Role of Diffusion Weighted Magnetic Resonance Imaging in Differentiating Benign From Malignant Thyroid Lesions: A Prospective Study
Kanika Bhargava1, Harneet Narula2, Amit Mittal3, Divya Sharma4, Kritesh Goel5, Divya Nijhawan6
1 Resident, Department of Radiology, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India.
2 Professor, Department of Radiology, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India.
3 Professor and Head, Department of Radiology, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India.
4 Resident, Department of Radiology, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India.
5 Resident, Department of Surgery, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India.
6 Resident, Department of Radiology, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Kanika Bhargava, Resident, Department of Radiology, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India.
E-mail: drkanika0809@gmail.com
Introduction
Accurate non-invasive imaging technique for characterising thyroid nodules has always been problematic. Diffusion-Weighted Magnetic Resonance Imaging (DW-MRI) is a functional MR imaging modality that quantifies the net diffusion of water molecules in any lesion. Thyroid carcinoma due to its increased cellularity shows diffusion restriction on DWI with low Apparent Diffusion Coefficient (ADC) values that can be used to differentiate benign and malignant thyroid nodules.
Aim
To evaluate role of DW-MRI in differentiating benign from malignant thyroid disease and to calculate ADC values of thyroid lesion/nodule on DW-MRI and correlate with FNAC/histopathology findings.
Materials and Methods
A prospective study was conducted in department of Radiodiagnosis, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala. Total of fifty patients with neck swelling diagnosed clinically and confirmed on ultrasound were included. The patients underwent routine as well diffusion weighted MRI using b-values of 0,400 and 800 mm2/sec. Their ADC values were calculated and were finally correlated with histopathological findings. Statistical analysis was done using SPSS v.21 and a p-value of <0.05 was considered as significant.
Results
The mean age of the patients was 41.8±13.9 years with maximum number of patients in the age group of 31 to 40 years. The mean ADC value of benign thyroid nodules (1.721×10-3mm2/sec) was significantly higher than that of malignant thyroid nodules (1.075×10-3mm2/sec) (p=0.01). The best cut-off value for distinguishing benign and malignant nodules was 1.371×10-3mm2/sec with sensitivity, specificity, PPV an NPV of 93.75%, 91.17%, 83.33% and 96.87%, respectively. The accuracy of the study in differentiating benign from malignant thyroid lesions was 92%.
Conclusion
DW-MRI due to its ability to probe the microstructure of the tumour, its short acquisition time, its high repeatability and safety is a new promising non-invasive imaging modality that can reliably differentiate between benign and malignant thyroid nodules and can help avoid unnecessary biopsies and consequently its hazards.
Apparent diffusion coefficient, b-value, Fine needle aspiration, Receiver operator characteristic curve
Introduction
The most common pathology of thyroid gland is thyroid nodules. There has been an increase in the incidence and prevalence of thyroid cancer [1-3]. The prevalence of thyroid disorders is 0.8% from total body malignancies. The prevalence is significantly higher in females than males and it was also higher in age group >31 years than age group <30 years [4]. USG is a sensitive and most common non-invasive diagnostic tool for thyroid lesions but there is still no reliable criteria to distinguish malignant and benign lesions and it is difficult to diagnose a malignant nodule if it is very large in size or is multinodular [5]. The use of colour doppler sonography to predict thyroid malignancy has given controversial results as some believe it to be helpful while others did not find it useful to improve diagnostic accuracy [5-8]. Fine Needle Aspiration (FNA) is considered as the diagnostic method of choice. However, the sensitivity of Fine Needle Aspiration Cytology (FNAC) is low due to factors like multiple nodules, experience of cytopathologist and indeterminate cytologic findings [9]. DWI is a non-invasive method with no risk of radiation which can differentiate benign and malignant lesions [10]. Benign or malignant lesion leads to microstructural changes in the tissue that produces different signals on DWI which can quantified by calculating ADC values.
Earlier, DW-MRI was mainly used for detection of cerebral ischemia in brain (hyperacute stage) but over the last two decades DW-MRI is now being used in other extracranial lesions [11,12]. Cancer is characterised by increased cellularity and hence shows restricted diffusion of water molecules. It has been seen that ADC is related to the cellular density of the tumours [11-13]. Most of the malignant tumours show reduced ADC due to high cellularity and reduced extravascular extracellular space [12]. Hence, ADC values calculation can distinguish malignant from benign thyroid nodules [13]. There is scarcity of literature in this field pertaining to Indian context [14]. Hence, the present study was carried out with an aim to determine the role of DW-MRI to diffferentiate between benign and malignant thyroid lesions and to analyse the ADC values from DW images and associate with Fine needle aspiration Cytology/histopathology.
Materials and Methods
A prospective study was carried out from September 2017 to July 2019 in Maharishi Markandeshwar Institute of Medical sciences and Research, Mullana (Ambala). Hence, taking the study pertaining to sample size calculation for sensitivity and specificity, a sample size was calculated to be 40 [15]. To compensate for any inadequacy in data during study it was rounded off to 50. The study was approved by the local Ethics Committee vide no. 1076 and informed consent of the participants was obtained before the assessment. A total of 50 patients (37 females and 13 males) in the age group of 12 to 65 years referred from medicine, surgery or ENT OPD with clinically palpable thyroid nodule/nodules confirmed on ultrasound were included and Thyroid lesions <1 cm, patients with cochlear implant, pacemaker, intraocular metallic foreign body, uncooperative patients, patients who are proven cases of thyroid malignancy and/or post-operative patients of neck surgery, patients who have diffuse enlargement of thyroid gland and patients with predominantly cystic component in the nodule were excluded from the study. A proper history was taken from all the patients. General and systemic examination was conducted thoroughly. Basic laboratory workup including complete blood count, chest x ray, thyroid function tests etc., was done.
MR scanning was performed with 1.5-T MR (Achieva, Philips Medical Systems, Netherland, B.V.) by using a standard head and neck coil. Localiser images was obtained in axial, coronal and sagittal planes followed by Conventional images including T2- weighted fast spin echo images (Repetition Time (TR)=3725 ms, Echo Time (TE)=80 ms) in axial and coronal planes, section thickness of 3 mm to 4 mm and intersection gap of 0.4 mm. Diffusion weighted MR images was obtained in axial plane with the parameters of Field of View (FOV)=250 mm, TR=3500 ms, TE=70 ms and 3 to 4 mm of slice thickness and 1 mm of intersection gap. A single shot echo-planar DW image was acquired using b-values (0, 400, 800) the diffusion sensitising gradient was applied in all three orthogonal planes (X,Y,Z) and Apparent Diffusion Coefficient (ADC) maps was automatically generated. ADC values were extracted from the ADC maps and were recorded.
A pilot project was conducted on a team of five radiologists who evaluated the DW images and calculated ADC values for a sample of 10 patients (who were not part of current study). The findings of the radiologists were scrutinized and unpaired t-test was applied to see the consensus among a pair of radiologists. The two radiologists who showed closest mean values and insignificant results on applying unpaired t-test were asked to participate in the study. These two experienced radiologists who were blind to the study independently, evaluated different set of DW images and calculated a single set of ADC value which was later correlated with FNAC/histopathological findings.
Statistical Analysis
Quantitative analysis was done using SPSS version 21. Diagnostic test sensitivity and specificity was obtained. Receiver Operating Characteristic (ROC) analysis curve was performed. A p-value <0.05 was considered significant.
Results
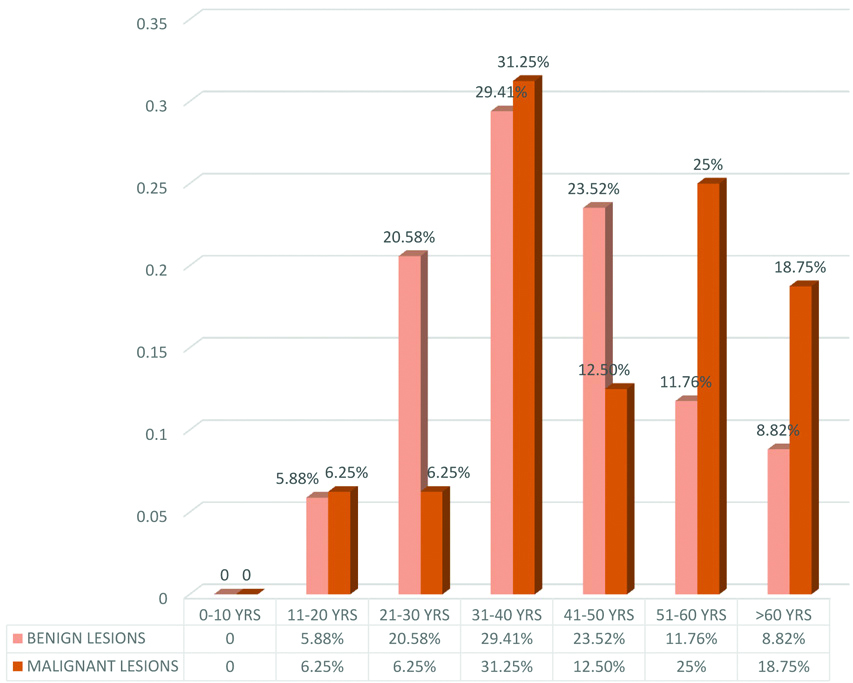
Majority of patients were females 37 (74%) and only 13 (26%) patients were males. Most of the patients were in the age group of 31-40 years at presentation which were 15 (30% of the total cases). The youngest and oldest age at presentation was 12 years and 65 years, respectively. Mean age was 41.8±13.9 years (Range: 12-65 years) [Table/Fig-1]. Out of 50 patients in our study, 18 patients showed diffusion restriction on DWI and ADC value of less than 1.371×10-3mm2/sec (cut-off value) and 32 patients showed no restriction on DWI and ADC value of more than 1.371×10-3mm2/sec.
Bar diagram showing age wise distribution of benign and malignant thyroid lesions.
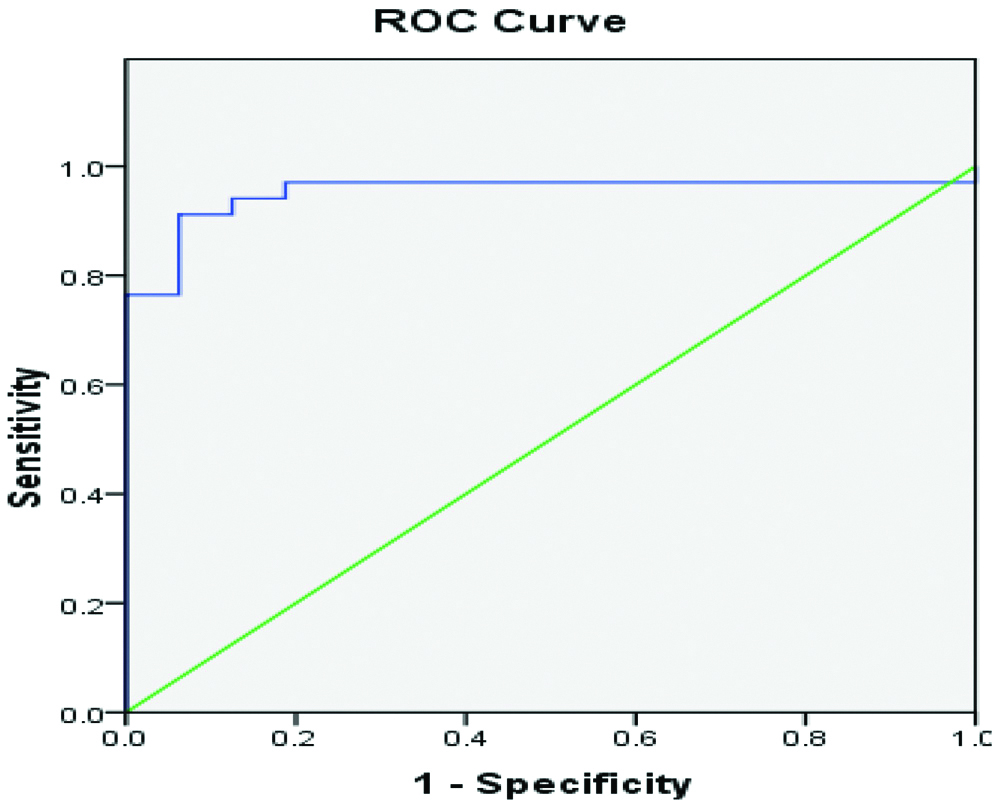
In final cytological/histopathological diagnosis of 50 patients, 34 patients had benign thyroid nodules and 16 patients had malignant thyroid nodules. Out of malignant thyroid nodules seven were papillary thyroid neoplasm, 3 were follicular neoplasm, three were medullary thyroid neoplasm, two were hurthle cell carcinoma and 1 was B-cell lymphoma of thyroid [Table/Fig-2]. On comparing with histopathological diagnosis, Out of 18 malignant lesions on DWI and ADC 15 were correctly diagnosed as malignant and three lesions were wrongly diagnosed which were benign on histopathology. And out of 32 benign lesions on DWI and ADC, 31 were correctly diagnosed as benign whereas one lesion was wrongly diagnosed which was malignant on histopathology. In present study of 50 patients, 34 patients had benign thyroid nodules on FNAC/Histopathological results with ADC value in the range of 0.602×10-3 mm2/sec to 2.408×10-3 mm2/sec with mean ADC value of 1.721±0.34×10-3 mm2/sec [Table/Fig-3]. Out of 16 malignant nodules with ADC value in the range of 0.842×10-3 mm2/sec to 1.512×10-3 mm2/sec with mean ADC value was 1.075±0.197×10-3 mm2/sec [Table/Fig-4]. The p-value of DWI for differentiating between benign and malignant lesions was 0.001. The calculated p-value was statistically significant and was less than 0.05 (Benign versus Malignant) [Table/Fig-5]. The ADC value of 1.371×10-3mm2/sec was used as a cut-off value for differentiation of benign from malignant thyroid nodules with a sensitivity of 93.75% and specificity of 91.17%, respectively [Table/Fig-6,7].
Distribution according to histopathological/cytlogical diagnosis.
| Final diagnosis | No. of Cases | % of Cases |
|---|
| Colloid Goitre | 19 | 38% |
| Adenomatous Nodule | 7 | 14% |
| Follicular Nodule | 4 | 8% |
| Hyperplastic Nodule | 3 | 6% |
| Hurthle Cell Adenoma | 1 | 2% |
| Papillary CA | 7 | 14% |
| Follicular CA | 3 | 6% |
| Medullary CA | 3 | 6% |
| Hurthle Cell CA | 2 | 4% |
| B-Cell Lymphoma | 1 | 2% |
| Total | 50 | 100% |
a) Axial T2W image showing a large heterogeneously hyperintense lesion in right lobe of thyroid. Another small hyperintense lesion is seen within the right lobe of thyroid. b) DWI showing high signal within the lesion on right side c) ADC map showing high signal with an ADC value of 2.016 x 10-3mm2/sec which was benign on MRI and proved to be multinodular goitre.

a) Coronal T2W MRI shows hyperintense signal in the region of thyroid nodules on both sides.b) DW image shows hyperintense signal in both the lesions of thyroid. c) The lesion shows an area of low signal on ADC map with an ADC value of 1.13 x 10-3mm2/sec, which was malignant on MRI and proved to be follicular carcinoma of thyroid on HPE.

Correlation of ADC values on DWI with FNAC/HPE diagnosis.
| Final diagnosis | N | Mean (x 10-3 mm2/sec) | Std. deviation | 95% Confidence Interval for Mean | Minimum (x 10-3 mm2/sec) | Maximum (x 10-3 mm2/sec) | p-value |
|---|
| Lower bound | Upper bound |
|---|
| Benign | 34 | 1.721 | 0.341 | 1.602 | 1.84 | 0.602 | 2.408 | 0.001 |
| Malignant | 16 | 1.075 | 0.197 | 0.971 | 1.181 | 0.842 | 1.512 |
| Total | 50 | 1.515 | 0.427 | 1.393 | 1.636 | 0.602 | 2.408 |
Receiver Operator Characterstic (ROC) curve of ADC value for discrimination between benign and malignant thyroid nodules.
Depicts the sensitivity, specificity, PPV, NPV and the accuracy of the study.
| FNAC-Malignant | FNAC-Benign |
|---|
| DWI-Malignant | 15 (a) | 3 (b) |
| DWI-Benign | 1 (c) | 31 (d) |
| Sensitivity=a÷(a+c)×100=15/16×100=93.75% |
| Specificity=d÷(d+b)×100=31/34×100=91.17% |
| PPV= a÷(a+b)×100=15/18×100=83.33% |
| NPV=d÷(c+d)×100=31/32=96.87% |
| Accuracy=(a+ d)÷(a+b+c+d)×100=46/50=92% |
Discussion
In present study, DWI was performed using b-values of 0, 400 and 800 mm2/sec and a high quality image was obtained. ADC values of thyroid lesions were calculated. Mean ADC value for benign lesions was 1.721×10-3 mm2/sec and the mean ADC value of malignant lesions was 1.075×10-3 mm2/sec respectively. There was a significant difference observed in the mean ADC value of benign and malignant thyroid nodules (p=0.001). Razek AA et al., performed DWI in thyroid nodules and calculated the ADC values. There was a significant difference observed in the mean ADC value of benign lesions (1.8×10-3 mm2/sec) from mean ADC value of malignant lesions (0.73 10-3 mm2/sec) [16]. Erdem G et al., reported using b- values of 0 and 1000 mm2/sec with mean ADC value of benign lesions as 2.743×10-3 mm2/sec and mean ADC value of malignant lesion as 0.695×10-3 mm2/sec [17]. Wu Y et al., used b-values of 0 and 300 and reported the mean ADC value of benign lesions as 2.37×10-3 mm2/sec, which was significantly higher than that of malignant lesions (1.49×10-3 mm2/sec) [18]. Abd el Aziz LM et al., reported a significant difference in the ADC values of benign and malignant lesions using b-value of 300 mm2/sec. DWI was done using b-values of 0, 300, 500 and 800 mm2/sec however, no significant difference was found using b-values of 500 and 800 mm2/sec [19]. Khizar AT et al., conducted study on 35 patients and calculated the mean ADC value in benign lesions as 1.93×10-3 mm2/sec, which was significantly higher than mean ADC values of malignant lesions as 0.94×10-3 mm2/sec [20]. Wang H et al., conducted a study on a large group of patients with 148 benign thyroid nodules and 111 malignant thyroid nodules and reported that the ADC values in benign lesions (1.95×10-3 mm2/sec) was significantly higher than ADC values in malignant lesions (1.26×10-3 mm2/sec) using b-value of 0 and 800 mm2/sec [21]. Aghaghazvini L et al., conducted a study using b-values of 50, 500 and 1000 mm2/sec. The mean ADC value in benign nodules was 1.94±0.54×10-3 mm2/sec and in malignant nodule was 0.89±0.29×10-3 mm2/s with p-value <0.005. Cut-off value of ADC was set to 1×10-3 mm2/s [22]. El-Hariri MA et al., also reported a significant difference between mean ADC of benign (1.85×10-3 mm2/sec) and malignant (0.89×10-3 mm2/sec) thyroid lesions using b-values of 0 and 500 mm2/sec [23]. There is variation in the cut-off values for the prediction of thyroid carcinomas in different studies and the exact cut-off value should be determined for each MR unit because of variations in the coils, pulse sequences and the MR imaging system [24].
Accurate pre-operative diagnosis of thyroid nodules would improve the surgical planning and reduce unnecessary operation. Therefore, there is a need to inculcate a new non-invasive and reliable radiographic modality that can distinguish between benign and malignant thyroid nodules.
Limitation(s)
Firstly, the study was carried in a small number of cases and needs to be expanded further to a larger population. Secondly, nodules less then 1 cm were not included in the study and improvements in the software of diffusion weighted MR studies will help in detection of smaller lesions in the future.
Conclusion(s)
DW-MRI is an easy, non-invasive and rapid technique that does not require i.v contrast administration and can be used for characterising the thyroid nodules. ADC values can be calculated which reliably differentiates benign from malignant thyroid lesions although it does not help to differentiate among the types of malignant thyroid nodules.
Author Declaration:
Financial or Other Competing Interests: None
Was Ethics Committee Approval obtained for this study? Yes
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Dec 13, 2019
Manual Googling: Feb 04, 2020
iThenticate Software: Mar 26, 2020 (16%)
[1]. Wong CK, Wheeler MH, Thyroid nodules: Rational managementWorld J Surg 2000 24(8):934-41.10.1007/s00268001017510865037 [Google Scholar] [CrossRef] [PubMed]
[2]. Brander A, Viikinkoski P, Nickels J, Kivisaari L, Thyroid gland: US screening in a random adult populationRadiology 1991 181(3):683-87.10.1148/radiology.181.3.19470821947082 [Google Scholar] [CrossRef] [PubMed]
[3]. Davies L, Welch HG, Increasing incidence of thyroid cancer in United states 1973-2002JAMA 2006 295(18):2164-67.10.1001/jama.295.18.216416684987 [Google Scholar] [CrossRef] [PubMed]
[4]. Nagarkar R, Roy S, Akheel M, Palwe V, Kulkarni N, Pandit P, Incidence of thyroid disorders in India: An institutional retrospective analysisInt J Dent Med Spec 2015 2(2):19-23.10.5958/2394-4196.2015.00012.6 [Google Scholar] [CrossRef]
[5]. Solbiati L, Osti V, Cova L, Tonolini M, Ultrasound of thyroid, parathyroid glands and neck lymph nodesEur Radiol 2001 11(12):2411-24.10.1007/s00330-001-1163-711734934 [Google Scholar] [CrossRef] [PubMed]
[6]. Frates MC, Benson CB, Charboneau J, Cibas ES, Clark OH, Coleman BG, Management of thyroid nodules detected at US: Society of Radiologists in Ultrasound consensus conference statementRadiology 2005 237(3):794-800.10.1148/radiol.237305022016304103 [Google Scholar] [CrossRef] [PubMed]
[7]. Gritzmann N, Koishwitz D, Retterbacher T, Sonography of thyroid and parathyroid glandsRadiol Clin North Am 2000 38(5):1131-45.10.1016/S0033-8389(05)70225-6 [Google Scholar] [CrossRef]
[8]. Papini E, Guglielmi R, Bianchini A, Crescenzi A, Taccogna S, Nardi F, Risk of malignancy in non-palpable thyroid nodules: Predictive value of ultrasound and colour doppler featuresJ Clin Endocrinol Metab 2002 87(5):1941-46.10.1210/jcem.87.5.850411994321 [Google Scholar] [CrossRef] [PubMed]
[9]. Pincot SN, Al-Wagih H, Schaerfer S, Cippel R, Chen H, Accuracy of fine needle aspiration biopsy for predicting neoplasm or carcinoma in thyroid nodules 4 cm or largerArch Surg 2009 144(7):649-55.10.1001/archsurg.2009.11619620545 [Google Scholar] [CrossRef] [PubMed]
[10]. Huang W, Roche P, Button T, ShindoIn M, In vivo 1H MR spectroscopic study of thyroid lesions: Correlation with pathologyBook of abstracts: 10th annual meeting of international society 2002 10:570 [Google Scholar]
[11]. Uhl M, Altehoefer C, Kontny U, Ilyasov K, Buchert M, Langer M, MRI diffusion imaging of neuroblastomas: First results and correlation to histopathologyEur Radiol 2002 12(9):2335-38.10.1007/s00330-002-1310-912195491 [Google Scholar] [CrossRef] [PubMed]
[12]. Lyng H, Haraldseth O, Rofstad EK, Measurement of cell density and necrotic fraction in human melanoma xenografts by diffusion weighted magnetic resonance imagingMagn Reson Med 2000 43(6):828-36.10.1002/1522-2594(200006)43:6<828::AID-MRM8>3.0.CO;2-P [Google Scholar] [CrossRef]
[13]. Bujang MA, Adnan TH, Requirements of minimal sample size for sensitivity and specificity analysisJCDR 2016 10(10):YE01-06.10.7860/JCDR/2016/18129.874427891446 [Google Scholar] [CrossRef] [PubMed]
[14]. Ravikanth R, Selvam RP, Pinto DS, Role of quantitative diffusion-weighted magnetic resonance imaging in differentiating benign and malignant thyroid lesionsJ Curr Res Sci Med 2017 3(3):131-33.10.4103/jcrsm.jcrsm_34_17 [Google Scholar] [CrossRef]
[15]. Gupta RK, Cloughesy TF, Sinha U, Garakian J, Lazareff J, Rubino G, Relationships between choline magnetic spectroscopy, apparent diffusion coefficient and quantitive histopathology in human gliomaJ Neurooncol 2000 50(3):215-26.10.1023/A:100643112003111263501 [Google Scholar] [CrossRef] [PubMed]
[16]. Razek AA, Sadek AG, Kombar OR, Elmahdy TE, Nada N, Role of apparent diffusion co-efficient values in differentiation between malignant and benign solitary thyroid nodulesAm J Neuroradiol 2008 29(3):563-68.10.3174/ajnr.A084918039755 [Google Scholar] [CrossRef] [PubMed]
[17]. Erdem G, Erdem T, Karakas HM, Mutlu DY, Firat AK, Sahin I, Diffusion weighted images differentiate benign from malignant thyroid nodulesJ Magn Reson Imaging 2010 31(1):94-100.10.1002/jmri.2200020027577 [Google Scholar] [CrossRef] [PubMed]
[18]. Wu Y, Yue X, Sen W, Du Y, Yuan Y, Tao X, Diagnostic value of diffusion-weighted MR imaging in thyroid disease: Application in differentiating benign from malignant diseaseBMC Medical Imaging 2013 13:2310.1186/1471-2342-13-2323899414 [Google Scholar] [CrossRef] [PubMed]
[19]. Abd el Aziz LM, Hamisa M, Badwy ME, Differentiation of thyroid nodules using diffusion-weighted MRIAlex J Med 2015 51(4):305-09.10.1016/j.ajme.2014.09.003 [Google Scholar] [CrossRef]
[20]. Khizer AT, Raza S, Slehria AU, Diffusion-weighted MR imaging and ADC mapping in differentiating benign from malignant thyroid nodulesJ Coll Physicians Surg Pak 2015 25(11):785-88. [Google Scholar]
[21]. Wang H, Wei R, Liu W, Chen Y, Song B, Diagnostic efficacy of multiple MRI parameters in differentiating benign vs malignant thyroid nodulesBMC Medical Imaging 2018 18(1):5010.1186/s12880-018-0294-030509198 [Google Scholar] [CrossRef] [PubMed]
[22]. Aghaghazvini L, Sharifian H, Yazdani M, Hosseeiny M, Kooraki S, Pirouzi P, Differentiation between benign and malignant thyroid nodules using diffusion-weighted imaging, a 3-T MRI studyIndian J Radiol Imaging 2018 28(4):460-64.10.4103/ijri.IJRI_488_1730662211 [Google Scholar] [CrossRef] [PubMed]
[23]. El-Hariri MA, Gouhar GK, Said NS, Riad MM, Role of diffusion-weighted imaging with ADC mapping and in vivo 1H-MR spectroscopy in thyroid nodulesEgypt J Radiol Nucl Med 2012 43(2):183-92.10.1016/j.ejrnm.2012.01.007 [Google Scholar] [CrossRef]
[24]. Schueller-Weidekamm C, Kaserer K, Schueller G, Scheuba C, Ringl H, Weber M, Can quantitative diffusion-weighted MR imaging differentiate benign and malignant cold thyroid nodules? Initial results in 25 patientsAm J Neuro Radiol 2009 30(2):417-22.10.3174/ajnr.A133818945798 [Google Scholar] [CrossRef] [PubMed]