Too Much Stress- A Rare Case of Takotsubo Cardiomyopathy
Soorya Narayanan Balasubramani1, Mohamed Kasim Abdul2
1 Postgraduate, Department of General Medicine, Mahatma Gandhi Medical College and Research Institute, Kumbakonam, Tamil Nadu, India.
2 Senior Resident, Department of General Medicine, Mahatma Gandhi Medical College and Research Institute, Pondicherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Soorya Narayanan Balasubramani, 15, Town Extension, Gandhi Nager, Kumbakonam, Tamil Nadu, India.
E-mail: sooryab99@gmail.com
Takotsubo syndrome is a reversible, stress-induced transient systolic and diastolic dysfunction. It was first described as a characteristic ballooning of left ventricular apex which closely resembles a Japanese fishing pot. Here the authors present a case report of a 40-year-old female who was posted for elective tonsillectomy, that developed sudden de-saturation immediately post-intubation, examination showed bilateral extensive and ECG showed symmetrical T wave inversion in leads V1 to V6 and troponin I was positive. A diagnosis of Perioperative myocardial infarction was made and hence patient was taken for coronary angiogram which was found to be normal. The left ventricular angiogram showed a typical finding of apical ballooning. The patient was diagnosed to have- Takotsubo Syndrome. Treatment included tablet Torsemide, Ramipril and Metoprolol. She was discharged after 7 days as the vitals got normalised.
Apical ballooning, Fishing pot, Stress cardiomyopathy
Case Report
A 40-year-old female, a known case of Type 2 diabetes mellitus for the past 2 years on oral anti-diabetic medications, was planned for elective tonsillectomy for chronic tonsillitis. The pre-operative period was unevent full and the patient was taken for the proposed procedure.
Before intubation, the baseline vitals were PR: 86/minute BP: 126/70 mmHg. The patient was intubated and initiated on general anaesthesia with induction agent Propofol and Vecuronium was used as a muscle relaxant. Following intubation and induction, patient had a rise in PR 110/minute and BP 200/110 mmHg, following which there was a fall in saturation. Systemic examination showed bilateral extensive crepitation. A provisional diagnosis of Acute Pulmonary oedema was made and the proposed surgery was cancelled.
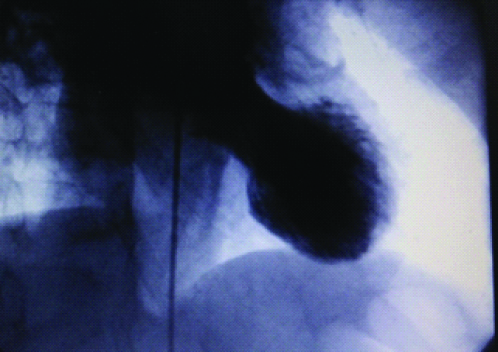
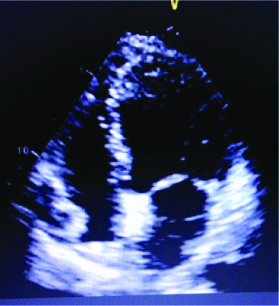
A provisional diagnosis of the Acute Coronary Syndrome (ACS) was made and the patient was started on Tablet Aspirin 150 mg OD, Ticagrelor 90 mg BD, Inj. Enoxaparin 60 mg BD and Inj. Lasix 40 mg BD were started. The patient improved symptomatically and was subsequently extubated. The patient was taken for Coronary Angiogram and showed normal epicardial coronaries with the right dominant circulation. The left ventricular angiogram showed a typical finding of apical ballooning [Table/Fig-1]. 2D echocardiogram of the patient showed the characteristic feature of systolic dysfunction and apical balooning [Table/Fig-2].
Apical ballooning Demonstrated in Left ventricular angiogram.
Apical ballooning in 2D ECHO.
The patient was diagnosed to have Takotsubo Syndrome. Treatment was started with tablet Torsemide 10 mg BD, Tablet Ramipril 5 mg OD and Tablet Metoprolol 50 mg BD. Patient vitals were normalised-BP: 120/70 mmHg, PR: 78/minute, saturation was 98% in room air. Hence, she was discharged after 7 days of hospitalisation.
Discussion
Takotsubo syndrome is characterised by a stress-induced transient systolic and diastolic dysfunction. It was first described as a characteristic ballooning of left ventricular apex which closely resembles a Japanese fishing pot which was an octopus pot [1]. The first case was reported in Japan in 1990. This apical ballooning cardiomyopathy occurs in 1%-2% of patients presenting with ST-Elevation Myocardial Infarction (STEMI) or cardiac troponin positive ACS [1].
It is otherwise called as apical ballooning syndrome, stress-induced cardiomyopathy which leads to a reversible left ventricular systolic (predominantly apical) dysfunction. The main underlying pathogenesis was unclear, and most of the time physical and emotional stress triggers with systemic catecholamine excess lead to Takotsubo syndrome [2], in the present case physical stress of intubation would have probably acted as a stress factor. This reversible myocardial injury was secondary to coronary vasospasm and rat models have shown that increased distribution of adrenergic receptors in the left ventricular apex have attributed to the predilection of affection of Left ventricular apex [3]. The common stressors associated were physical factors like cocaine use, non-cardiac surgery, severe pain, thyrotoxicosis, and General anaesthesia; the common emotional factors were the death of a family member, severe argument, financial loss and accidents.
Physical factors are more common than the emotional trigger and also this syndrome is more common in women less than 50 years of age [4]. It was also found that many drugs are also associated with TCM [5]. Even though there are various triggers associated with TCM up to 30% of cases the cause remains unidentified [6]. A systematic review showed 20 drugs that might be induced in TCM, most of them are main agents that mimic the actions of epinephrine or norepinephrine, Oxymetazoline and anticholinergic or parasympatholytic drugs such as atropine, agents that inhibit of reuptake of catecholamines from synaptic cleft such as nortriptyline some other drugs like opioid (oxycodone), cephalosporin antibiotic (cefotiam), phosphodiesterase III inhibitor (anagrelide), thyroid hormone is also associated [5].
The main modality of diagnosis of TCM is 2D Echocardiography [Table/Fig-2]. Cardiac MRI shows absence of late Gadolinium enhancement. Coronary angiogram shows usually normal/non-significant lesion and Left Ventricular Angiogram which shows the ballooning of the ventricle. On left ventricular angiogram there are predominantly 4 types; Apical type/Mid-ventricular type/basal type/Focal type [6].
The main differential diagnoses are ACS, Cocaine related vasospastic angina, Myocarditis and Pheochromocytoma [7]. These can be ruled out by coronary angiogram and serum markers likes Metanephrines and Vanilmandelic acid.
Medical management with drugs like diuretics, angiotensin-converting enzyme inhibitors and beta-blockers is common, studies have also favoured the use of levosimendan in TCM [8].
Conclusion(s)
TCM is reversible stress-induced systolic and diastolic dysfunction, which most commonly occurs secondary to physical and emotional factor. With prompt identification and management, morbidity can be reduced.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Feb 04, 2020
Manual Googling: Mar 23, 2020
iThenticate Software: Apr 16, 2020 (6%)
[1]. Komamura K, Fukui M, Iwasaku T, Hirotani S, Masuyama T, Takotsubo cardiomyopathy: Pathophysiology, diagnosis and treatmentWorld J Cardiol 2014 6(7):602-09.10.4330/wjc.v6.i7.60225068020 [Google Scholar] [CrossRef] [PubMed]
[2]. Chahal GS, Polena S, Fard BS, Natesan S, Sharma S, Gintautas J, Takotsubo cardiomyopathy: Case report and review of the literatureProc West Pharmacol Soc 2008 51:48-51. [Google Scholar]
[3]. Shao Y, Redfors B, ScharinTäng M, Möllmann H, Troidl C, Szardien S, Novel rat model reveals important roles of β-Adrenoreceptors in stress-induced cardiomyopathyInt J Cardiol 2013 168(3):1943-50.10.1016/j.ijcard.2012.12.09223357048 [Google Scholar] [CrossRef] [PubMed]
[4]. Nyman E, Mattsson E, Tornvall P, Trigger factors in takotsubo syndrome- A systematic review of case reportsEur J Intern Med 2019 63:62-68.10.1016/j.ejim.2019.02.01730833207 [Google Scholar] [CrossRef] [PubMed]
[5]. Amariles P, A comprehensive literature search: Drugs as possible triggers of Takotsubo cardiomyopathyCurr Clin Pharmacol 2011 6(1):1-11.10.2174/15748841179494134021235467 [Google Scholar] [CrossRef] [PubMed]
[6]. Templin C, Ghadri JR, Diekmann J, Napp LC, Bataiosu DR, Jaguszewski M, Clinical Features and Outcomes of Takotsubo (Stress) CardiomyopathyN Engl J Med 2015 373(10):929-38.10.1056/NEJMoa140676126332547 [Google Scholar] [CrossRef] [PubMed]
[7]. Moscatelli S, Montecucco F, Carbone F, Valbusa A, Massobrio L, Porto I, An Emerging Cardiovascular Disease: Takotsubo SyndromeBiomed Res Int 2019 2019:01-09.10.1155/2019/657104531781633 [Google Scholar] [CrossRef] [PubMed]
[8]. Y-Hassan S, Tornvall P, Epidemiology, pathogenesis, and management of takotsubo syndromeClinAuton Res 2018 28(1):53-65.10.1007/s10286-017-0465-z28917022 [Google Scholar] [CrossRef] [PubMed]