Tonsillectomy is one of the most common surgical procedures performed all over the world [1]. The common indications remain recurrent tonsillar infection (chronic tonsillitis) or obstruction of the airway (kissing tonsils). Until the late 1960’s: tonsillectomies were performed using cold method, wherein thes capsule of tonsil was dissected from the floor of the fossa by blunt and sharp dissection [1]. In 1970’s hot electrocautery was declared a safe and easy to perform due to the minimum intra-operative haemorrhage [1]. The intra-operative blood loss, post-operative haemorrhage and post-operative pain have remained the considerable challenges despite technological advances, surgical techniques and instrumentations of tonsillectomy.
Surgeons and anaesthesiologists always recommended and searched for methods to reduce peri and post-operative morbidity [2,3]. Several electrocautery-based techniques have been developed that result in less post-operative bleeding, but they do not significantly reduce the post-operative pain [1]. Intra-operative ligation of the bleeding site was first adopted as a routine measure by Cohen L and has remained in use ever since [4].
The study by Salam MA and Cable HR reported that as the number of cases of tonsillectomy is high in their set up the time of operation as well as the intra-operative blood loss are the important factors to be considered in tonsillectomy [5]. For sake of evaluation of post-operative pain, intra-operative blood loss, operating time, post-operative healing of tonsillar fossa and total duration of stay, the study of comparing tonsillectomy methods of dissection and snare and electrocautery was undertaken amongst a rural population of western Maharashtra, India.
Materials and Methods
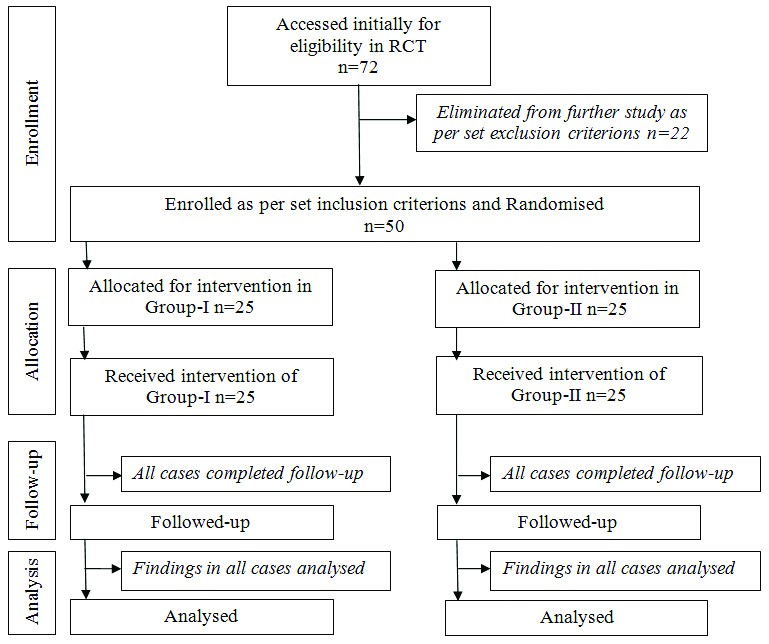
The randomised clinical trial was carried out in the Department of Otorhinolaryngology of tertiary care teaching hospital of western Maharashtra, on a sample size of 50, during the period April 2019 to December 2019. The ethical clearance from institutional ethics committee was sought vide their letter number KIMSDU/IEC/05/2019 dated 03/04/2019. The Institutional Ethics Committee of Krishna Institute of Medical Sciences, Karad and KIMSDU, Karad (IEC Karad) is registered with DCGI vide letter number ECR/708/Krishna/Inst/MH/2013 dated 08.05.2013. Prior informed consent was obtained from all the participants in this study. As this study was of short duration, it was planned with at least 20 cases in each group. However, keeping the possibilities of drop out during follow up in the study, it was decided to enroll minimum 25 cases in each group, and hence the sample size was 50.
The clinically diagnosed cases suffering from chronic tonsillitis and having age more than six years, irrespective of their gender were included in the study. Patients diagnosed as acute tonsillitis or having bleeding disorders, active menstruation, Hb level less than 10 gm/dL and those on antibiotic treatment recently since five or fewer days were excluded.
All 50 cases enrolled in the study were placed in group-I and II by using lottery method, for maintaining single blind status and were subjected to tonsillectomy performed by a single consultant surgeon and with similar pre and post-operative medications using dissection and snare, and electrocautery method respectively in all cases. The general anaesthesia was provided by the available consultant in every case. Routine blood and urine examination namely Complete Blood Count (CBC), Bleeding Time (BT) and Clotting Time (CT), Blood grouping as well as urine routine and microscopy etc., was undertaken in every case before operation. The post-operative pain was recorded using Visual Analogue Scale (VAS) (response from 1-10). In this study, VAS was noted after the wearing of effects of anaesthesia i.e., 4-6 hours after the surgery. For tonsillectomy using dissection and snare technique the tonsillectomy set of instruments (Kalelkar Surgicals Pvt., Ltd.,) consisting of Boyle-Davis mouth gag, Draffin’s bipod, Denis Browne’s tonsil holding forceps, Mollison’s tonsillar dissector cum anterior pillar retractor and Eve’s tonsillar snare (Cold Steel) was used. The bi-polar and monopolar electrocautery of L&T make was used.
The operating time was noted from making of incision up to achieving the complete haemostasis in bilateral dissected tonsillar fossae using a stop watch. The intra-operative blood loss was estimated by weighing the gauze pieces before and after soakage. The intra-operative complications requiring extended procedure if any were noted. The total duration of hospitalisation from admission of the patient till finally conforming fitness before sending home was assessed based on status of patient as to whether there is any abnormal odynophagia, fever and any active bleeding or excessive slough in the tonsillar fossa.
The cases requiring additional analgesic dose was noted as per the degree of pain measured on VAS scale during initial 4-6 and after 24 hours of surgery. All cases received Dexmeditomidine 1 micro gram per Kg IV intra-operatively, followed by 0.5 micro grams per kg in normal saline drip every hourly till 4 hours or full recovery from anaesthesia. The cases with VAS score more than 6 received additional analgesic dose of injection tramadol 0.8 mg per Kg IV at every 8 hour or until VAS <5. The condition of tonsillar fossae was frequently examined during immediate follow-up of first 24 hours after tonsillectomy. There after all cases were called again for follow-up after discharge on 7-10 days postsurgery [Table/Fig-1].
Statistical Analysis
The mean post-operative pain, intra-operative blood loss and total duration of hospitalisation were compared by Mann-Whitney U-test. The mean duration of operating time was compared by Student’s t-test. In some parameters like mean post-operative pain, intra-operative blood loss and total duration of hospitalisation, the data didn’t follow normal distribution hence parametric test such as student’s t-test was replaced by nonparametric test ’Mann-Whitney test’. Wherever, the data followed normal distribution like in mean duration of operating time the student’s t-test was used. Dose comparison of analgesic and extended haemostatic measure required were compared by Chi-square test (software used InStat 9.0, INDIA).
Results
All enrolled 50 cases of group-I and II underwent tonsillectomy using dissection and snare and electrocautery methods, respectively. The age range was 8 to 25 years, gender of participants in either group was almost similar M:F ratio was 0.48:0.52, mean age of group-I and II was 16.12 and 16.14 respectively [Table/Fig-2].
| Parameters | Both groups n=50 | Group-I n=25 | Group-II n=25 |
|---|
| Median age (Years) | 16 (8-25) | 16 (8-25) | 16 (8-25) |
| Mean±SD (Years) | 16.12±03.91 | 16.12±2.42 | 16.14±4.02 |
| Sex distribution |
| Male | 24 (48%) | 12 (48%) | 12 (48%) |
| Female | 26 (52%) | 13 (52%) | 13 (52%) |
Mean intra-operative blood loss in group-I was 4.85 mL and in group-II was 2.55 mL with p<0.0001. The mean post-operative pain was 5.5 in group-I and 6.23 in group II with p<0.0001. Mean duration of surgery was 6.39 and 4.55 minutes for group I and II, respectively, -p<0.0001. The mean duration of stay remained less than two days in either group. However, it was 30.72 hours and 44.16 hours in group I and II respectively p=0.0131 [Table/Fig-3].
| Group-I n=25 | Group-II n=25 | p-value |
|---|
| Intra-operative blood loss (milliliters)Mean±SD | Mean- 4.85±1.15 | Mean- 2.55±0.88 | <0.0001* |
| Male- 4.72±0.35 | Male- 2.52±0.54 |
| Female- 4.98±0.78 | Female- 2.57±0.52 |
| Pain after 4-6 hours postsurgery (VAS)Mean±SD | Mean- 5.5±0.51 | Mean- 6.23±0.42 | <0.0001* |
| Male- 5.48±0.061 | Male- 6.17±0.22 |
| Female- 5.52±0.073 | Female- 6.28±0.21 |
| Duration of operating time Mean±SD (minutes) | 6.39±0.47 | 4.55±0.50 | <0.0001* |
| Duration of stay Mean±SD (hours) | 30.72±16.28 | 44.16±19.2 | 0.0131 |
*p<0.0001 is significant
The number of cases requiring extended post-operative procedure like ligature and cauterisation for haemostasis was three in group I and four in group II while those requiring additional dose of analgesia was four in group I and 14 in group II. The mean additional dose of analgesia required was higher in group-II cases. During post-operative follow-up slough in tonsillar fossa was noted in 2, 8 cases of group-I and II p=0.098 [Table/Fig-4,5].
| Cases requiring/having: | Number of cases | Chi-square test value | p-value |
|---|
| Group-I | Group-II |
|---|
| Extended post-operative procedure | 3 | 4 | 0.1661 | 0.684 |
| Additional analgesic dose in first 24 hours of surgery(mean extra analgesic dose in-μg) | 4 (72) | 14 (82.28) | 7.44 | 0.684 |
| Presence of slough at post-operative fossa during follow-up | 2 | 8 | 2.741 | 0.098 |
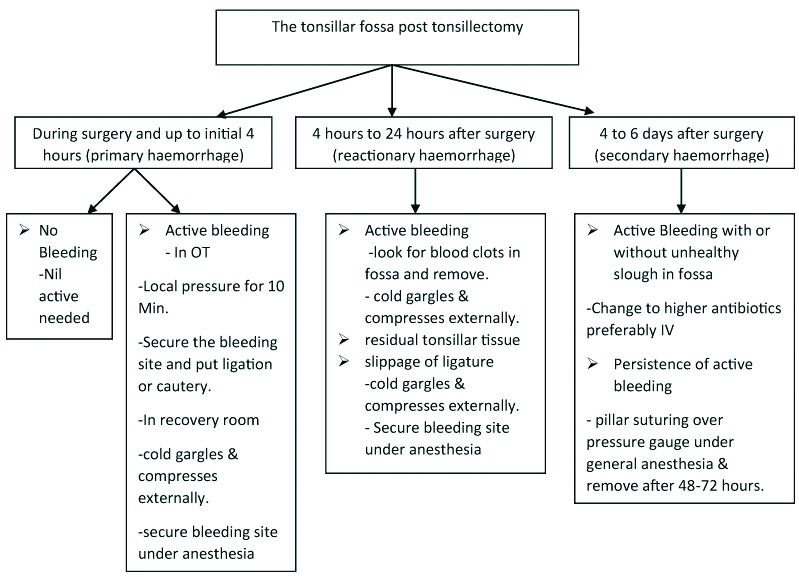
The post tonsillectomy management of tonsillar fossa.
Discussion
Tonsillectomy is performed by blunt dissection, laser or diathermy. Electro-dissection tonsillectomy initially was performed with monopolar diathermy. Historically, diathermy was questioned during tonsillectomy because of concomitant use of inflammable anaesthetic gases. Later on after the advent of non-flammable anaesthetic agents, the use of monopolar and subsequently bipolar diathermy as a mean of securing haemostasis was started. Various authors have used this method with low morbidity i.e., shorter operative time, and significantly low volume of blood loss. The precise nature of electrocautery dissection allows the blood vessels to be identified and diathermised keeping blood loss to minimal [6,7]. In this comparative study between tonsillectomy methods of dissection and snare versus electrocautery the average intra-operative blood loss was 4.85±1.15, 2.545±0.88 mL (p<0.0001) in group I, II, respectively. Intra-operative average blood loss was significantly less in electrocautery group than in dissection-snare group as reported by many other studies [6-10]. Similarly, the mean operating time in this study was lesser in electrocautery group. Some studies found that the operating time in electrocautery group was significantly less as compared to dissection group [7,9-11].
The mean post-operative pain noted in this study after 4-6 hours postsurgery was 5.50±0.51, 6.223±0.42 (p<0.0001) according to VAS scale in group I, II, respectively. In study of 103 cases by Álvarez Palacios I et al., that compared post-operative pain in three different techniques i.e., Cold Dissection (CD), Monopolar-Bipolar Dissection (MBD) and Coblation Dissection (CBD) the post-operative pain did not show any significant differences between the groups, except for the first day, when MBD tonsillectomy showed a higher pain score [12]. Similarly the studies done by Mofatteh MR and Salehi F; and Senzen OS and Kaytanc H found higher pain scores in electrocautery group than in dissection and snare group on first post-operative day [8,10].
The additional analgesic dose needed in the cases of this study was higher in electrocautery group as compared to dissection and snare group. Similar study by Nunez DA and Provan J carried out in 54 cases required the additional analgesic dose within first 24 hours of surgery more in electrocautery as compared to dissection and snare group [13].
In this study, complications such as primary or reactionary haemorrhage occurred in 3, 4 cases in group I, II which required extended procedures like ligation, cautery respectively. Mackenzie IJ reported 172 patients who had ligatures on one side compared to diathermy on the other side, only one primary bleed occurred on the ligated side [14]. Secondary haemorrhage did not occur in any of the cases in this study as it could be due to proper aseptic care as well as tissue handling at the time of surgery which is in accordance with study by Lassaletta-L found no difference between the two techniques in the incidence of later post-operative haemorrhage [11]. In either groups, of this study there was no significant difference in mean duration of stay, extended post-operative procedure as well as additional analgesic dose required and tonsillar fossa healing during 7-10 days.
Limitation(s)
The factors, viz. short duration and subsequent small sample size are the limitations of study.
Conclusion(s)
In this study amongst the cases of chronic tonsillitis from western Maharashtra, the tonsillectomy technique of group-II using electrocautery was more effective in significant reduction of both excessive intra-operative blood loss and duration of surgery under anaesthesia as compared to dissection and snare of group-I. Hence, while planning for tonsillectomy in chronic tonsillitis with increased morbidity due to boarder line haemoglobin level and or other causes of increased anaesthetic risks especially at centers with higher daily patient turnover such as in large tertiary care hospitals, the more effective method of using electrocautery should be preferred.
*p<0.0001 is significant