Dandy-Walker Malformation with an Occipital Cephalocele in an Infant: A Case Report
Muhammad Baba Sule1, Ibrahim Haruna Gele2, Yakubu Bababa Shirama3, Mohammed Abacha4
1 Lecturer and Consultant Radiologist, Department of Radiology, Usmanu Danfodiyo University Teaching Hospital (UDUTH), Sokoto, Nigeria.
2 Consultant Radiologist, Department of Radiology, Usmanu Danfodiyo University Teaching Hospital (UDUTH), Sokoto, Nigeria.
3 Consultant Radiologist, Department of Radiology, Abubakar Tafawa Balewa Teaching Hospital, Bauchi, Nigeria.
4 Lecturer, Department of Radiography, Usmanu Danfodiyo University (UDUS), Sokoto, Nigeria.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Muhammad Baba Sule, Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria.
E-mail: muhammadsule@yahoo.com
Dandy-Walker Malformation (DWM) is an unusual hereditary intracranial anomaly that affects the cerebellum and its components and is also characterised with an enlarged posterior fossa. DWM can appear dramatically or develop unnoticed and occurs with occipital cephalocele in about 5% of cases. This is a case report of a 10-month-old male child with DWM who had a co-existing occipital cephalocele and presented on account of hydrocephalus and poor developmental milestone. He had a Contrast Enhanced Computed Tomographic (CECT) scan of the brain; which showed a posterior fossa cysts, a hypoplastic cerebellar vermis with a dysmorphic fourth ventricle that appear continuous with the posterior fossa cyst giving the so called ‘key hole deformity’. There is also associated hydrocephalus with an occipital cephalocele.
Congenital, Dysplastic, Hydrocephalus, Posterior fossa
Case Report
A 10-month-old male infant was referred for a CECT scan on account of multiple birth defects; hydrocephalus, occipital swelling and kyphoscoliosis of the vertebral spine. Patient had a history of hypotonia, poor sucking with little or no cry at birth and also a history of delayed milestone. No family history of similar occurrence was noted. On physical examination, he was oriented and not in any respiratory distress. He was not pale or dehydrated. The muscle tone were on the low grade (grade of III). His haemoglobin count and full blood count with differentials were within normal limits for his age group. He had a CECT scan of the brain following sedation by the anaesthetic team of doctors; which showed a huge posterior fossa cysts, a hypoplastic cerebellar vermis with a dysmorphic fourth ventricle that appear continuous with the posterior fossa cyst giving the so called key hole deformity [Table/Fig-1,2]. There was also associated hydrocephalus involving the remaining ventricles ([Table/Fig-2] showing dilated lateral ventricle). There was a defect in the occipital skull vault inferiorly with extrusion of the meninges and herniation of the brain parenchyma with Cerebrospinal Fluid (CSF); the occipital cephalocele [Table/Fig-1,3]. Magnetic resonance imaging was not performed because of its unavailability at our centre at the time of this report. Plain radiograph of the spine showed normal vertebral bodies with no fusion or defects. The patient subsequently had ventriculoperitoneal and cystoperitoneal shunts with surgical repair (cranioplasty) of the occipital cephalocele by the neurosurgical team.
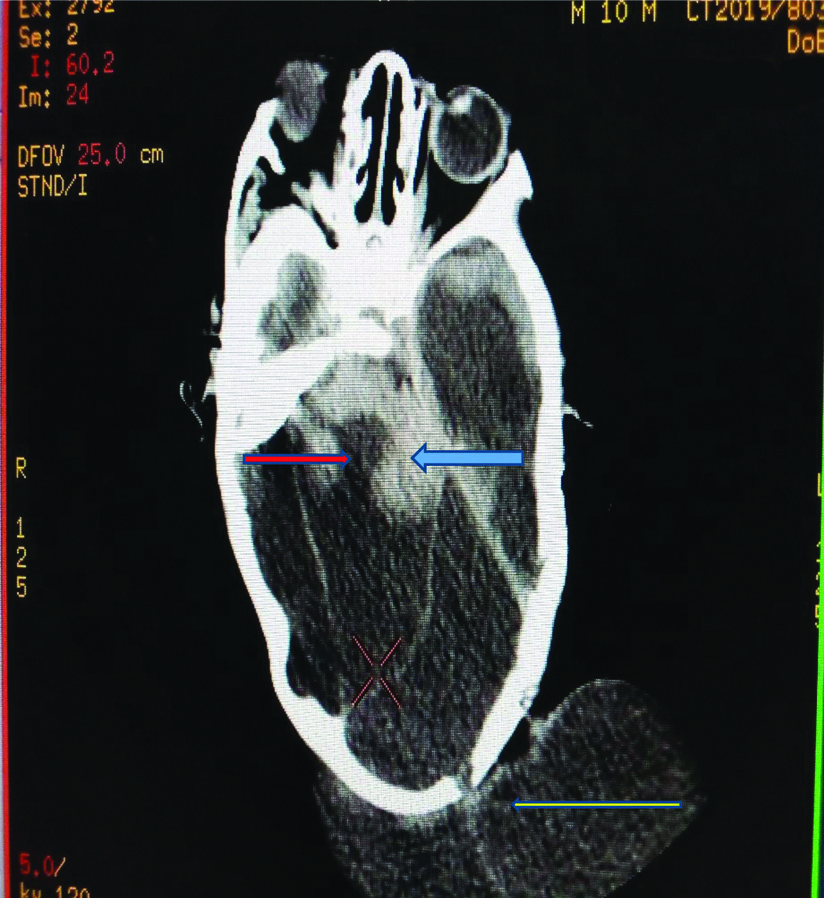
Axial computed tomogram of the brain showing dysplastic cerebellum and vermis (blue arrow) with a dysplastic fourth ventricle (red arrow) seen continuous with a huge posterior fossa cyst; Key hole deformity. The occipital cephalocele is also demonstrated (yellow arrow).
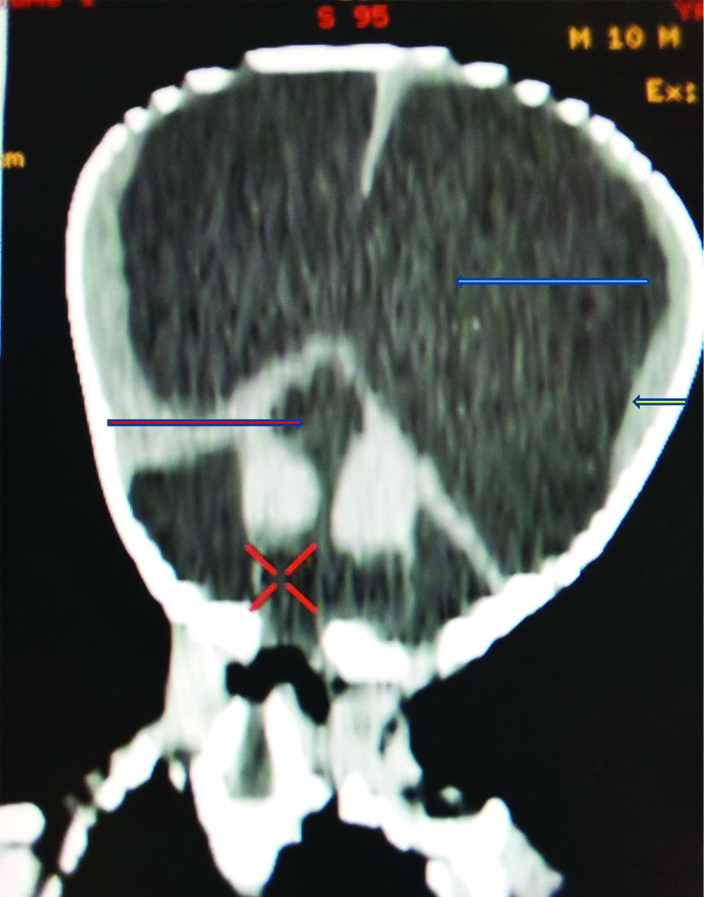
Reconstructed coronal computed brain tomogram showing dilated lateral ventricles (blue arrow), thinned cerebral mantle (yellow arrow), dysplastic fourth ventricle communicating with the posterior fossa cyst giving the key hole deformity (red arrow).
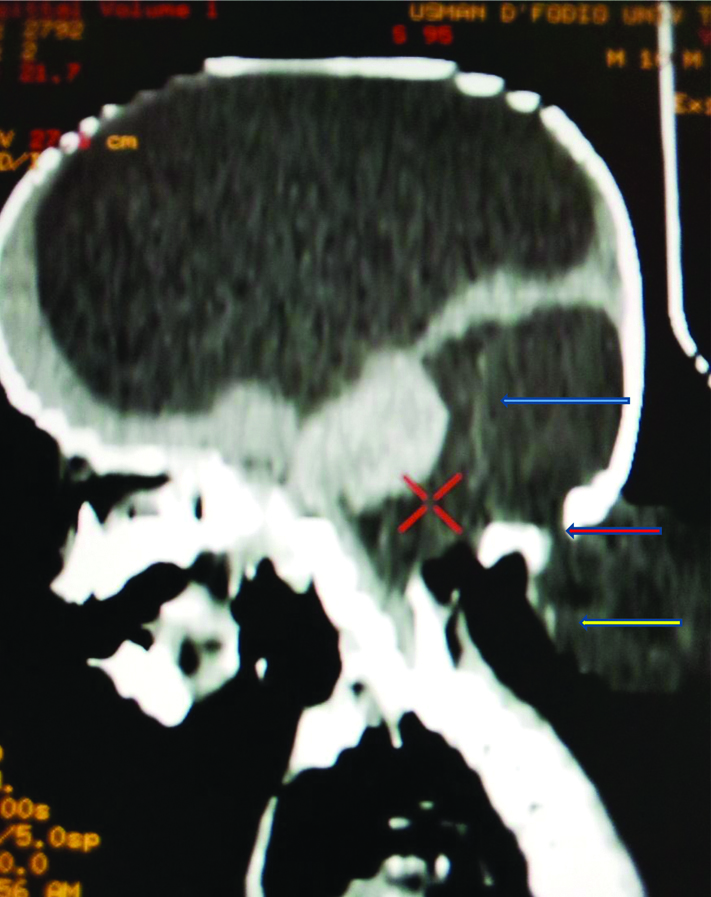
Sagittal reconstructed computed tomogram showing posterior fossa cyst (blue arrow), occipital skull vault defect (red arrow) with cephalocele (yellow arrow).
Discussion
DWM is a congenital intracranial anomaly that affects the cerebellum and few of its other parts such as cerebellar vermis, fourth ventricle and it’s characterised with an enlarged posterior fossa [1]. The index case presented with dysplastic cerebellum and cerebellar vermis, dysplastic fourth ventricle and a large posterior fossa cysts in agreement to this literature. This occurs as an autosomal dominant inherited disorder and occur in 25000-35000 pregnancies [1,2]. In this case, the present patient was the only sibling that was affected. DWM has an incidence of about 1 in 30000 live births with a slight female preponderance [3]. The index case happens to be a male patient which was not in agreement to the literature. DWM is the severe form of the Dandy walker syndrome or complex, the syndrome has three types; the dandy walker syndrome malformation, DWS mega cisterna magna and DWS variant [4,5]. This case presented with features of Dandy-Walker syndrome or complex. DWM is further defined by characteristic triad consisting of complete or partial agenesis of the vermis, cystic dilatation of the fourth ventricle, an enlarged posterior fossa with upward displacement of lateral sinuses with tentorium and torcular herophili [6,7]. Present case had similar presentations further agreeing to these literatures. DWM has a milder variant called Dandy-Walker variant which is a condition with variable hypoplasia of the cerebellar vermis with or without an enlarged cisterna magna, communication between the fourth ventricle and the arachnoid space and no hydrocephalus [8,9]. The index case was a confirmed case of DWM with classical triad of dysplastic cerebellum and cerebellar vermis, dysplastic fourth ventricle and a large posterior fossa cysts contrary to what comprises the Dandy-Walker variant.
DWM is associated with many syndromes such as Klippel-Fiel syndrome, Aicardi syndrome, Trisomy’s and PHACE syndrome to mention a few. The PHACE syndrome which is an acronym referring to posterior fossa defects, haemangioma’s, arterial anomalies, cardiac defects and eye abnormalities may on very rare occasion be associated with DWM [10-12]. The index case had a posterior fossa defect/anomaly the occipital cephalocele with herniation of the brain tissue, CSF and meninges. The association of DWM with occipital encephalocele is rare and it is in about 5% of cases [13,14], the reported case also had a coexisting occipital encephalocele conforming to these literatures. There are reported anomalies outside the CNS in association with DWM which include cardiac defects, craniofacial abnormalities, gastrointestinal abnormalities, genitourinary abnormalities, respiratory aberrations and musculoskeletal dysmorphisms [15-19]; these were however not demonstrated in this patient.
Conclusion(s)
DWM though very rare is occasionally diagnosed from imaging, these cases should be soughted out and well evaluated for possible causative agent and to improve the quality of life of these group of individuals presenting with features of DWM.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Nov 20, 2019
Manual Googling: Jan 13, 2020
iThenticate Software: Apr 24, 2020 (13%)
[1]. Tadakamadla J, Kumar S, Mamatha GP, Dandy-Walker malformation: An incidental findingIndian J Hum Genet 2010 16(1):33-35.10.4103/0971-6866.6493620838490 [Google Scholar] [CrossRef] [PubMed]
[2]. Cordoso J, Lange MC, Loranzoni PJ, Scola RH, Wernek LC, Dandy-Walker syndrome in adult mimicking Myasthemia gravisArq Neuropsiquiatr 2007 65(1):173-75.10.1590/S0004-282X200700010003717420852 [Google Scholar] [CrossRef] [PubMed]
[3]. Sreelatha S, Vedavathy N, Sathya P, Hanji N, Dandy-Walker variant: A case reportSch J Med Case Rep 2014 2:40-41.Available at: http://saspjournals.com/wp-content/uploads/2014/01/SJMCR-2250-41.pdf [Google Scholar]
[4]. Dandy-walker syndrome. Wikipedia. https/en.m.wikipedia.org. Assessed on 19th November 20110 [Google Scholar]
[5]. Altman NR, Naidich TP, Braffman BH, Posterior fossa malformationsAJNR Am J Neuroradiol 1992 13(5):691-724. [Google Scholar]
[6]. Hosam AH, Dandy-Walker malformationEgypt J Hum Genet 2007 8(2):115-116. [Google Scholar]
[7]. Hart MN, Malamud N, Ellis WG, The Dandy-Walker syndrome. A clinic pathological study based on 28 casesNeurology 1972 22(8):771-80.10.1212/WNL.22.8.7714343429 [Google Scholar] [CrossRef] [PubMed]
[8]. Yasodha MR, Dulangi MAD, Swarna W, Dandy-Walker malformation presenting with psychological manifestationCase Rep Psychiatry 2016 2016:01-04.10.1155/2016/910430627493822 [Google Scholar] [CrossRef] [PubMed]
[9]. Kim JH, Kim TH, Choi YC, Chung SC, Moon SW, Impulsive behaviour and recurrent major depression associated with Dandy-Walker variantPsychiatry Investig 2013 10(3):303-05.10.4306/pi.2013.10.3.30324302956 [Google Scholar] [CrossRef] [PubMed]
[10]. Tiwary AK, Mishra DK, Jha G, A rare face of PHACE syndrome with Dandy-Walker malformation, micropthalmia with leukocoria, hearing loss and involuting segmental facial hemangiomaIndian J Paediatr Dermatol 2017 18(3)::223-26.10.4103/2319-7250.206056 [Google Scholar] [CrossRef]
[11]. Frieden IJ, Reese V, Cohen D, PHACE syndrome. The association of posterior fossa brain malformations, hemangiomas, arterial anomalies, coarctation of the aorta and cardiac defects, and eye abnormalitiesArch Dermatol 1996 132(3):307-11.10.1001/archderm.1996.038902700830128607636 [Google Scholar] [CrossRef] [PubMed]
[12]. Todo T, Usui M, Ariaki F, Dandy-Walker syndrome forming a giant occipital meningocele- case reportNeurol Med Chir (Tokyo) 1993 33(12):845-50.10.2176/nmc.33.8457512233 [Google Scholar] [CrossRef] [PubMed]
[13]. Cakmak A, Zeyrek D, Cekin A, Karazeybek H, Dandy-Walker syndrome together with occipital encephaloceleMinerva Pediatr 2008 60:465-68. [Google Scholar]
[14]. Mostafa EF, Frank G, Dandy-Walker malformationhttps://radiopaedia.org/articles/dandy-walker-malformation. Accessed on 40th December 20110 [Google Scholar]
[15]. Gaffiney RE, Fisher KL, Dandy-Walker malformation with concomitant agenesis of the corpus callosum as investigated by neonatal ultrasonographyJournal of Diagnostic Medical Sonography 2017 33(4):318-23.10.1177/8756479317697276 [Google Scholar] [CrossRef]
[16]. Olson GS, Halpe DC, Kaplan AM, Spataros J, Dandy-Walker malformation and associated cardiac anomaliesChild’s Brain 1981 8(3):173-80.10.1159/0001199817238134 [Google Scholar] [CrossRef] [PubMed]
[17]. Pascual-Castroveijo I, Velez A, Pascual-Pascual SI, Roche MC, Villarejo F, Dandy-Walker malformation: Analysis of 49 casesChild’s Neuro Syst 1991 7(2):88-97.10.1007/BF002478631863935 [Google Scholar] [CrossRef] [PubMed]
[18]. Zaki MH, Masri A, Grujor A, Gleason JG, Rosti RO, Dandy-Walker malformation, genitourinary affectation, and intellectual disability in two familiesAm J Med Genet A 2015 167(11):2503-07.10.1002/ajmg.a.3722526109232 [Google Scholar] [CrossRef] [PubMed]
[19]. Stevens CA, Lachman RS, New lethal skeletal dysplasia with Dandy-Walker malformation, congenital heart defects, abnormal thumbs, hypoplastic genetalia, and distinctive facieAm J Med Genet A 2010 152(8):1915-18.10.1002/ajmg.a.3348820602491 [Google Scholar] [CrossRef] [PubMed]