Sensory Useless Hand of Oppenheim: A Rare Case
Varsha Muddasani1, Raghavendra Bakki Sannegowda2
1 MBBS Graduate, Department of Neurology, Father Muller Medical College, Mangalore, Karnataka, India.
2 Professor, Department of Neurology, Father Muller Medical College, Mangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Varsha Muddasani, No. 1023, Prestige Misty Waters Apartment, Kempapura, Hebbal, Bangalore-560024, Karnataka, India.
E-mail: vmuddasani@gmail.com
Sensory useless hand of Oppenheim was first described in 1911. It is an unusual presentation of Multiple Sclerosis. It is characterised as a functional disorder with loss of sensory modalities and preserved motor functions. Here the present authors report a case of an 18-year-old girl with acute vague symptoms described as ‘uselessness’ of left hand. Clinical examination of the neurological system was unremarkable. Imaging investigations revealed hyper-intensities in the Middle Cerebral Peduncle (MCP) and pons, suggestive of demyelination. Treatment with Intravenous and oral steroids showed improvement of symptoms. On follow-up patient presented with cerebellar symptoms after previous complete resolution. Imaging studies showed no new lesion suggesting the old lesion responsible for recurrence of new symptoms. This distribution of symptoms of space and time suggests the diagnosis of useless hand of Oppenheim a rare and uncommon presentation of multiple sclerosis.
Autoimmune, Multiple sclerosis, Sensory loss, Tumefactive demylination
Case Report
An 18-year-old female presented with acute onset of abnormal sensation over her left upper limb particularly over the hand 7-10 days before. However, she has no relevant history or family history suggestive of her presenting symptom. It was a vague symptom which she found difficult to describe. However, she could mention it as a sense of her hand being useless. She did not give any history of numbness, painful sensation in the form of tingling or burning sensations. The only description she used each time was that her hand appears to be useless. For the above symptoms, she had consulted many doctors prior to our hospital and had received symptomatic treatment. She was also diagnosed to have hysterical conversion reaction or psychosomatic illness as there were no deficits.
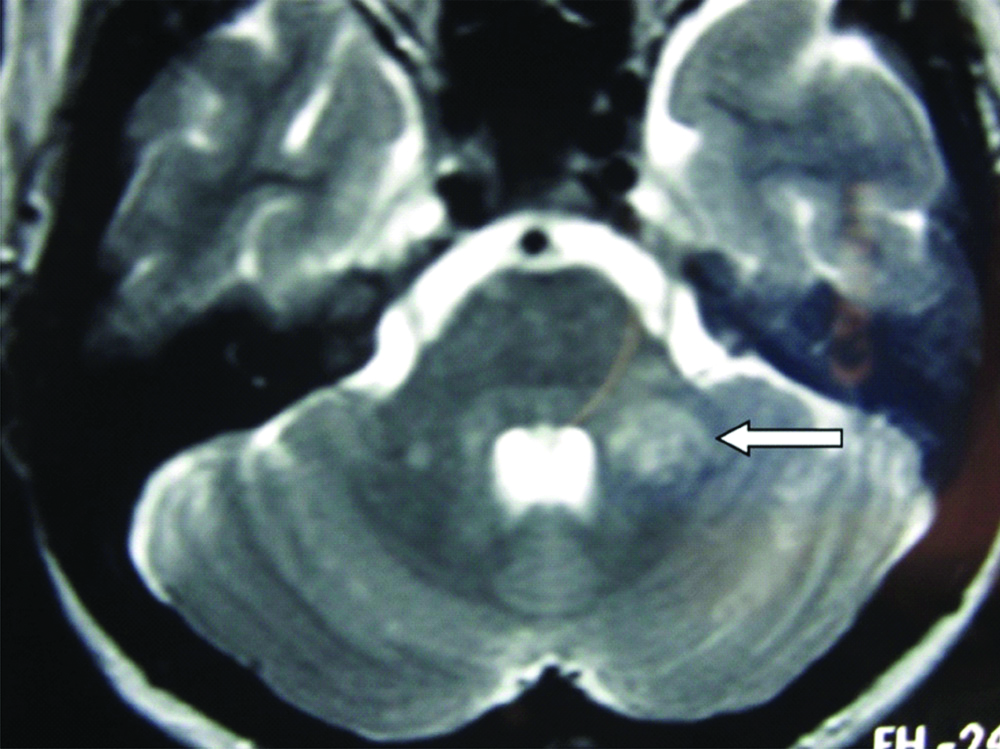
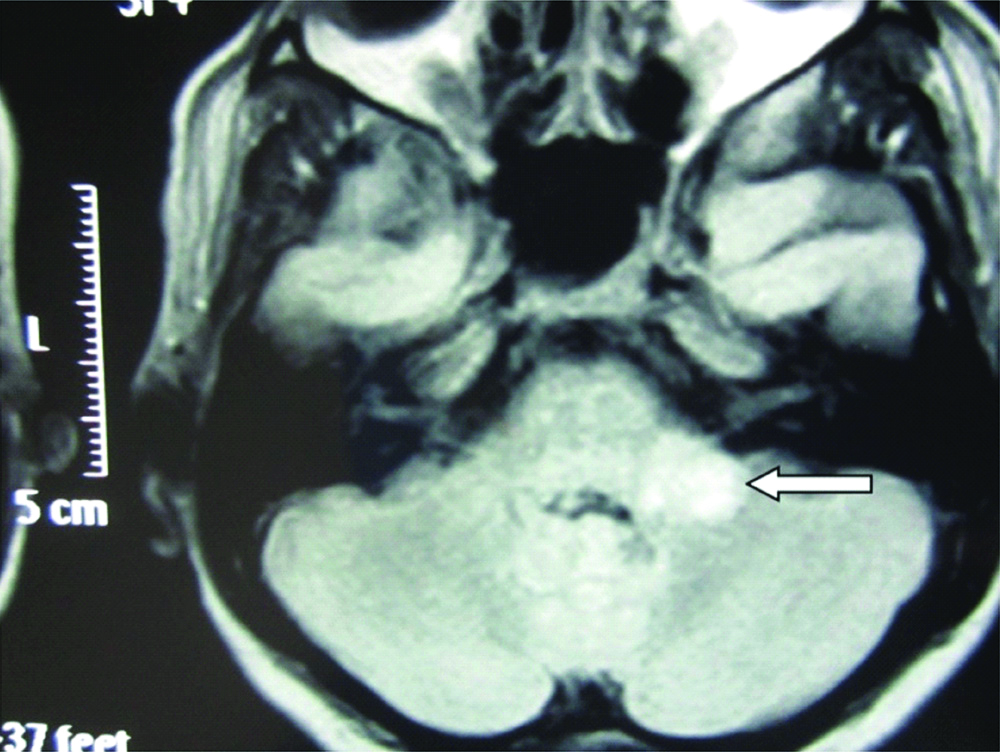
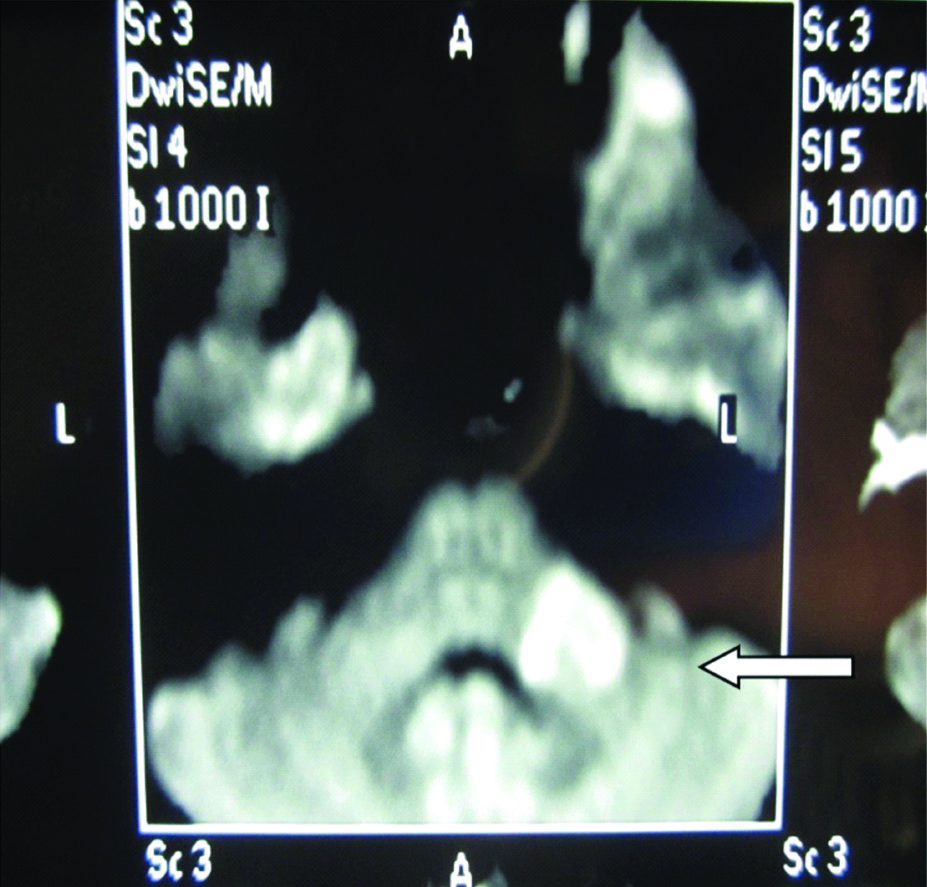
On detail neurological examination her higher mental functions were normal, cranial nerve examinations were unremarkable. Tone in all the four limbs was normal and power was 5/5 bilaterally. Reflexes were 2+ bilaterally at all the joints. Plantar reflex was flexor bilaterally. Sensory examination was normal for all the modalities and there were no cerebellar signs. Since, patient was concerned by her abnormal “sensory useless hand” description MRI brain was advised which showed T2 [Table/Fig-1] and FLAIR [Table/Fig-2] hyperintensities in left MCP and pons with peripheral restriction on DWI [Table/Fig-3] with contrast enhancement highly suggestive of demyelination. Size of the lesion was 2 cm. Rest of the brain MRI and screening of whole spine was normal. Clinical diagnosis of “Sensory useless hand of Oppenheim” secondary to demyelination was kept. Since lesion was single and size was 2 cm diagnosis of tumefactive demyelination was kept. As there was no dissemination in time and space clinically and radiologically at that time, multiple sclerosis was not considered and diagnosis of Clinically Isolated Syndrome (CIS) was made.
T2 weighted MRI showing hyper intensity in left MCP and pons.
FLAIR MRI showing hyper intensity in left MCP and pons with mild perilesional oedema.
DWI MRI showing restricted diffusion in left MCP and pons.
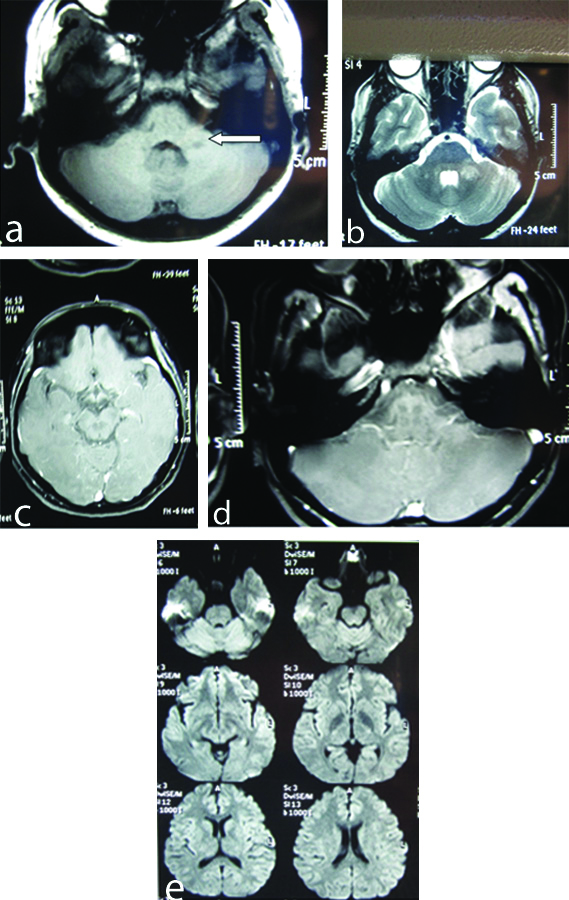
She was treated with intravenous methylprednisolone 1 gm for five days. Patient showed significant improvement in her symptoms. Her abnormal sensation completely resolved in a week and was discharged with tapering dose of oral steroids over next three weeks. Patient was absolutely asymptomatic for next three months. Three months after the recovery patient presented with acute onset cerebellar symptoms in the form of swaying towards left side while walking. There was no history of weakness of the limbs or any bulbar symptoms. On examination, patient was conscious with normal higher mental function. Cranial nerve examinations were within normal limits. Motor and sensory system examination was unremarkable. Cerebellar system examination revealed left sided horizontal gaze evoked nystagmus. Patient had left sided finger nose incoordination and left sided heel knee shin test was positive. Patient was swaying towards left while walking. For above symptoms which appeared to be dissemination in time her MRI brain and spine was repeated to rule out multiple sclerosis. MRI brain interestingly showed same previously existing demyelinating lesion in left MCP without much of contrast enhancement [Table/Fig-4a-e]. There was no increase in size nor was there any new lesion in the brain or spine. All the presenting clinical features could be explained with that same lesion more appropriately this time than previous symptom. Her CSF analysis was normal for routine and was negative for oligoclonal bands. Patient was treated again with injectable steroids followed by oral steroids. Patient again showed remarkable improvement in her symptoms. Cerebellar signs resolved gradually over next 10 days. Patient was discharged on maintenance dose of steroids this time and advised to review after one month and planned for repeat MRI to look for any resolution of the lesion.
MRI brain interestingly showed same previously existing demyelinating lesion in left MCP without much of contrast enhancement and no new lesions; (a) T1 image of previously existing demylinating lesion in left MCP; (b) T2 Image of previously existing demylinating lesion in left MCP; (c) MRI Brain with contrast axial section showed no new lesion elsewhere; (d) Contrast sequence showing no enhancement in same area and no new lesions elsewhere; (e) DWI representing different parts of the brain with no diffuse restriction lesions elsewhere.
Discussion
Multiple sclerosis has a neurological condition with multiple presentations, characteristic signs and some under-recognised presentations like the sensory useless hand of Oppenheim [1,2].
Sensory useless hand of Oppenheim was first described in 1911 by Oppenheim H as [3]: “Sensations of numbness and awkwardness in one arm, sometimes, but rarely, in both, but when both arms affected then one always more than the other. Pains may be an associated symptom. These disturbances increase rapidly, reaching ‘the greatest intensity within days, weeks, or months. The patient complains that he lets objects slip from his hand, that he finds himself unable to button his. Clothes or to distinguish between purse and knife in his pocket, etc.,”
It was thought to be due to involvement of spinothalamic tract at the level of cervical spinal cord leading to sensory loss of functions with intact motor functions of the limb [2]. Multiple cases with characteristic presentation and supportive imaging have been reported before [4-6]. A case reported by Wiblin L and Guadagno J, was about a 30-year-old woman that complained of heaviness and loss of dexterity in her right arm with evidence of asymmetric demyelinating lesions in C2 level of spinal cord [4]. Kamogawa K and Okuda B, reported a case of bilateral useless hand and astereognosis [5]. Cervical T1 MRI revealed gadolinium enhanced lesion at C3-C4 level of posterior cord. Other parts of the brain and spine were normal. Coleman RJ et al., described a case of a 38-year-old man with loss of sensation and development of involuntary movements in left hand [6].
However, in the present patient, she had similar sensory symptoms over left hand but had lesion over left MCP which has not been described earlier. Tumefactive demyelination is defined a demyelinating illness of brain usually seen in cerebral hemisphere characterised by solitary demyelinating lesion with size more than 2 cm with mass effect and can mimic brain tumour clinically and radiologically [7,8]. Tumefactive demyelination in a brain stem and peduncle involvement which was seen in our patient has not been described previously. Clinical manifestations during second admission in our patient can be explained more appropriately with same old lesion (as there was no contrast enhancement) but, mimicking dissemination in time to suggest multiple sclerosis. Recurrent manifestations in the present patient could be due to the non-resolution of the pontine and MCP lesion rather than a fresh lesion.
Tumefactive demyelination of brainstem is rare and presenting as sensory useless hand of Oppenheim is still a rare entity. Same lesion presenting as a recurrent and different clinical episode mimicking dissemination in time further adds to this rarity.
Conclusion(s)
Multiple Sclerosis has varied presentations. Useless hand of Oppenheim is an uncommon and rare presentation. Neurological manifestations include abnormal sensation and feeling of ‘uselessness’ of limb. Most common imaging finding includes lesions in cervical spine, but we report a case with lesions in the brainstem. We like to emphasise that no clinical symptom should be undermined however vague it appears to be and regular follow-up of patient helps in appropriate management of the patient.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? No
For any images presented appropriate consent has been obtained from the subjects. NA
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jan 11, 2020
Manual Googling: Feb 08, 2020
iThenticate Software: Apr 15, 2020 (5%)
[1]. Ghasemi N, Razavi S, Nikzad E, Multiple sclerosis: Pathogenesis, symptoms, diagnoses and cell-based therapyCell J 2017 19(1):01-10. [Google Scholar]
[2]. Rae-Grant AD, Unusual Symptoms and Syndromes in Multiple SclerosisContinuum (MinneapMinn) 2013 19(4):992-1006.10.1212/01.CON.0000433287.30715.0723917097 [Google Scholar] [CrossRef] [PubMed]
[3]. Oppenheim H, Discussion on the different types of multiple sclerosisThe British Medical Journal 1911 (2):729-33. [Google Scholar]
[4]. Wiblin L, Guadagno J, The useless hand of OppenheimPractical Neurology 2017 17(6):464-68.10.1136/practneurol-2016-00149428778930 [Google Scholar] [CrossRef] [PubMed]
[5]. Kamogawa K, Okuda B, Useless hand syndrome with astereognosis in multiple sclerosisMultiple Sclerosis and Related Disorders 2015 4(1):85-87.10.1016/j.msard.2014.09.21225787059 [Google Scholar] [CrossRef] [PubMed]
[6]. Coleman RJ, Russon L, Blanshard K, Useless hand of Oppenheim-magnetic resonance imaging findingsPostgrad Med 1993 69:149-50.10.1136/pgmj.69.808.1498506199 [Google Scholar] [CrossRef] [PubMed]
[7]. Fallah A, Banglawala S, Ebrahim S, Paulseth JE, Jha NK, Case Series: tumefactive demyelinating lesions: A diagnostic challengeCan J Surg 2010 53(1):69-70. [Google Scholar]
[8]. Algahtani H, Shirah B, Alassiri A, Tumefactive demyelinating lesions: A comprehensive reviewMultiple Sclerosis and Related Disorders 2017 14:72-79.10.1016/j.msard.2017.04.00328619436 [Google Scholar] [CrossRef] [PubMed]