The human hand is considered to be most marvelous due to its myriad functions. An understanding of the complexities of functions of hand to manipulate, feel and even think is evident from its role in the usage of modernised technologies like mobile phones, computers and handling types of equipment apart from its domestic role in daily activities, which requires precise functioning of all the fingers, including the thumb. Zimmer in 2012 wrote that “our hands are where the mind meets the world”. Without hand, all our daily activities would be crippled [1]. Hands are almost as expressive as words, replacing linguistic cues.
Finger Flexion Cascade (FFC) at rest is normally described as the alignment of fingers to flex through 70° to 90°, with most flexion in the little finger and least in the index finger. Based on the attachment of the flexor tendons to the bones, passive tension is created by the two joint muscles causing this functional movement [Table/Fig-1]. Allowing the wrist to drop causes smooth flexion of all fingers due to the passive tenodesis effect of long flexors of hand. In accordance to the Mosby’s medical dictionary 8th edition 2009, cascade is defined as any process that develops in stages, with each stage developing on the preceding one, often producing a cumulative effect. According to Houghton Miffliz in 2002, it may also be defined as the series of physiological processes that occur in successive stages and each of the process is dependent on the preceding one to produce a cumulating effect. At rest, the fingers form a flexion cascade which is indicated by the tips pointing to the region of scaphoid at the base of the palm [2]. Clinically, a cascade sign indicates a rotational deformity of the fingers due to metacarpal and phalangeal fractures [3].
Fingers are designed for the sophisticated task, but they work at a subconscious level while performing our daily activities. This is evident in the finely coordinated functions of flexor muscles which are located on the anteromedial aspect of the forearm, with their tendons crossing the wrist and finger joints which are arranged in an amazing manner to provide fine and infinite movements possible [4].
In a grip, the fingers flex to wrap around an object. If a power grip is needed, for example, an industrial worker grasping a screwdriver, the fingers are more or less flexed at MCP, PIP and DIP joints. According to the size of the object, they are laterally rotated and inclined towards the ulnar side of the hand.
In non-power grip or otherwise, precision grip the thumb is held more perpendicular to the hand and moved into opposition, with limited flexion at the fingers. Examples of this type of grip are while writing, pinching, playing a piano, typing and in a long time computer users. In a pinch or prehensile grip, greater force is generated if the pulp of the thumb is placed against the pulps of the index and long fingers. The computer professional secure mouse gripped between thumb and fingers and is easily maneuvered by flexing the straight fingers and the thumb, and the hand is in a relaxed, untwisted, and in a natural upright position.
The hand is most commonly injured in almost one-third of industrial injuries and nearly two-third of the injuries result in permanent partial disability [5]. Thus, efforts taken at the primary level of prevention of disability to find the normal FFC for each individual, working in various job sectors, helps in regaining the ROM and restoring their hand functions. Hence, the aim of the study was to identify the range of values of FFC among individuals working with PGU and NPGU and to compare the FFC between the individuals with occupations involving power grip and individuals with non-power grip occupations and hence identify the minimal resting ROM values required for both the groups.
Materials and Methods
A cross-sectional study was conducted in a mixed population of 510 active individuals at manufacturing industrial and software companies, from 2014-2016. The names of the industries are withheld on privacy agreement. This study was approved by the Institutional Ethics Committee, Sri Ramachandra Institute of Higher Education and Research (IEC-NI/11/OCT/25/61).
The participants age ranged between 25 and 40 years and they belonged to various occupations like heavy equipment handling, industrial work and individuals working with software company.
Subjects who were active in occupational activities in power grip and non-power grip repetitive tasks and working with the same occupation for a minimum of three years were included in the study. Both male and female subjects between the age group of 25 years and 40 years participated in the study. This age variation was selected to include only the subjects active in their occupation and to exclude any medical illness that affect the hand and finger resting positions, which is a common scenario beyond 40 years of age [6,7]. Any congenital or acquired ailments of the hand, swelling of the wrist and digits, any recent or past trauma to an upper extremity, and pain at any part of the body with a Visual Analogue Scale (VAS) of 5 or above were excluded from the study.
The sample size was determined using a previous literature review based on the prevalence of hand injuries and non traumatic injuries like carpal tunnel syndrome affecting industrial workers and computer users worsening functional usage of the hand in everyday activities [8].
A written consent was obtained from the individuals participating in the study, explaining them about the procedure followed for recording the range of values of their hands and its uses.
After completing a questionnaire based on occupation, the subjects were grouped into PGU (Group I) and NPGU (Group II). A total 510 individuals were selected based on the prevalence rate of hand impairments among industrial and computer users. Two hundred and sixty subjects (GROUP I) working in a single heavy equipment manufacturing unit handling heavy machineries and heavy tools with repetitive task of lifting, loading and using drilling tools were chosen. Fork lifters, loaders and subjects handling tools like pneumatic drillers, spanners and hammers were included in the PGU group. Among them, 10 subjects were excluded from the study due to severe callosities and deformity in the hand. Two hundred and fifty subjects (GROUP II) working in software company were included in NPGU group.
The participants were positioned comfortably in a chair with their hand well supported and feet flat on the floor. Measurements of ROM of resting state of all the individual four digits of both the dominant and non-dominant hand were recorded using universal goniometer and composite finger flexion of all the four digits was measured using a ruler.
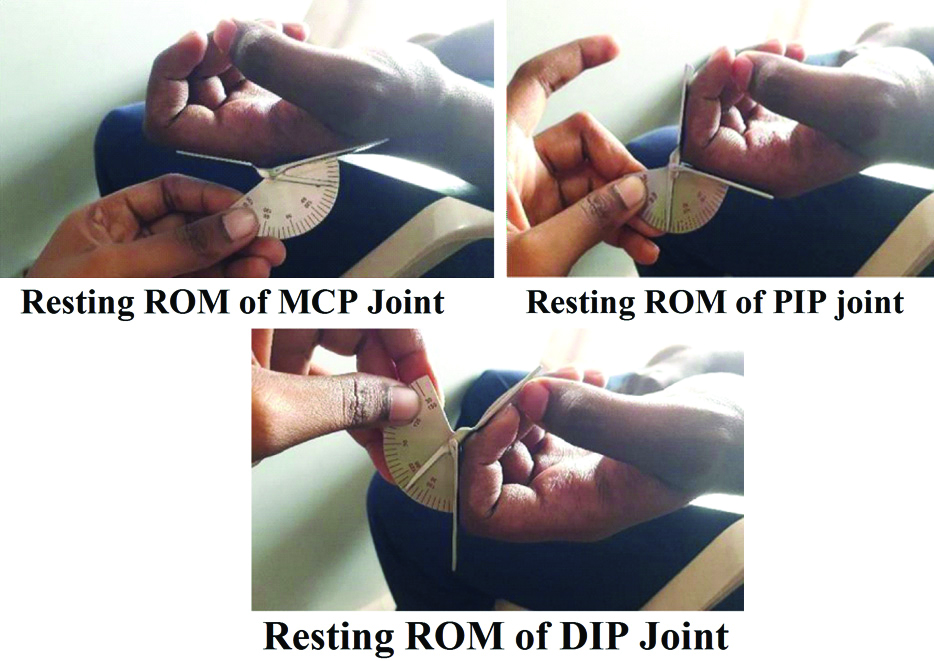
The ROM of MCP, PIP and DIP joints of the dominant hand was taken initially followed by measurements for the non-dominant hand. The dominant hand to be tested was positioned with shoulder adducted by the side of the body, forearm supinated, wrist in a functional position at 15-20° of extension and fingers, and placed at the edge of the body. The therapist sat adjacent to the subject and the readings were recorded. The participants were instructed not to move and to remain completely relaxed throughout the procedure. Finger goniometer was used to measure the flexion ROM of MCP joint of the index finger. The stable arm of the goniometer was placed parallel to the 2nd metacarpal bone, the midpoint of the goniometer was placed at the MCP joint and the movable arm was moved from zero degrees to a position where it lies parallel to the proximal phalanx and the readings were recorded as ROM of 2nd MCP joint. Next, the flexion ROM of the PIP joint of the same digit was measured with stable arm parallel to the 2nd proximal phalanx, the midpoint of goniometer at the PIP joint and the movable arm was moved from zero such that it lies parallel to the middle phalanx. The readings were recorded as flexion ROM of 2nd PIP joint. Subsequent flexion ROM of the DIP joint of the same digit was measured with stable arm parallel to the 2nd middle phalanx, the midpoint of goniometer at the DIP joint and the movable arm was moved from zero such that it lies parallel to the distal phalanx. The readings were recorded as flexion ROM of 2nd DIP joint. Similarly, flexion ROM of MCP, PIP and DIP joints of all other 3rd, 4th, and 5th digits were also recorded by the therapist. The positions of the MCP joints, PIP joints and DIP joints were recorded [Table/Fig-2].
Measuring resting rom of MCP joint, PIP joint and DIP joint using goniometer.
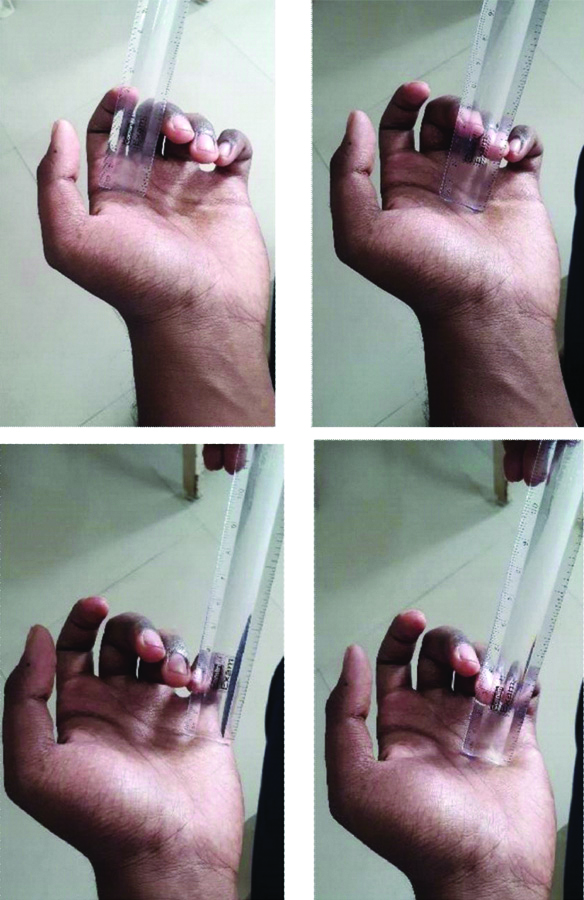
Composite finger flexion of all the four digits was measured for each hand using a geometric ruler. The position of the subject and the therapist was followed as the same as for goniometry measurement. A geometric ruler was placed perpendicular to the palm at the level of the distal palmar crease such that the end of the ruler marked 0 cm corresponded to the palmar crease and the marking on the ruler that corresponded to the tip of the index finger was noted down as 2nd digit. Similarly, the 3rd, 4th, and 5th digits were measured [Table/Fig-3].
Resting ROM measurement using numeric scale for index, middle, ring and little finger-composite finger flexion.
Outcome Measures
The primary outcome tool included measuring the resting ROM of Metacarpophalangeal (MCP), Proximal Interphalangeal (PIP) and Distal Interphalangeal (DIP) joints both dominant and non-dominant hand using goniometer. The secondary outcome measure was recorded using the composite finger flexion method, which assesses finger ROM, measured as the distance from the fingertip to a fixed point in the palm, using a ruler. The subject attempted to make a fist. Composite finger flexion is a quick, simple and cheap method and provides a measure which both therapist and patients can use as an indicator of progress. This measurement gives an approximation of the total digital motion in flexion and is more comprehensible to most individuals than motion measured in degrees. Centimeters were used to record the distance with zero indicating full flexion to the distal palmar crease [9,10].
Statistical Analysis
The demographic information of the participants is compared between power grip and non-power grip groups by descriptive statistics like mean and standard deviation in case of continuous data or frequency and percentage for categorical data. The ROM values and composite figure flexion values are summarised by mean and SD within each of power grip and non-power grip groups. The normal values for each of the sub categories are estimated by mean with its 95% confidence interval. The confidence intervals were compared across different sub categories. The pairwise mutually exclusive confidence intervals were considered to be significantly different form each other else insignificant statistically. The p-values from paired and unpaired t-test were also obtained in case of comparison of the features within and between the participants respectively. The results were visualised by error bars. The data was entered in excel and analysed by statistical software R version 3.5.1.
Unpaired t-test was used to compare the resting ROM values obtained using goniometric measurement and Composite Finger Flexion (CFF) values of all the four digits between PGU and NPGU.
Results
Group I consisted of 250 PGU and Group II consisted of 250 NPGU. [Table/Fig-4] shows baseline characteristics of age, work experience and number of male and female participants in both the groups. The mean age of both the groups was almost similar with 31.57±4.26 and 32.71±4.76, respectively. Both groups had participants with >5 years of work experience. There were more number of male participants in power grip group then that of non-power grip group.
Baseline characteristics of the study population.
| Variables | Occupation involving power grip | Occupation involving non-power grip | p-value |
|---|
| Age (mean±SD) | 31.57±4.26 | 32.71±4.76 | 0.005 |
| Age of male (years) | 31.97±4.37 | 33.24±4.69 |
| Age of female (years) | 30.08±3.45 | 31.08±4.62 |
| Number of male participants | 197 | 188 |
| Number of female participants | 53 | 62 |
| Average years of work of participants in occupation | 7±2 | 8±4 |
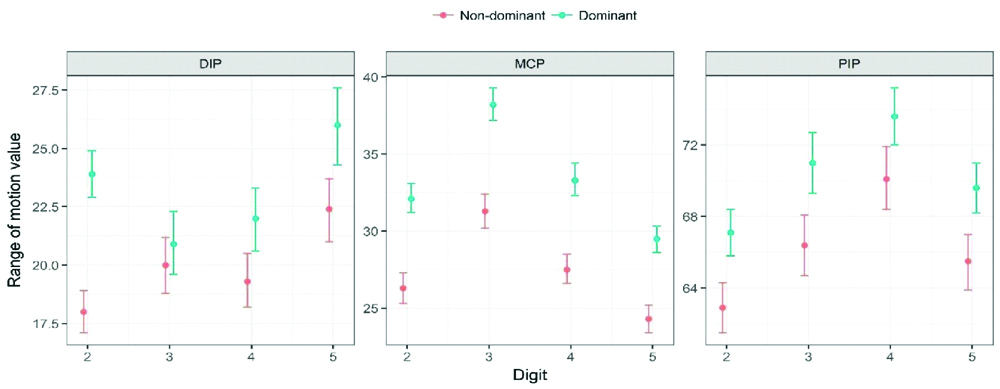
[Table/Fig-5,6] represents the resting ROM values of DIP, MCP, PIP joints of both dominant and non-dominant hand in power grip group. The dominant hand has an increased ROM values in all the above distal three joints than the non-dominant hand. In the DIP joint resting ROM values of 5th digit showed a higher value of 26° and 22° compared to other 3 digits, in both dominant and non-dominant hand, respectively. Similarly, in the MCP joint the resting ROM values of 3rd digit was 38° and 31° comparatively more than other 3 digits and in the PIP joint, the resting ROM values of the 4th digit was 73° and 70° and found to have higher value than other three digits in both dominant and non-dominant hand, respectively.
Range of motion values of finger flexion cascade in power grip users.
| Digit | Hand | DIP | MCP | PIP |
|---|
| | Mean±SD | 95% CI | Mean±SD | 95% CI | Mean±SD | 95% CI |
|---|
| 2nd | Non-dominant | 17.97±7.23 | 17.1, 18.9 | 26.29±7.75 | 25.3, 27.3 | 62.90±11.06 | 61.5, 64.3 |
| Dominant | 23.86±8.09 | 22.9, 24.9 | 32.14±7.36 | 31.2, 33.1 | 67.10±10.56 | 65.8, 68.4 |
| 3rd | Non-dominant | 20.02±9.82 | 18.8, 21.2 | 31.29±8.91 | 30.2, 32.4 | 66.39±13.60 | 64.7, 68.1 |
| Dominant | 20.95±11.02 | 19.6, 22.3 | 38.23±8.41 | 37.2, 39.3 | 71.02±13.63 | 68.4, 72.7 |
| 4th | Non-dominant | 19.32±9.18 | 18.2, 20.5 | 27.54±7.38 | 26.6, 28.5 | 70.11±14.13 | 68.4, 71.9 |
| Dominant | 21.96±10.89 | 20.6, 23.3 | 33.31±8.38 | 32.3, 34.4 | 73.62±12.93 | 72, 75.2 |
| 5th | Non-dominant | 22.35±11.16 | 21, 23.7 | 24.27±7.11 | 23.4, 25.2 | 65.46±12.26 | 63.9, 67 |
| Dominant | 25.98±13.35 | 25.3, 27.3 | 29.48±6.92 | 28.6, 30.3 | 69.62±11.38 | 68.2, 71 |
DIP: Distal interphalangeal joint; MCP: Metacarpo phalangeal joint; PIP: Proximal interphalangeal joint
Range of motion values of finger flexion cascade in power grip users (graph).
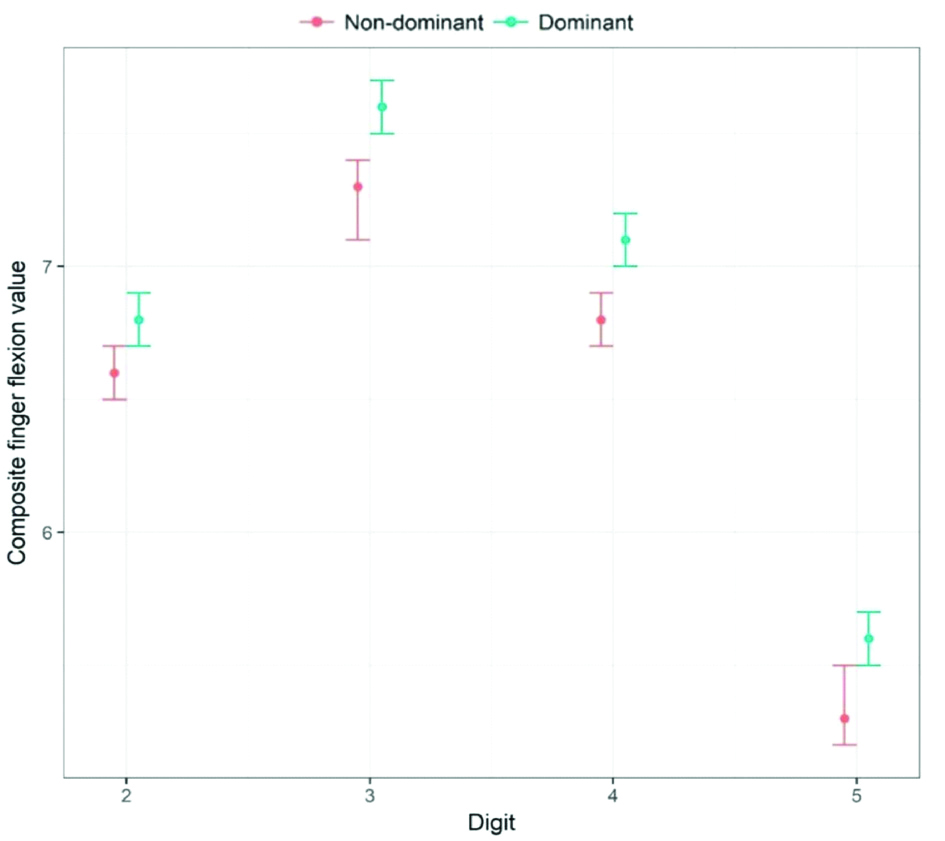
[Table/Fig-7,8] consist of CFF values of both dominant and non- dominant hand in power grip users. The CFF values of the dominant hand are more than the non-dominant hand. Among the CFF values of the lateral four digits, the 3rd digit in both the dominant and non-dominant hand is 7.61 cm and 7.26 cm, respectively and has a higher value compared to other digits.
The composite finger flexion values in the power grip users.
| Digit | Composite finger flexion values in power grip users |
|---|
| Dominant hand | Non-dominant hand |
|---|
| Mean±SD in cm | 95% CI | Mean±SD in cm | 95% CI |
|---|
| 2nd | 6.78±0.75 | 6.7, 6.9 | 6.63±0.70 | 6.5, 6.7 |
| 3rd | 7.61±0.99 | 7.5, 7.7 | 7.26±0.97 | 7.1, 7.4 |
| 4th | 7.07±0.97 | 7, 7.2 | 6.81±0.95 | 6.7, 6.9 |
| 5th | 5.57±0.87 | 5.5, 5.7 | 5.35±0.85 | 5.2, 5.4 |
The composite finger flexion values in the power grip users (graph).
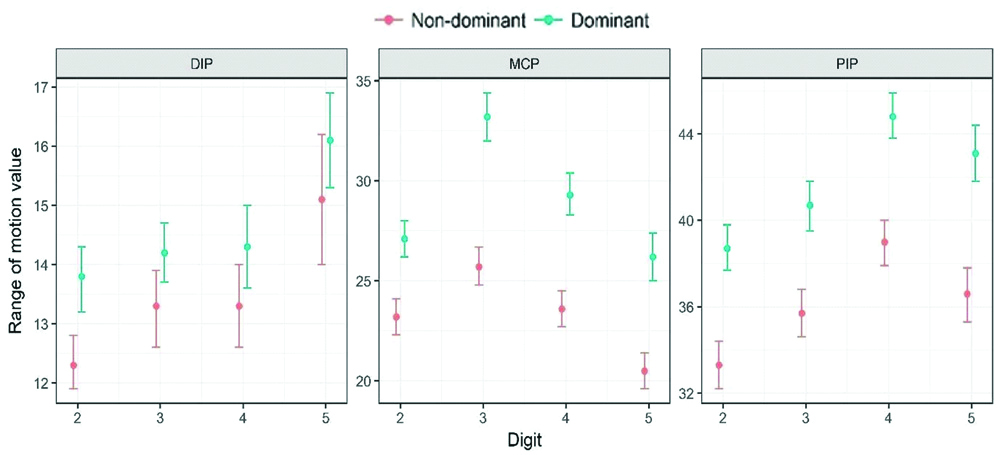
[Table/Fig-9,10] consist of resting ROM values of DIP, MCP, PIP joints of both dominant and non-dominant hand in non-power grip group. The dominant hand has an increased ROM values in all the above distal three joints than the non-dominant hand. In the DIP joint resting ROM values of 5th digit showed a higher value compared to other three digits, in both dominant and non-dominant hand. Similarly, in the MCP joint the resting ROM values of 3rd digit was comparatively more than other three digits and in the PIP joint, the resting ROM values of the 4th digit was found to have higher value than other three digits in both dominant and non-dominant hand.
Range of motion values of finger flexion cascade in non-power grip users.
| Digit | Hand | DIP | MCP | PIP |
|---|
| | Mean±SD | 95% CI | p-value | Mean±SD | 95% CI | p-value | Mean±SD | 95% CI | p-value |
|---|
| 2nd | Non-dominant | 12.34±3.56 | 11.9, 12.8 | <0.001 | 23.19±7.55 | 22.3, 24.1 | <0.001 | 33.31±9.13 | 32.2, 34.4 | <0.001 |
| Dominant | 13.76±4.65 | 13.2, 14.3 | 27.08±7.00 | 26.2, 28 | 38.74±8.74 | 37.7, 39.8 |
| 3rd | Non-dominant | 13.26±5.02. | 12.6, 13.9 | 0.010 | 25.75±7.77 | 24.8, 26.7 | <0.001 | 35.69±9.06 | 34.6, 36.8 | <0.001 |
| Dominant | 14.20±4.08 | 13.7, 14.7 | 33.21±9.43 | 32, 34.4 | 40.67±9.07 | 39.5, 41.8 |
| 4th | Non-dominant | 13.31±5.41 | 12.6, 14 | <0.001 | 23.64±7.17 | 22.7, 24.5 | <0.001 | 38.96±8.50 | 37.9, 40 | <0.001 |
| Dominant | 14.33±5.56 | 13.6, 15 | 29.34±8.65 | 28.3, 30.4 | 44.83±8.42 | 43.8, 45.9 |
| 5th | Non-dominant | 15.14±8.73 | 14, 16.2 | 0.066 | 20.51±7.48 | 19.6, 21.4 | <0.001 | 36.56±9.81 | 35.3, 37.8 | <0.001 |
| Dominant | 16.08±6.44 | 15.3, 16.9 | 26.24±9.67 | 25, 27.4 | 43.07±10.35 | 41.8, 44.4 |
Range of motion values of finger flexion cascade in non-power grip users (graph).
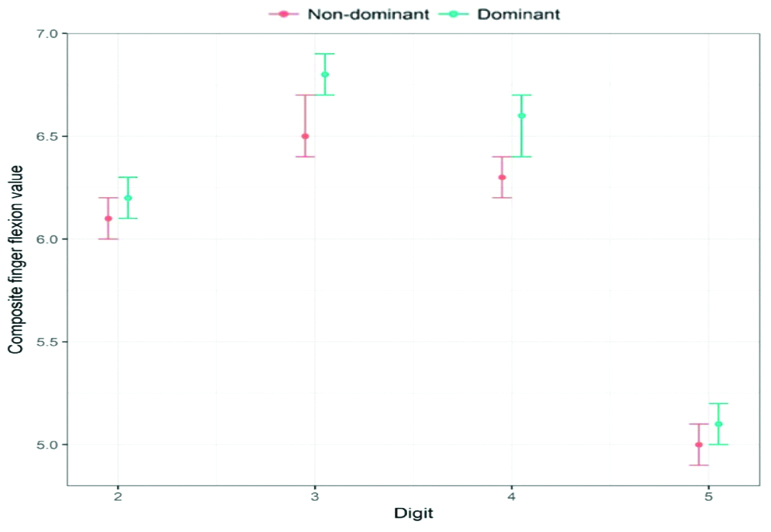
[Table/Fig-11,12] consist of CFF values of both dominant and non-dominant hand in non-power grip users. The CFF values of the dominant hand are more than the non-dominant hand. Among the CFF values of the lateral four digits, the 3rd digit in both the dominant and non-dominant hand has a higher value compared to other digits.
The composite finger flexion values in non-power grip users.
| Digit | Composite finger flexion values in Non-power grip users |
|---|
| Dominant hand | Non-dominant hand |
|---|
| Mean±SD | 95% CI | Mean±SD | 95% CI |
|---|
| 2nd | 6.19±0.91 | 6.1, 6.3 | 6.12±0.66 | 6, 6.2 |
| 3rd | 6.81±0.89 | 6.7, 6.9 | 6.55±0.87 | 6.4, 6.7 |
| 4th | 6.55±0.90 | 6.4, 6.7 | 6.29±0.92 | 6.2, 6.4 |
| 5th | 5.15±0.78 | 5, 5.2 | 4.98±0.85 | 4.9, 5.1 |
The composite finger flexion values in non- power grip users (graph).
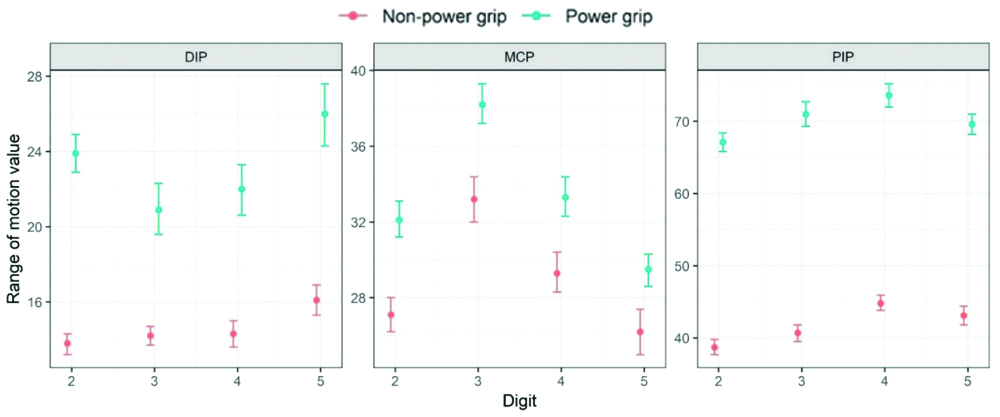
[Table/Fig-13,14] represents the comparison of ROM values between Group I and Group II in all the DIP, MCP and PIP joints of the dominant hand. The ROM of all the DIP, MCP and PIP joints in 2nd, 3rd, 4th and 5th digits of subjects in Group I was more than the ROM of all the DIP, MCP and PIP joints in 2nd, 3rd, 4th and 5th digits of subjects in Group II and was found to be statistically significant (p<0.001) compared to DIP, MCP and PIP joints ROM of subjects in Group II.
Comparison of ROM in dominant hand between power grip users and non-power grip users.
| Digit | Mean values | DIP | MCP | PIP | p-value |
|---|
| | PGU(Group I) | NPGU(Group II) | PGU(Group I) | NPGU(Group II) | PGU(Group I) | NPGU(Group II) |
|---|
| 2nd | Mean±SD | 23.86±8.09 | 13.76±4.65 | 32.14±7.36 | 27.08±7.00 | 67.10±10.56 | 38.74±8.74 | <0.001 |
| 95% CI | 22.9, 24.9 | 13.2, 14.3 | 31.2, 33.1 | 26.2, 28 | 65.8, 68.4 | 37.7, 39.8 |
| 3rd | Mean±SD | 20.95±11.02 | 14.20±4.08 | 38.23±8.41 | 33.21±9.43 | 71.02±13.63 | 40.67±9.07 | <0.001 |
| 95% CI | 19.6,22.3 | 13.7, 14.7 | 37.2, 39.3 | 32,34.4 | 68.4, 72.7 | 39.5, 41.8 |
| 4th | Mean±SD | 21.96±10.89 | 14.33±5.56 | 33.31±8.38 | 29.34±8.65 | 73.62±12.93 | 44.83±8.42 | <0.001 |
| 95% CI | 20.6, 23.3 | 13.6, 15 | 32.3, 34.4 | 28.3, 30.4 | 72, 75.2 | 43.8, 45.9 |
| 5th | Mean±SD | 25.98±13.35 | 16.08±6.44 | 29.48±6.92 | 26.24±9.67 | 69.62±11.38 | 43.07±10.35 | <0.001 |
| 95% CI | 25.3, 27.3 | 15.3, 16.9 | 28.6, 30.3 | 25, 27.4 | 68.2, 71 | 41.8, 44.4 |
DIP: Distal interphalangeal joint; MCP: Metacarpo phalangeal joint; PIP: Proximal interphalangeal joint
Comparison of ROM in dominant hand between power grip users and non-power grip users (graph).
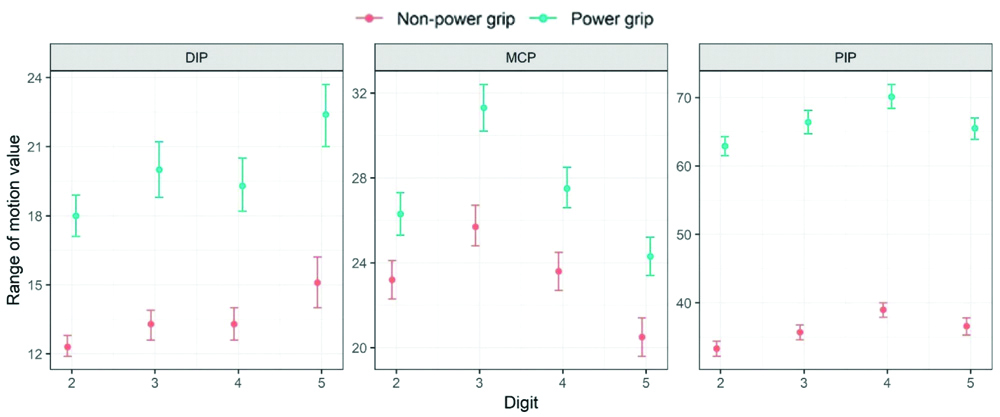
[Table/Fig-15,16] represents the comparison of ROM values between Group I and Group II in all the DIP, MCP and PIP joints of the non- dominant hand. The ROM of all the DIP, MCP and PIP joints in 2nd, 3rd, 4th and 5th digits of subjects in Group I was more than the ROM of all the DIP, MCP and PIP joints in 2nd, 3rd, 4th and 5th digits of subjects in Group II and was found to be statistically significant (p<0.001) compared to DIP, MCP and PIP joints ROM of subjects in Group II.
Comparison of rom in non-dominant hand between power grip users and non-power grip users.
| Digit | Mean values | DIP | MCP | | PIP |
|---|
| | PGU(Group I) | NPGU(Group II) | PGU(Group I) | NPGU(Group II) | PGU(Group I) | NPGU(Group II) | p-value |
|---|
| 2nd | Mean±SD | 17.97±7.23 | 12.34±3.56 | 26.29±7.75 | 23.19±7.55 | 62.90±11.06 | 33.31±9.13 | <0.001 |
| 95% CI | 17.1, 18.9 | 11.9, 12.8 | 25.3, 27.3 | 22.3, 24.1 | 61.5, 64.3 | 32.2, 34.4 |
| 3rd | Mean±SD | 20.02±9.82 | 13.26±5.02 | 31.29±8.91 | 25.75±7.77 | 66.39±13.60 | 35.69±9.06 | <0.001 |
| 95% CI | 18.8, 21.2 | 12.6, 13.9 | 30.2, 32.4 | 24.8, 26.7 | 64.7,68.1 | 34.6, 36.8 |
| 4th | Mean±SD | 19.32±9.18 | 13.31±5.4 | 27.54±7.38 | 23.64±7.17 | 70.11±14.13 | 38.96±8.50 | <0.001 |
| 95% CI | 18.2, 20.5 | 12.6, 14 | 26.6, 28.5 | 22.7, 24.5 | 68.4, 71.9 | 37.9, 40 |
| 5th | Mean±SD | 22.35±11.16 | 15.14±8.73 | 24.27±7.11 | 20.51±7.48 | 65.46±12.26 | 36.56±9.81 | <0.001 |
| 95% CI | 21, 23.7 | 14, 16.2 | 23.4, 25.2 | 19.6, 21.4 | 63.9, 67 | 35.3,37.8 |
PGU: Power grip users; NPGU: Non power grip users; DIP: Distal interphalangeal joint; MCP: Metacarpo phalangeal joint; PIP: Proximal interphalangeal joint
Comparison of ROM in dominant hand between power grip users and non-power grip users (graph).
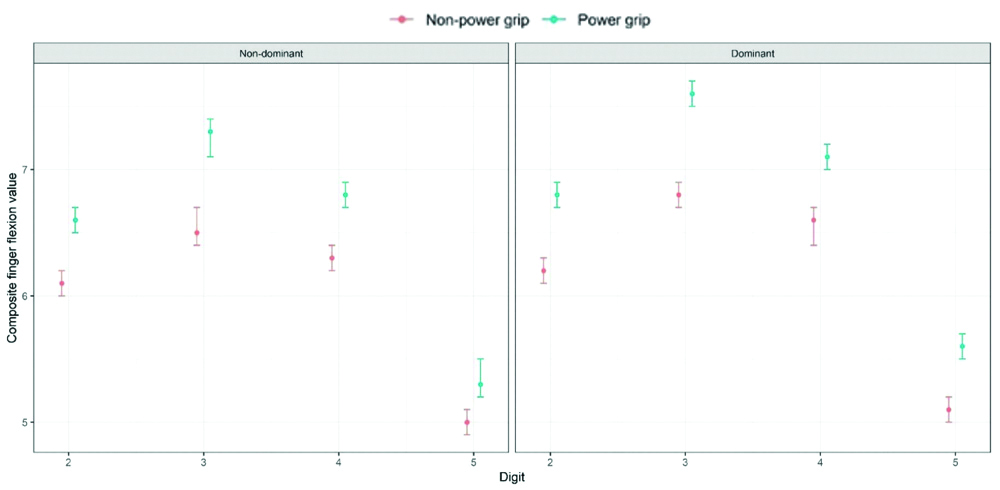
The [Table/Fig-17,18], represents the comparison of CFF of all the four digits of the subjects in Group I and Group II. The CFF values of both dominant and non-dominant hand was statistically significant (p<0.001) in all the four digits of subjects in Power grip group (Group I) than in Non- power grip group (Group II).
Comparison of composite finger flexion values between power grip users and non-power grip users in non-dominant and dominant hand.
| Digit | Non-dominant hand | Dominant hand |
|---|
| Power grip users | Non-power grip users | p-value | Power grip users | Non-power grip users | p-value |
|---|
| Mean±SD | Mean with 95% CI | Mean±SD | 95% CI | | Mean±SD | 95% CI | Mean±SD | 95% CI | |
|---|
| 2nd | 6.63±0.70 | 6.5, 6.7 | 6.12±0.66 | 6,6.2 | <0.001 | 6.78±0.75 | 6.7, 6.9 | 6.19±0.91 | 6.1,6.3 | <0.001 |
| 3rd | 7.26±0.97 | 7.1, 7.4 | 6.55±0.87 | 6.4, 6.7 | <0.001 | 7.61±0.99 | 7.5, 7.7 | 6.81±0.89 | 6.7, 6.9 | <0.001 |
| 4th | 6.81±0.95 | 6.7, 6.9 | 6.29±0.92 | 6.2, 6.4 | <0.001 | 7.07±0.97 | 7, 7.2 | 6.55±0.90 | 6.4, 6.7 | <0.001 |
| 5th | 5.35±0.85 | 5.2,5.5 | 4.98±0.85 | 4.9, 5.1 | <0.001 | 5.57±0.87 | 5.5, 5.7 | 5.15±0.78 | 5, 5.2 | <0.001 |
Comparison of composite finger flexion values between power grip users and non-power grip users in non-dominant and dominant hand (graph).
Discussion
The current study has proved that occupation has an influence on FFC as the fingers of the hand have to adapt to various requirements of grasp in PGU and NPGU.
In this study, the ROM observed explains that the ulnar side fingers contributed largely for gripping among PGU, such as DIP joint of the 5th digit and PIP joint of the 4th digit and MCP joint of the 3rd digit showed a higher value compared to other digits. A power grip requires a significant amount of force. In a most powerful grip, the fingers flex around an object in one direction and the thumb wraps around in the opposite direction providing counterforce to keep the object in contact with the palm and/or fingers. The fingers spread in abduction and are brought back together in adduction at the MCP joint.
Discussion on Normative Resting ROM Values in Power Grip Group
The participants in power grip group of the study showed higher resting ROM values in PIP joint than that of MCP and DIP joint in both dominant and non-dominant hand. The PIP joint of the 4th digit (ring finger) had a higher resting ROM value of 73° in dominant and 70° in non-dominant hand compared to other three digits. Among the ROM values, the PIP joint has higher resting ROM as the nature of the job demands prehensile grip of holding tools like hammer, drilling machine, holding cylindrical objects with diameter of 35 mm hand grip. A study done to find the ROM of finger joints using computer vision system, revealed that the required Active Range Of Motion (AROM) of PIP joint is 100° and that of MCP joint is 90o [11]. But as the focus of the present study was on the static resting ROM values (FFC) in both power grip and non-power grip users, it required only the least ROM values to rehabilitate the subjects to the pre-injury level than the required AROM values and also aids to modify the equipments to the data values found for ergonomic advantage.
A study done among 52 Rheumatoid arthritis patients found that actual impairment of flexion and extension in PIP and MCP joint are predictors of impairment in grasping abilities and fine manipulation of objects [12].
In the present study among all the MCP joints of all digits, only MCP joint of the 3rd digit showed a higher ROM of 38° in the dominant hand and 31° in non-dominant hand compared to other digits. As MCP joint is designed to increase the span of the hand and hence grasping of objects more than 35 mm hand grip is possible and contributes to functional ROM of hand. Collateral ligaments of MCP joints are lax in mild extension, which allows abduction of fingers and hence facilitates grasping of objects.
In the DIP joint resting ROM values of 5th digit showed a higher value of 26° and 22° compared to other three digits, in both dominant and non-dominant hand, respectively. Flexor power to the ulnar side of the hand is provided by the strong long flexors and supported at the MCP joint by the unipennate lumbricals. In a comparative study done among female 248 teachers and 295 dentist proved that teachers had grade 2 osteoarthritis of DIP joint than other distal joints of hand [13]. These values of resting ROM of the distal joints of hand may prove to be useful to the required ROM values needed for various occupations demanding power grip, as the fingers need to move and grip various tools in an industry. The shape, size and texture of the tools have a great influence on the power grip of the hand [14]. The measure of ROM deficits is useful in predicting the subjects actual hand functions [15].
In this study, the CFF values of the dominant hand was more than the non-dominant hand and was statistically significant (p<0.001). Among the CFF values of the lateral four digits, the 3rd digit (middle finger) in both the dominant and non-dominant hand has a higher value of 7.61cm and 7.26 cm, respectively and was comparatively more than other digits. As the subjects in the index study had more than 5 years of work experience, their nature of occupation consequently demands more flexion of fingers and hence influences the resting ROM values in PGU than among NPGU.
A study done on ergonomic values of normal hand functions, has mentioned that normative values evaluate the static position of joints of hand [16]. These resting ROM values are extremely effective in manufacturing equipments to the ergonomic resting ROM values found in this study which are less likely to cause cumulative trauma to hand, to formulate goals for hand rehabilitation after sustaining an injury, and in evaluating the prognosis to pre-injury level, instead of setting goals in achieving full functional requirements of hand which is time consuming.
Discussion on Normative Resting ROM Values in Non-Power Grip Group
The subjects included in this study in non-power grip group were software professionals, working with the continuous gripping activity of mouse and repetitive clicking. It involves both static and dynamic manipulation of the mouse. Dynamic mouse activity involves both moving and activating. Moving of the mouse consist of non-clicking and dragging, while activating the mouse consist of right click, left click and scrolling [17]. The job demands cylindrical gripping of the mouse which is more than 70 mm diameter.
In a study, on finger joint impedance during tapping on a computer, it was concluded that MCP joint caused flexion during clicking activities on keyswitch while DIP and PIP joints comparatively caused extension and absorbed energy. Kinematic movement at MCP joint does work on interphalangeal joints as well while working on keyswitch 18. Hence, the joint ROM of DIP, PIP and MCP joints are comparatively lesser than the PGU. In a study, conducted in Japan among 10 healthy men with no hand injuries, for measuring the flexion angles of the finger joints during cylindrical gripping of three different objects with 10 mm diameter, 60 mm and 120 mm, the angles were found to be decreasing as the diameter of the object increases [19].
When a two button mouse is used, continuous gripping causes muscular imbalance between flexors and extensors of the hand. Static, sustained holding causes finger lifting behaviour due prolonged extensor loading and avoiding fingers pressing against the buttons.
Clicking activity on mouse uses some of the smallest intrinsic muscles of the hand and word processing can easily require 3000 to 5000 clicking or pressing on the mouse per day. Hence muscle tension, causes muscles not only to consume more oxygen and produce more waste but also they slow or even arrested blood circulatory circumstances due to the constriction of blood vessels within the muscle when they contract for a prolonged period [20].
Discussion on Comparison Between Resting ROM Values PGU and NPGU
The resting ROM value of PIP joint is more than DIP and MCP joint as subjects in power grip were using equipments like spanner, repair tools and cylindrical equipments requiring powerful grip. But as the subjects in Group II were mostly software professionals, they required gripping of larger object than the PGU and hence the resting ROM values were found to be comparatively less in MCP and DIP joints than the PIP joints. As the size of the object increases, the ROM decreases. The associations were found to be statistically significant (p<0.001) when FFC was compared between the power grip and non-power grip in the dominant hand.
Though the little finger has the most passive, active and functional role in gripping activities, MCP joint passive extension is important for increasing the extent of the hand to grasp large objects [21].
Greater active extension is provided by the two extensor tendons (MCP extension), and bipennate lumbricals to index and middle finger and unipennate lumbricals to ring and little finger (interphalangeal joint extension). The mobility of the little finger is enhanced by the saddle shaped CMC joint which increases the mobility of the fifth ray and adds rotation, to allow opposition [22]. It permits the ulnar side of the hand to cup around an object like hammer, or extend when picking up a large cube or placing the hand flat on the table. The hypothenar musculature allows the mobile fifth ray to manipulate objects with precision and control. The increased mobility, dexterity and opposition enhance the function of the fifth ray and may represent the evolution of a “second thumb” [21]. From the study, even though significant difference (p<0.001) was found in all the distal joints of the hand between the non–dominant hand of subjects in group I and group II, greater difference was found in the resting ROM of the PIP joint. In a research done on analytical study of FFC in general, population of various occupations like electrical department, maintainenece department and medical record department. The electrical department showed greatest in PIP joint followed by MCP and DIP joint in the dominant hand. But PIP and DIP of non-dominant hand was more that the dominant hand [23]. In present study, the ROM values of all distal joints were more in the dominant hand than in the non-dominant hand.
The greatest resting ROM of the PIP joint of 4th digit in non-dominant hand is 70° among PGU and 38° in the NPGU. This increase may be contributed to the need for bilateral manipulation of tools using hands as non-dominant hand is used to hold the object in position (nails) and the dominant hand performs the action (hammers) demanding power grip when compared to that of using the non-dominant hand merely for keying purpose by non-power grip users.
Hence, an analysis of resting ROM of lateral four fingers of the hand in subjects of various occupations will be helpful to manufacture machineries and equipments according to the resting ROM values found in present study as they reduce the cumulative strain on joints of hand and to rehabilitate the individuals to their pre-injury level as they reflect on the functional ROM of the distal joints required to perform the activities of daily living, rather than focusing on the complete recovery of hand which is time consuming.
Limitation(s)
There was less number of female participants in the study. The female participants were included for comparative study between genders and to know how power grip and non-power grip differs with gender. Anthropometry of male and female body type has no role to play in FFC. But hand anthropometry on the length and breadth of hand, fingers and the circumference of finger varies between male and females. The study was not profession specific as it included subjects from different, non-identical professions. Few extraneous variables like hobbies such as biking, riding or gardening could be a limitation as it can have an influence on the FFC.
Conclusion(s)
The present study concludes that the normative values of the resting ROM values infer to the FFC measured at rest in both power grip and non-power grip users and there is an actual difference in the FFC between the individuals with occupation of power grips and individuals with the occupation of non-power grips. The data obtained in this study on normative resting values of MCP, PIP and DIP joints of required FFC for power grip and non-power grip groups may be beneficial in setting minimal ROM goals for patients with distal joint impairment and modify the tools as required for gripping of power grip and non-power grip equipments.
Further, scope of the study can be focused to analyse hand force required for various occupations and its effect on FFC. An analysis of diameter of various gripping tools and its effect on FFC, further implications on the effectiveness of FFC on rehabilitation of burns, stroke and rheumatoid arthritis patients, and the required functional ROM necessary for concerned modifications.
DIP: Distal interphalangeal joint; MCP: Metacarpo phalangeal joint; PIP: Proximal interphalangeal joint
DIP: Distal interphalangeal joint; MCP: Metacarpo phalangeal joint; PIP: Proximal interphalangeal joint
PGU: Power grip users; NPGU: Non power grip users; DIP: Distal interphalangeal joint; MCP: Metacarpo phalangeal joint; PIP: Proximal interphalangeal joint