Amputation of lower extremity is one of the oldest surgical procedures. Amputated limb with ideal stump has excellent results, whereas bad stumps prolong the prostheses fitting and rehabilitation. Revision amputations are commonly indicated in poor stump formation, infection, recurrent ulceration, stitch abscess, neuroma and flap necrosis. Revision surgery rate of primary amputations stands high despite maximum care at tertiary hospitals. Successful revision surgeries are very rare as infection is inevitable yet preventable cause. This is a case of a 63-year-old male, who presented to the Surgery Outpatient Department (OPD) with wound over the right popliteal region which developed over the course of 15 days after he was attacked by a wild bore and later it was diagnosed as vascular injury. Therapeutic embolisation was done. However, the patient continued to develop gangrenous changes over the wound site. Hence, an emergency above-knee amputation of the right limb was done. However, patient developed infection post-operatively leading to formation of poor stump. Thus, revision surgery was done. This case is rare because, in spite of meticulous search of various medical portals online for similar case scenarios, very rarely revision surgeries done for above-knee amputations with infected stump are found to be successful.
Case Report
A 63-year-old male, came with a chief complaint of wound on the right popliteal region, since 15 days. Patient was attacked by a wild boar 15 days back while working on a farm. He had no chronic illness (like diabetes mellitus, hypertension, bronchial asthma). On general physical examination, the patient was conscious and well oriented to time, place and person. He was afebrile with blood pressure of 110/80 mmHg, pulse rate of 80 bpm and respiratory rate of 20 breathes per minutes.
On systemic examination, no obvious abnormality was detected. On local examination, there was a wound of size 8 cm × 5 cm on the right popliteal region, with scab over the wound and active bloody discharge [Table/Fig-1]. On palpation, popliteal artery, anterior tibial artery, posterior tibial artery and dorsalis pedis artery pulsations were diminished on right lower limb, whereas femoral artery pulsations were normal.
Wound in the right popliteal region.

Patient was admitted under Interventional Radiology (IR) Department for embolisation of right popliteal artery since it had active bleeding. Embolisation was done on the same day of admission. Routine laboratory investigations were done which showed severe anaemia (Hb- 4 gm%), high White Blood Cell (WBC) count (21700 cells/cumm) and deranged renal function tests (Serum Creatinine- 2 mg/dL, Serum Urea- 54 mg/dL). Hence 2 units of Packed Red Blood Cell (PRC) was transfused on the second day of admission along with antibiotics (Inj. Ceftriaxone 50 mg/m2).
Post-procedure colour doppler study of the right lower limb was done on third day of admission which revealed monophasic severely dampened flow in the anterior tibial artery, posterior tibial artery and dorsalis pedis artery. However, post-emobolisation gangrenous changes were noticed in the right lower limb. Henceforth, patient was referred to General Surgery Department for further evaluation and management.
Patient was planned for emergency above-knee amputation surgery of right lower limb on third day of admission. Intra-operatively, muscle present in the popliteal fossa was gangrenous with loculated pus discharging areas. Femoral artery was ligated and the stump was kept open [Table/Fig-2]. The collected pus was sent for culture and sensitivity.
Wound after above-knee amputation of right leg.

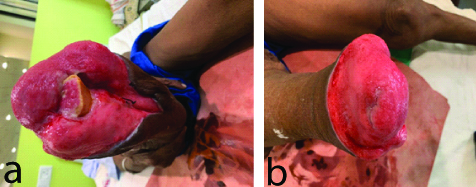
Post-operatively on the fifth day of admission, infection was noted at the operated site [Table/Fig-3]. Culture and sensitivity reporting was done on sixth day of admission which revealed growth of multiple organisms Acinetobacter, Oxacillin and Methicillin resistant (MRSA) coagulase positive Staphylococci, Klebsiella pneumoniae, Pseudomonas aeroginosa, Citrobacter fruendi. These organisms were sensitive to Amikacin and Ciprofloxacillin. Hence, Injection (Inj) Amikacin (15 mg/kg/day in two divided doses for 5 days) and Inj. Ciprofloxacin (400 mg/day in two divided doses for 7 days) was given. The wound was also managed with daily sterile dressing along with intravenous antibiotics administration. The wound on 13th day of admission showed minimal infection with hypergranluated tissue [Table/Fig-4a,b]. Repeat culture and sensitivity was sent and reporting was done on 16th day of admission which revealed persistent growth of Acinetobacter and Pseudomonas aeroginosa.
Three infected wound leading to poor stump.

Wound after administration of intravenous antibiotics and daily sterile dressing.
Hence, patient was planned for revision surgery followed by secondary suturing of the stump on 17th day of admission. Post-operatively, wound was healthy with no gape/discharge. Hence, patient was being discharged with an advice to follow-up after 2 weeks. On follow-up visit, Complete Suture Removal (CSR) was done [Table/Fig-5] and patient was advised for prosthesis. The patient did not develop any stump problems though patient has restricted mobility as knee joint was compromised and patient underwent above-knee amputation.
Successful wound closure after revision surgery.

Discussion
There are many causes like trauma (most common), infection, peripheral vascular disease, malignancy and leprosy [1] which may lead to amputation; whereas penetrating trauma is the most common cause of vascular injuries in the extremities. The second most common cause is blunt trauma, including traffic accidents, falls from a height, and crush injuries [2].
Even though complication rates are higher with Below Knee Amputations (BKAs), the ambulatory rates are higher with BKAs when compare to above-knee amputations. Thus, aggressive attempts should be made to salvage the knee joint when planning for amputation [3]. In the present case report, trauma by an animal (wild boar) was the cause and the level of injury being popliteal fossa did not permit the salvage of knee joint thus resulting in above-knee amputation.
In a similar study done by Kumar D et al., out of 32 patients 14 patients had history of trauma and required amputation [1]. Another study by Ajibade A et al., also found 52 of 132 patients with a history of trauma. So trauma is the most common cause in such cases [4]. Vascular injury may cause irreversible ischemia in 6 to 8 hours. Blunt popliteal artery injury may cause amputation in nearly 30-60% of the cases; this is because of the vascular occlusion secondary to thrombi of the ruptured vascular intima [2].
In the present case report, the patient presented with a vascular injury of 15 days history, on the popliteal fossa with an active bleeding point from the wound for which embolisation was done. In a similar case by Imerci A et al., 34-year-old male with history of crush injury showed a thrombus in the popliteal area on Doppler study, so embolectomy was done [2].
An early diagnosis of the vascular injury of knee joints along with popliteal vascular injury is made by clinical signs and necessary additional examinations. Early diagnosis is made by the following characteristics which need to be identified in the injured limb: dorsalis pedis artery and the posterior tibial artery palpation which are not obvious; the skin is often cold below the injured knee when compared with the healthy limbs; the capillary filling in peripheral toes of the foot below the injury is poor [3]. The blood oxygen saturation monitoring of the injured limb’s toes is usually low; and the examinations of the injured limb via vascular intervention of Digital Subtraction Angiography (DSA) imaging, colour doppler ultrasonography and spiral Computed Tomography (CT) reconstruction often confirms early stage vascular injury [5].
In the present case report, early diagnosis of vascular injury was not made. Colour Doppler was done 15 days after the injury which revealed monophasic severely dampened flow in anterior tibial artery, posterior tibial artery and dorsalis pedis artery. If the diagnosis of vascular injury in the patients having an open injury is not done early, multiple injuries and other damages endanger life which may be due to the distraction of the attending doctor especially when the dorsal and posterior tibial arterial palpation is feeble along with decreased skin temperature of the injured limb. Such symptoms are mistakenly thought to be signs of shock or caused by vascular spasms. Vascular intimal injury and partial vascular embolism are induced in some patients due to the blunt force nature of the injury [5].
In the present case report, the patient had an open injury along with raised WBC count and normal temperature of limb so he was thought to be in septic shock.
In a study done by Xu YQ et al., out of 15 patients, diagnosis of vascular injury was missed in 2 cases, similar to the present case report [5]. A study done by Dutronc H et al., showed Staphylococcus as the most frequent organism after lower limb amputations and 44% of the patients in the study needed surgical revision in addition to antibiotic treatment. The second common organism isolated was Pseudomonas aeruginosa and that the organism was cultured mostly from samples of patients that underwent amputation due to traumatic reasons [6]. In the present case, the patient had infected stump with slough and serial cultures revealed growth of multiple organisms including MRSA and Pseudomonas aeruginosa.
A study by Loro A et al., reported that out of 123 patients 26 had revision surgery for amputation, out of which 22 required revision surgery because of soft tissue infection and gangrene of stump [7]. It has been noticed that a bad stump formation and infection are the most common indications for revision amputation [1]. In the present case also revision surgery was planned after primary amputation due to presence of infection.
There are many factors which play an important role in healing of the amputated stump and they include careful surgery, meticulous tissue handling, accurate skin apposition and effective dressings [8]. Stump problems like ulcer, delayed wound healing, excess soft tissues and prominent bone under skin, spurs and neuroma causing stump pain are very common in patients undergoing traumatic amputations [9]. In the present case, the patient had excellent wound healing and did not have any significant stump problems after revision surgery. Also, the patient tolerated the prosthesis well, except for having restricted mobility due to above-knee amputation.
Conclusion(s)
Amputation and the revision surgeries remains a challenge to both the treating surgeon and patient. In the index case, vascular injury was the cause for the initial amputation and later infection and poor stump formation was the cause for revision surgery. Greatest attention should be given to prevent these causes which lead to loss of limb. Early detection of the vascular injury can be done by assessing the clinical manifestations combined with colour doppler study and blood vessel angiography. Revision surgery can be prevented by following standard aseptic precautions, prophylactic antibiotics. As the success of the revision surgeries is rare all the effort should be made to focus on preventable causes of amputation and revision surgery.
[1]. Kumar D, Singh S, Shantanu K, Goyal R, Khushwaha NS, Gupta AK, Need of Revision of lower limb amputations in a north indian tertiary centreJ Clin Diagn Res 2015 9(12):RC01-03.10.7860/JCDR/2015/16385.688626813957 [Google Scholar] [CrossRef] [PubMed]
[2]. Imerci A, Ozaksar K, Gurbuz Y, Sugun TS, Canbek U, Savran A, Popliteal injury associated with blunt trauma to the knee without fracture or dislocationWest J Emerg Med 2014 15(2):145-48.10.5811/westjem.2013.12.1822324672601 [Google Scholar] [CrossRef] [PubMed]
[3]. Moyer HR, Minter J, Salvage of an infected below-knee amputation with chlorhexidine and bi-layer dermal matrix: A case reportSurgical Infections Case Reports 2016 1(1):47-51.10.1089/crsi.2016.0007 [Google Scholar] [CrossRef]
[4]. Ajibade A, Akinniyi OT, Okoye CS, Indications and complications of major limb amputations in Kano, NigeriaGhana Med J 2013 47(4):185-88. [Google Scholar]
[5]. Xu YQ, Li Q, Shen TG, Su PH, Zhu YZ, Early diagnosis and treatment of trauma in knee joints accompanied with popliteal vascular injuryInt J Clin Exp Med 2015 8(6)9421-29 [Google Scholar]
[6]. Dutronc H, Gobet A, Dauchy FA, Klotz R, Cazanave C, Garcia G, Stump infections after major lower-limb amputation: A 10-year retrospective studyMed Mal Infect 2013 43(11-12):456-60.10.1016/j.medmal.2013.09.00324210847 [Google Scholar] [CrossRef] [PubMed]
[7]. Loro A, Franceschi F, Samwel JM, Revision of amputation stumps in Dodoma- TanziaProsthet Orthot Int 1992 16(2):133-36.8.10.3109/030936492091643261408673 [Google Scholar] [CrossRef] [PubMed]
[8]. McIntosh J, Earnshaw JJ, Antibiotic prophylaxis for the prevention of infection after major limb amputationEur J VascEndovasc Surg 2009 37(6):696-703.10.1016/j.ejvs.2009.01.01319328028 [Google Scholar] [CrossRef] [PubMed]
[9]. Liu K, Tang T, Wang A, Cui S, Surgical revision for stump problmes after traumatic above-ankle amputations of the lower extremityBMC Muscoskelet Disord 2015 16(48):01-07.10.1186/s12891-015-0508-325887565 [Google Scholar] [CrossRef] [PubMed]