Subarachnoid Cyst in the Patient with Psychosis: A Rare Case
Poonam Bharti1, Sana Usmani2, Gunjan Jindal3
1 Associate Professor, Department of Psychiatry, Maharishi Markandeshwar Deemed to be University, Ambala, Haryana, India.
2 Postgraduate Student, Department of Psychiatry, Maharishi Markandeshwar Deemed to be University, Ambala, Haryana, India.
3 Assistant Professor, Department of Radiology, Maharishi Markandeshwar Deemed to be University, Ambala, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Sana Usmani, Guru Nanak Colony, House No-73, Street No. 6, Opp. Medical College, Faridkot, Punjab, India.
E-mail: poonambharti109@gmail.com
Arachnoid cysts develop between arachnoid membrane and the surface of the brain. These cysts may cause neurological deficits as well as neuropsychiatric symptoms. Intracranial cysts are usually picked accidently on MRI brain studies. Mostly they are congenital and have gender prediction. Here, the authors reported a case of 57-year-old male who came with the complaint of headache, aggressive behaviour and psychotic symptoms. On neuroimaging, he had subarachnoid frontal cyst causing buckling of left frontal region which may be the underlying cause of his psychiatric symptoms. He was admitted and treated with Risperidone, Clonazepam and Naproxen with which he showed gradual improvement in the symptoms.
Aggressive behaviour, Headache, Psychotic symptoms
Case Report
A 57-year-old male, muslim shop-keeper, educated till 6th standard came to the Outpatient Department (OPD) of Psychiatry with on and off headache, aggressive outbursts, decreased sleep, and episodes of irrelevant talk and hearing of voices since 2 years. He had also adopted a very hostile attitude towards his family members. He used to say that they are talking about him and want to harm him which lead to frequent fights at home. Patient’s socio-occupational life was hampered. He started having frequent fights with his customers and was unable to manage his financial matters effectively at his shop. No history of any substance abuse or any head trauma. There was a history of abusing the bystanders and throwing stones at them without any provocation after the prayers in a nearby mosque. Next day after this episode, the family members brought him to the hospital and got him admitted. Patient was found to be irritable with increased psychomotor activities, impaired social judgment, delusion of reference and auditory hallucinations on mental status examination.
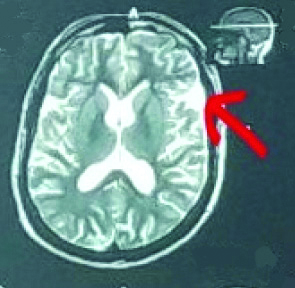
All routine blood investigations were within normal limits. MRI 2D head was done which showed a subarachnoid cyst (13.5 mm × 9.5 mm) in the left frontal region causing mild buckling of cerebral cortex, with mild atrophy [Table/Fig-1]. Axial T2W image shows a hyper-intense extra-axial lesion in the left frontal (lobe) suggestive of arachnoid cyst. The radiological differential for such presentation can be epidermoid cyst and chronic subdural haemorrhage. Epidermoid cyst was ruled out as there was no restricted diffusion seen and it couldn’t be subdural haemorrhage as there was no history of any trauma.
Axial T2W image showing extra axial fluid intensity lesion (Arrow) in left frontal lobe suggestive of arachnoid cyst.
Patient was started with Risperidone 4 mg, clonazepam 0.5 mg and naproxen 500 mg daily. Slight improvement in aggressive outbursts, psychotic symptoms and sleep disturbances (behavioural component) with decrease in episodes of headache was seen after one week of inpatient stay. After gradual improvement after 10 days, patient was discharged and is on regular follow-up, stable with medications.
Discussion
Intracranial arachnoid cyst has been reported to occur in 1.4% of general population on brain MRI studies [1]. Subarachnoid cyst is mostly congenital, which are diagnosed accidently. There is a gender predilection of the cyst in which temporal cysts are in men, whereas cerebellopontine are seen in women [2]. Patients with intracranial arachnoid cysts presents with psychiatric symptoms as their chief complaints [3]. Arachnoid cyst impairs not only cognitive function but also executive function [4]. Organic as well as functional conditions which lead to psychotic symptoms affecting the thought and perception of the patient leads to global social impairment [5]. Headache, dizziness and convulsive episodes are the most common clinical symptoms presented in such cases [6]. Temporal and frontal cysts cause many psychiatric symptoms [7].
The patient presented with a history of headache, aggressive behaviour and sleep disturbance since last 2 years, he was never investigated and treated before this. This association between the patient’s abnormal behaviour and subarachnoid cyst can be best explained as psychotic symptoms started along with headache so this reflects that organic cause can be the reason behind such behaviour. Further, MRI findings support the symptomology. No past or family history of psychiatric illness is there. A case reported by da Silva JA et al., where aggressive behaviour, delusions and complex auditory hallucinations were seen in patient with arachnoid cyst in left temporal and frontal lobe in supportance with the findings of the index case [8]. Another case reported by Mironov A et al., showed improvement in psychotic symptoms with delirium having subarachnoid cyst in left temporal lobe from Risperidone which supports the index case [9].
In the present case, there is clinically possible link between subarachnoid cyst and psychiatric symptoms. Guliani GS reported a case of acute onset of psychotic behaviour with heaviness of head associated with arachnoid cyst in occipital region [10]. Patient showed marked improvement with Risperidone over Olanzapine. This case report finding are very much similar with the findings of the index case where psychiatric symptoms were associated with the organic cause and patient showed improvement with the use of Risperidone. Another interesting finding of this case is Risperidone use may found to be effective in cases of psychosis associated with arachnoid cyst. This finding would support use of atypical anti-psychotics for treatment of psychosis related to organic aetiology.
Many such cases with similar presentation go unnoticed, either misdiagnosed or untreated as neuroimaging is not performed in each and every case with similar presentation. This is an effort to bring in attention, the possibility of psychiatric symptoms with the presence of organic deficits in form of arachnoid cyst. With the progression of neuroimaging the relationship between psychiatric disorders with organic brain changes may become clearer. This case helps to integrate clinical manifestations with structural finding, hence opening avenues for more such investigations, diagnosis and therapeutic approach.
Conclusion(s)
It is not easy to tell whether the presenting cyst and symptoms are concordance in regarding the patient’s over all psychiatric symptoms. Though there are changes in the cerebral cortex in frontal lobe with major psychiatric symptoms associated with them may lead to this possibility that the lesion might have played a role in the aetiopathogensis of the psychotic symptoms, which cannot be excluded. These types of findings with organic lesion are required to be taken-up more extensively to establish the possibility and optimise the therapeutic approach in cases that involve co-existence of psychosis and subarachnoid cyst.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Mar 03, 2020
Manual Googling: Apr 10, 2020
iThenticate Software: Apr 22, 2020 (11%)
[1]. Al-Holou WN, Terman S, Kilburg C, Garton HJ, Muraszko KM, Maher CO, Prevalence and natural history of arachnoid cysts in adultsJ Neurosurg 2013 118(2):222-31.10.3171/2012.10.JNS1254823140149 [Google Scholar] [CrossRef] [PubMed]
[2]. Helland CA, Lund-Johansen M, Wester K, Location, sidedness, and sex distribution of intracranial arachnoid cysts in a population-based sampleJ Neurosurg 2010 113(5):934-39.10.3171/2009.11.JNS08166320095787 [Google Scholar] [CrossRef] [PubMed]
[3]. Gelabert-Gonzalez M, Intracranial arachnoid cystsRev Neurol 2004 39(12):1161-66.10.33588/rn.3912.200440015625636 [Google Scholar] [CrossRef] [PubMed]
[4]. Gjerde PB, Schmid M, Hammar Å, Wester K, Intracranial arachnoid cysts: Impairment of higher cognitive functions and postoperative improvementJ Neurodev Disord 2013 5(1):2110.1186/1866-1955-5-2123985219 [Google Scholar] [CrossRef] [PubMed]
[5]. Richards CF, Gurr DE, PsychosisEmerg Med Clin North Am 2000 18(2):253-62.10.1016/S0733-8627(05)70122-X [Google Scholar] [CrossRef]
[6]. Helland CA, Wester K, Intracystic pressure in patients with temporal arachnoid cysts: A prospective study of preoperative complaints and postoperative outcomeJ Neurol Neurosurg Psychiatry 2007 78(6):620-23.10.1136/jnnp.2006.10186517158556 [Google Scholar] [CrossRef] [PubMed]
[7]. Wester K, Intracranial arachnoid cysts- Do they impair mental functions?J Neurol 2008 255(8):1113-20.10.1007/s00415-008-0011-y18677648 [Google Scholar] [CrossRef] [PubMed]
[8]. da Silva JA, Alves A, Talina M, Carreiro S, Guimarães J, Xavier M, Arachnoid cyst in a patient with psychosis: Case reportAnn Gen Psychiatry 2007 6(1):1610.1186/1744-859X-6-1617598903 [Google Scholar] [CrossRef] [PubMed]
[9]. Mironov A, John S, Auerbach J, Jamaleddine G, Acute onset of psychosis in a patient with a left temporal lobe arachnoid cystCase Rep Med 2014 2014:20402510.1155/2014/20402524715905 [Google Scholar] [CrossRef] [PubMed]
[10]. Guliani GS, Association of episodic psychotic behaviour with an arachnoid cyst of the brain. A rare case reportJ Child Adolesc Psych 2018 2(3):01-02. [Google Scholar]