig-5,6], all the outcome measures in intra-group analysis for both the groups showed significant improvements.
Mean and Standard deviation (SD) of age and frequencies of male and female.
| Group | Mean age | Male N (%) | Female N (%) |
|---|
| A | 45.13±12.64 | 4 (13.3) | 26 (86.7) |
| B | 38.80±12.35 | 4 (13.3) | 26 (86.7) |
Paired t-test for group A.
| Paired t-test | Group A | | Mean | Standard deviation (SD) | p-value |
|---|
| Pair- 1 (A) | Symptom severity score | Pre | 1.73 | 0.46 | <0.001 |
| Post | <0.001 | <0.001 |
| Pair-2 (A) | Functional severity score | Pre | 2.07 | 0.70 | <0.001 |
| Post | 0.07 | 0.25 |
| Pair-3 (A) | Grip strength | Pre | 13.40 | 4.97 | <0.001 |
| Post | 24.13 | 6.10 |
| Pair-4 (A) | Pinch strength | Pre | 5.47 | 1.99 | <0.001 |
| Post | 9.87 | 2.82 |
| Pair-5 (A) | 2 point discrimination | Pre | 10.00 | 4.07 | <0.001 |
| Post | 6.40 | 2.32 |
p-value <0.05 to be significant
Paired t test for group B.
| Paired t-test | Group B | | Mean | Standard deviation (SD) | p-value |
|---|
| Pair-1 (B) | Symptom severity score | Pre | 1.67 | 0.49 | <0.001 |
| Post | 0.53 | 0.51 |
| Pair-2 (B) | Function severity score | Pre | 1.53 | 0.51 | <0.001 |
| Post | 0.73 | 0.46 |
| Pair-3 (B) | Grip strength | Pre | 11.33 | 6.44 | <0.001 |
| Post | 14.60 | 5.62 |
| Pair-4 (B) | Pinch strength | Pre | 4.53 | 1.47 | <0.001 |
| Post | 6.50 | 2.16 |
| Pair-5 (B) | 2 point discrimination | Pre | 10.27 | 4.52 | <0.001 |
| Post | 8.27 | 5.35 |
p-value <0.05 to be significant
As shown in [Table/Fig-7] Inter-group analysis proved that neural mobilisation is more effective in terms of reduction of symptom severity, improvement in functional status, grip strength and pinch strength than nerve and tendon gliding exercises except two point discrimination (p<0.05).
Inter-group analysis using upaired t test.
| Unpaired t-test | Group | Mean | Standard deviation | p-value | Mean difference |
|---|
| Difference in symptom severity score (Equal variances assumed) | A | -1.73 | 0.46 | 0.006 | -0.60 |
| B | -1.13 | 0.64 |
| Difference in functional status score (Equal variances assumed) | A | -2.00 | 0.65 | <0.001 | -1.20 |
| B | -0.80 | 0.41 |
| Difference in Grip strength (Equal variances assumed) | A | 10.73 | 3.10 | <0.001 | 7.46 |
| B | 3.27 | 1.87 |
| Difference in Pinch strength (Equal variances assumed) | A | 4.40 | 2.97 | 0.005 | 2.43 |
| B | 1.97 | 0.99 |
| Difference in 2 point discrimination (Equal varience assumed) | A | -3.60 | 2.35 | 0.084 | -1.6 |
| B | -2.00 | 2.54 |
p-value <0.05 to be significant
Discussion
On basis of clinical diagnosis, the prevalence of CTS in the general population is 3.8% and on basis of neurophysiological diagnosis, it is 2.7% [9]. Findings of this study correlated with the findings of several other authors who stated that females are more prone than males for developing CTS [10]. Talebi GA et al., has concluded that “Manual therapy techniques applied to mechanical interface of the median nerve and nerve mobilisation, possess more appropriate and valuable effects on hand difficulties than modalities in diabetic patients with CTS” [11]. The data analysis showed that with the use of four weeks of protocol there was a significant reduction in symptom severity with improved functional status, grip strength, pinch strength and two point discrimination in both the groups. Comparative analysis between groups revealed better improvement with neural mobilisation in terms of all outcome measures except two point discrimination. This result is supported by a study that describes the peripheral nervous system as having considerable regenerative powers [12].
In a study that investigated the effect of neural mobilisation in addition to standard care in CTS reported better functional outcome with addition of neural mobilisation. All the other outcome measures showed no significant difference [8]. Akalin E et al., found a greater improvement in grip strength (p=0.026) with wrist splint in combination with tendon gliding exercises, on 8th week follow-up [13]. Tal-Akabi A and Rushton A investigated the effectiveness of manual therapy intervention i.e., carpal bone mobilisation and mobilisation of the nervous system in CTS patients and reported significant improvement in pain scores. It showed clinical improvements but failed to show statistically significant difference in functional scores in three weeks [14]. Utilising a larger sample size could possibly explore the effect further. Butler DS and Shacklock MO investigated the effects of nervous system mobilisation on nerve entrapment problems [12,15].
The probable mechanism underlying is improvement in axonal transport leading to improved nerve conduction. Nerve mobilisation reduces its pressure causing an improvement in blood flow to the nerve. It may also help in regeneration and healing of an injured nerve [14]. Herbert R et al., who used other conservative methods of treatment like ultrasound and splinting claimed good results in CTS [16]. Chiropractic and osteopathic researchers who used different manipulation techniques on CTS showed improvement in terms of functional outcome [17]. Rozmaryn LM et al., found that nerve and tendon gliding exercises when given in CTS, performed remodeling and stretching of the investing, adhesive tenosynovium around these structure, thus diminishing their adherence to the structures inside the canal [8]. In addition, by bringing the nerve through its maximal excursion, there may be redistribution of the point of maximal compression on the median nerve inside the carpal canal by allowing varying points of the nerve to be exposed to the maximal compressive area underneath the transverse carpal ligament. This “milking” effect would promote venous return from median nerve and may restore the linear relationship between median nerve and flexor tendon displacement [11]. Probably more sessions will be required for even two point discrimination to show improvement statistically.
Limitation(s)
There was no follow-up done to see sustained effects of interventions. This study lacked control group to establish efficacy of two interventions.
Conclusion(s)
It is likely that patients with CTS would be benefited with the addition of neural mobilisation to standard treatment like night splinting and ultrasound. This approach reduces pain, improves sensation, hand muscle strength and function which makes it a reasonable therapeutic option for clinicians in treating individuals with mild to moderate CTS. We recommend to do study with follow-ups to see sustained effects of intervention.
p-value <0.05 to be significant
p-value <0.05 to be significant
p-value <0.05 to be significant