Partially Treated Typhoid fever Leading to Inevitable Abortion: A Case Report
Ashima Jain1, Namita Jaggi2, Deepa Maheshwari3
1 Attending Consultant, Department of Laboratory Medicine, Artemis Hospitals, Gurugram, Haryana, India.
2 Chairperson, Department of Labs and Infection Control, Artemis Hospitals, Gurugram, Haryana, India.
3 Senior Consultant, Department of Obstetrics and Gynaecology, Artemis Hospitals, Gurugram, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Ashima Jain, Department of Laboratory Medicine, Gurugram, Haryana, India.
E-mail: ashimajain15@gmail.com
Typhoid fever continues to be a major public health problem in developing countries especially due to the challenging infrastructure and sanitation facilities. Many cases of abortions due to untreated Salmonella infection have been reported. The present report is about a 25-year-old female who was inadequately treated for typhoid fever with suboptimal doses of oral ampicillin leading to inevitable abortion despite the infection being cleared from blood. Salmonella typhi was isolated from products of conception. The patient was treated with Ceftriaxone injections and has been found to be fine on follow-up visits. Typhoid during pregnancy needs to be treated with higher doses and preferably intravenous antibiotics instead of oral due to the increased volume of distribution and reduced tissue penetration of antibiotics in such patients.
Ampicillin dosage, Pregnancy, Salmonella typhi
Case Report
A 25-year-old female, primigravida at 14 weeks of gestation, presented to the emergency department with complaints of intermittent pain abdomen and spotting for 2 days, with sudden increase in intensity and severity of pain for few hours before presentation. However, the patient was afebrile. She also gave history of hypothyroidism in the current pregnancy and was taking tablet Levothyroxine sodium 50 mcg daily for the same.
She was euthyroid at the time of presentation. The patient had a marked leucocytosis (TLC 18.6 × 109/L). All the other blood parameters including liver and kidney function tests were within normal ranges. The Toxoplasmosis, Rubella Cytomegalovirus, Herpes simplex, and HIV (TORCH) parameters were negative. During ultrasonography, she further deteriorated. The pain worsened and bleeding increased, the fetus got expelled and she had an inevitable abortion. The patient was immediately shifted to the operation theatre for ultrasound guided suction and evacuation in view of retained placenta.
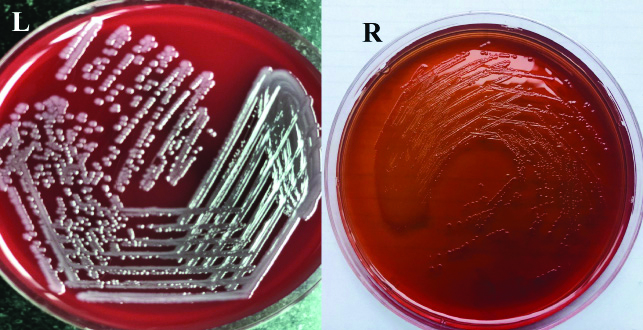
In order to further investigate the cause for the abortion, a culture sensitivity test of the Products of Conception (POCs) was sent to the laboratory to rule out infection. The POCs were cultured on Blood agar and MacConkey agar as per the lab protocol. A small piece of tissue was also incubated in brain-heart infusion and sub-cultured after 24 hours on blood agar and MacConkey agar to further enhance the chances of growth of infecting organism. The blood agar grew 0.5-1 mm, white, smooth, non-haemolytic colonies with entire edges. On Macconkey agar, 0.5-1 mm, non-lactose fermenting, smooth colonies were obtained [Table/Fig-1]. Oxidase was negative and catalase was positive. On Grams staining, gram negative bacilli with no specific pattern were seen. The colonies were further processed for identification and antimicrobial susceptibility on Vitek-2 compact (Biomerieux, France). The organism was identified as Salmonella enterica subsp. enterica sero. Typhi sensitive to Ampicillin, Trimethoprim-Sulfamethoxazole, Ceftriaxone, Cefixime, Chloramphenicol and Azithromycin.
Growth seen on Blood agar (left) and MacConkey agar (right).
The strain was resistant to Nalidixic acid and fluoroquinolones. The identification of the organism was further confirmed by serotyping and growth of Hydrogen Sulfide (H2S) producing organism on triple-sugar iron agar [Table/Fig-2]. The blood cultures of the patient was sterile. On enquiring from the patient specifically regarding typhoid, she gave a history of being treated 1 month back for typhoid fever, diagnosed on the basis of blood culture performed elsewhere. As per the reports shown by the patient, she had a blood culture report showing growth of Salmonella typhi with sensitivity pattern similar to the one reported in the POCs. She further revealed that she had taken tablet Ampicillin 1000 mg thrice daily for 15 days after which she was afebrile and fine.
Biochemical reactions showing production of H2S.

After 3 days of empirical treatment with Amikacin (1 gm once daily intravenous) and Ceftriaxone (1 gm twice daily intravenous), the TLC became normal and the patient was clinically stable. She was discharged on Cefixime (20 mg/kg/day) for further 10 days. The patient has been fine on follow-up visits.
Discussion
Typhoid is an endemic infection in India and majority of Indian population is exposed to this infection in the childhood itself. Owing to the poor sanitation and hygiene facilities especially amongst the low socioeconomic strata, and feco-oral route being the most common route of transmission, a huge burden of this disease is prevalent in the country. An estimated 12-20 million cases and 13000-220,000 deaths of typhoid fever in Asian countries were reported recently [1]. In India, an annual incidence of 493.5/100,000 persons per year has been reported [2]. Pregnant females are even more immunosuppressed and prone to infections due to the hormonal changes further leading to a compromised cell mediated immunity. An estimated incidence of fetal loss in untreated cases of typhoid in pregnancy has been reported to be around 80% [3]. Vertical transmission of Salmonella has been reported transplacentally especially with history of Salmonella bacteremia and typhoid has been attributed to be an important cause of mid-trimester abortions [4]. However, it is often missed while investigating such cases.
Although Cefixime (20 mg/kg/day × 14 days) or Azithromycin (500 mg twice daily × 7 days) are the drugs of choice for treatment on outpatient basis, the recommendations also suggest that ampicillin might be used as per the sensitivity pattern in culture report [5]. Some obstetricians suggest that Ampicillin remains the drug of choice in pregnant patients [4]. Although the recommended dose of Ampicillin in adults is 100 mg/kg/day in four divided doses for 14 days [5], there have been reports to suggest that at least for oral regimens, but not for intramuscular or intravenous routes, higher doses should be prescribed for pregnant females to achieve adequate drug levels considering a significant increase in volume of distribution and renal plasma clearance [6-8]. In the present case, the patient was treated with suboptimal doses of oral Ampicillin (3000 mg/day in 3 divided doses) which may have probably cleared the bacteraemia but could not achieve adequate levels in the placenta and amniotic fluid. Intravenous route should have been used to achieve the required concentration of the drug. Also, third generation Cephalosporins should be the preferred agents considering the increasing prevalence of multi-drug resistant organisms [5].
A similar report has also been published where the patient presented with bleeding per vaginum followed by a spontaneous abortion and Salmonella typhi was grown in high vaginal swab. She too gave history of being treated for typhoid fever a month back. However, the details of treatment received by the patient could not be elicited [9]. Another case report described a patient in the second trimester of pregnancy with a similar presentation. However, the patient was having intermittent fever and took treatment from a local practitioner (details unknown). Nalidixic Acid Resistant Salmonella typhi (NARST) was grown in the POCs and she was later treated with intravenous ceftriaxone [4]. Vertical transmission and spontaneous abortion have also been reported for Salmonella paratyphi A in a case report. The patient had intermittent fever associated with pain abdomen and was given tablet Azithromycin 500 mg for 3 days empirically by a local practitioner. She eventually had a spontaneous abortion and POCs grew Salmonella Paratyphi A. Intravenous cefixime and intravenous metronidazole was given to the patient for 3 days empirically. However, the patient was lost to follow-up [10].
Conclusion(s)
Typhoid fever is an important cause of mid-trimester abortions and should be investigated for patients presenting with pyrexia during pregnancy. Also, once detected, it should be aggressively treated preferably with intravenous antibiotics. Considering the increasing prevalence of NARST and Multidrug Resistant (MDR) strains, the empirical therapy should preferably be third generation Cephalosporins. The patients should be kept under strict follow-up and repeated ultrasound scans should be performed in order to detect any abnormalities.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. NA
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Mar 04, 2020
Manual Googling: Apr 23, 2020
iThenticate Software: May 11, 2020 (12%)
[1]. Mogasale V, Maskery B, Ochiai RL, Lee JS, Mogasale VV, Ramani E, Burden of typhoid fever in low-income and middle-income countries: A systematic, literature-based update with risk-factor adjustmentLancet Glob Health 2014 2:e570-80.10.1016/S2214-109X(14)70301-8 [Google Scholar] [CrossRef]
[2]. Ochiai RL, Acosta CJ, Danovaro-Holliday MC, Baiqing D, Bhattacharya SK, Agtini MD, A study of typhoid fever in five Asian countries: Disease burden and implications for controlsBull World Health Organ 2008 86:260-68.10.2471/BLT.06.03981818438514 [Google Scholar] [CrossRef] [PubMed]
[3]. Kaistha N, Singla N, Bansal N, Chander J, Salmonella typhi isolation in pregnant women: determining the importanceJ of Clin and Diagnostic Research Sept 2013 7(9):2100-01.10.7860/JCDR/2013/6118.341724179957 [Google Scholar] [CrossRef] [PubMed]
[4]. Poonia S, Satia MN, Torame VP, Natraj G, Vertical transmission of Salmonella typhiJ of Postgraduate Gynae & Obs 2015 2(1)ISSN 2348-5442. Available from: http://www.jpgo.org/2015/01/vertical-transmission-of-salmonella.html [Google Scholar]
[5]. Upadhyay R, Nadkar MY, Murugananthan A, Tiwaskar M, Amarapurkar D, Banka NH, API Recommendations for management of typhoid feverJ of The Association of Physicians of India 2015 63:77-96. [Google Scholar]
[6]. Ansari J, Carvalho B, Shafer SL, Flood P, Pharmacokinetics and Pharmacodynamics of Drugs Commonly Used in Pregnancy and ParturitionAnesthesia and Analgesia 2016 122(3):786-804.10.1213/ANE.000000000000114326891392 [Google Scholar] [CrossRef] [PubMed]
[7]. Philipson A, Pharmacokinetics of ampicillin during pregnancy 1977 136(3):370-76.10.1093/infdis/136.3.370903675 [Google Scholar] [CrossRef] [PubMed]
[8]. Nau H, Clinical pharmacokinetics in pregnancy and perinatology. II. PenicillinsDev Pharmacol Ther 1987 10(3):174-98.10.1159/0004577443301235 [Google Scholar] [CrossRef] [PubMed]
[9]. Kaur R, Barman P, A case of Salmonella typhi infection leading to miscarriageJ Lab Physicians 2011 3(1):61-62.10.4103/0974-2727.7857421701670 [Google Scholar] [CrossRef] [PubMed]
[10]. Sethi S, Gautam V, Gupta K, Suri V, Angrup A, Vertical transmission of Salmonella enterica serotype Paratyphi A leading to abortionJMM Case reports 2017 4:01-03.10.1099/jmmcr.0.00512729255611 [Google Scholar] [CrossRef] [PubMed]