Endodontic Management of Mandibular Second Premolar with Type-III Vertucci: A Rare Case
Neelam Mittal1, Tarun Kumar2, Vijay Parashar3
1 Dean and Head, Department of Conservative and Endodontics, Faculty of Dental Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India.
2 Academic Junior Resident, Department of Conservative and Endodontics, Faculty of Dental Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India.
3 Senior Resident, Department of Conservative and Endodontics, Faculty of Dental Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Tarun Kumar, Faculty of Dental Sciences, BHU, Varanasi, Uttar Pradesh, India.
E-mail: dentarunkumar@gmail.com
This case report describes endodontic management of mandibular second premolar with type-III Vertucci root canal configuration, in a 42-year-old female patient. She reported to the department for root canal treatment intended for prosthetic purpose. Vertucci type-III configuration (one common canal in coronal part, two distinct canals in the middle third of root which ended with a common apex) has been reported less worldwide; in range of 1.5%-6.66% only. Clinical examination revealed access opening which was restored with Zinc Oxide Eugenol (ZnOE). Radiographs showed minimal periapical changes, no widening of periodontal ligament space and lamina dura was intact. Clinician should have thorough knowledge of the pulp canal system so that an effective treatment can be provided.
Anatomical variations, Endo explorer david green, Magnification, Tactile examination
Case Report
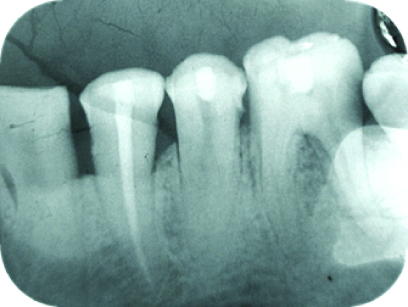
A 42-year-old female patient was referred from Department of Prosthodontics for intentional root canal treatment, to the Department of Conservative and Endodontics, with a purpose for fabrication of prosthesis under full mouth rehabilitation. After careful clinical examination, the patient had access opening which was restored with ZnOE in 44,45. The radiograph in relation of 44,45 [Table/Fig-1] revealed minimal periradicular changes, with intact lamina dura and normal PDL space. History of root canal in 44,45 was there, from the conservative and endodontics department three weeks before, by undergraduate student and was restored temporarily. Patient had persistent pain, which was mild and continuous in nature with respect to 45. Tooth no.44 was completely asymptomatic so, obturation was done and restored.
Pre-op IOPA of tooth no. 45.
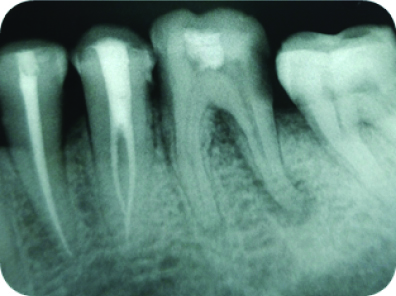
In the first visit, under local anaesthesia (Lignox 2%; Indoco Remedies Ltd., Mumbai) and rubber dam isolation (GDC Titanium Coated Clamps; Vasa Denticity Pvt., Ltd.,), root canal treatment was initiated in 45. With the help of an endo-access point (type FG-1; Dentsply, USA), temporary ZnOE was removed and access cavity was modified using Endozed bur (Tungsten Carbide Burs; Dentsply, USA). A single root canal orifice was located initially. As evident radiographically, the sudden disappearance of main canal obvious to suspect extra canals. Initially main canal was made it, which was found to be directed bucally. After careful re-negotiation of canal under ×3.5 magnification loupe and DG-16, (DG-16 Endo Probe, Densply; USA) one catch was found in slight distolingual direction, which was later confirmed with #10 no. k file (M Access K files, Dentsply; Switzerland). The tentative working length was determined to be 21 mm with an apex locator, (CanalPro Apex Locator, coltene; USA) which was further confirmed with IOPA [Table/Fig-2].

After establishing glide path with size #10 and #15 k-file, using crown-down technique, biomechanical preparation was done using rotary instruments with 06 #25 in buccal canal and 04 #25 in lingual canal (AF Blue S one file, Fanta Dental; Shanghai). Copious saline and sodium hypochlorite (3%) irrigation (Parcan; Septodont) was done during each instrumentation change.
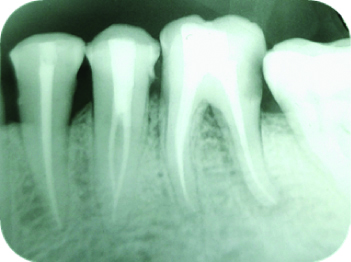
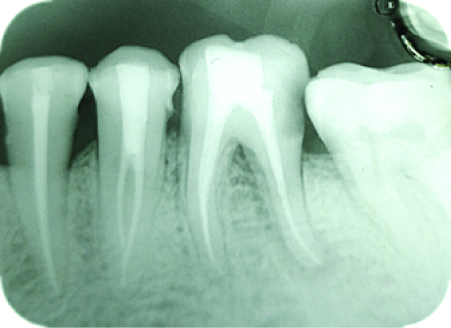
After drying canals with paper points, Calcium hydroxide (RC-Cal; Prime Dental Ltd., India) was placed as an intracanal medicament. The access cavity was temporary restored with ZnOE (Cavitemp, Ammdent; India) and a second visit was scheduled for further management. At scheduled second visit, patient was completely asymptomatic. Looking into anatomy of root canal, the obturation of both root canals was carried out using single cone technique with 06/25 and 04/25 gutta percha respectively, sealapex (kerr; Sybron endo) used as root canal sealer, in buccal and lingual canals [Table/Fig-3]. The follow-up review radiograph after 3 months [Table/Fig-4] and 6 months [Table/Fig-5] revealed no periapical changes, and the patient was totally asymptomatic.
IOPA after final obturation and restoration.
Discussion
Mandibular premolars are known for their unusual anatomy and considered as an enigma to the endodontist. Various root canal configurations have been studied and evaluated. Weine and Vertucci were the earliest to report clinical classifications of more than one canal system in a single root [1]. Understanding of root canal pattern with their disparity is important for successful non-surgical root canal treatment. Hence, it is recommended that clinicians should consider a thorough assessment of radiographs under different angulations [1].
Development of root and root canal system mainly depends upon Hertwig Epithelial Root Sheath (HERS). Extension of HERS grows as a single collar-shaped diaphragm that gives rise to single-rooted tooth or multiple tongue-like extensions that gives rise to multiple rooted tooth. The factors like ethnical background, gender and age of the population are responsible for the variations in root canal anatomy [2]. Vertucci (1978) reported that mandibular premolars have Type I canal in 70% of the cases, Type II canal in 4% of the cases, Type III canal in 1.5 % of the cases and Type 1V canal [3,4] in 24% of the cases [5]. Vertucci type-III configuration has been reported less by various authors in range of 1.5%-6.66% only [6].
Various Studies have shown the summary of Vertucci classification [Table/Fig-6] [4,6-9]. It was also observed that broad, flat roots are much more likely to contain multiple canals and intercanal ramifications [10]. While the main canal divide into two or more smaller canals that are not apparent on a radiograph, In order to rule out extra root and root canal, pre-operative as well as intra-operative radiographs with different angulations are very helpful [11]. For finding the split canal, important step was tactile examination of main canal with, precurved K-file tip. Once canal were located, access opening was modified for root canal preparation. Initially root canal was prepared with hand files up to size#20 and then finished with rotary file systems [12].
Summary of percentage of vertucci classification by different authors [4,6-9].
| Refrences | Percentage of vertucci classification |
|---|
| I | II | III | IV | V | VI | VII | VIII | IX |
|---|
| Chalil NM et al., [4] | 70 | 4 | 1.5 | 24 | | | | | |
| Singh S and Pawar M, [9] | 66 | 30 | | | 4 | | | | |
| Parekh V et al., [6] | 80 | | | 2.5 | 17.5 | | | | |
| Banga KS et al., [7] | 66.68 | 20 | 6.66 | | | | | | |
| Lyer VH et al., [8] | 75.4 | 1.0 | | 20.8 | 2.4 | | | 0.4 | |
The buccal canal that was in line with the core channel is frequently open to sufficient enlargement and obturation trial but the preparation and filling of the lingual canal is complicated. If the pulp chamber does not lie in its expected buccal-lingual relationship, then one or more canal should be suspected and searched on the other side, if the main canal is found in eccentric position. Dentinal map on the pulp chamber floor also helps the operator to the precise location of root canal orifices. 27 gauge, side vented irrigation needle were effectively used to flush out the debris from the canal system, without pushing it periapicaly. Intracanal medicament as, calcium hydroxide, various combinations of antibiotics are very effective in controlling intracanal infections by reducing the bacterial count [13]. Obturation was favoured with single cone technique, with filling of main buccal canal first followed by lingual canal.
In this case, the persistence mild pain reported by patient is due to missed lingual canal. Proper knowledge of canal anatomy, its variations and developed skills should be considered for proper management of such cases. In Endodontics, if magnification is done it will not only provide better vision but also facilitates the access for straight forward preparation and obturation of root canals. It will also cause less strain to eyes, ergonomics of the worker is improved, and concurrently prevents any technical errors [14].
Conclusion(s)
The root canal is a complex system. Identifying such variations is a challenge itself, clinician should be aware of variations related to canal configuration and types in mandibular second premolars. The key step in identifying the extra/split canal is tactile examination. In addition to such a highly developed imaging system, the use of intensification and the advanced canal preparation system helped us to deliver a predictable treatment outcome.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jul 23, 2019
Manual Googling: Feb 28, 2020
iThenticate Software: Mar 18, 2020 (20%)
[1]. Vertucci FJ, Haddix JE, Britto LR, Tooth morphology and access cavity preparation. In: Cohen S, Hargreaves KMPathways of the Pulp 2006 St. Louis Mosby:148-232. [Google Scholar]
[2]. Vertucci FJ, Root canal morphology and its relationship to endodontic proceduresEndod Topics 2005 10:03-29.10.1111/j.1601-1546.2005.00129.x [Google Scholar] [CrossRef]
[3]. Mittal N, Tomer A, Srivastava A, Treatment of mandibular first premolar with Type IV canal by intentional replantationJ Conserv Dent 2000 3(2):81-85. [Google Scholar]
[4]. Chalil NM, Kini S, Jose S, Narayanan A, Salahudeen S, Peedikayil FC, Endodontic treatment of a mandibular second premolar with Type IV Wiene’s root canal: A case reportCase Rep Dent 2014 2014:73146710.1155/2014/73146724711930 [Google Scholar] [CrossRef] [PubMed]
[5]. Al-Abdulwahhab B, Al-Nazhan S, Root canal treatment of mandibular second premolar with four root canalsSaudi Endod J 2015 5(3):196-98.10.4103/1658-5984.163630 [Google Scholar] [CrossRef]
[6]. Parekh V, Shah N, Joshi H, Root canal morphology and variations of mandibular premolars by clearing technique: an in vitro studyJ Contemp Dent Pract 2011 12(4):318-21.10.5005/jp-journals-10024-105222186868 [Google Scholar] [CrossRef] [PubMed]
[7]. Banga KS, Pawar AM, Nagpal D, Landge J, Thakur B, Rastogi S, Root canal morphology of premolar teeth in the population of Maharashtra (Pune) compared to the other Indian populationEndodontology 2018 30(1):15-20. [Google Scholar]
[8]. Iyer VH, Indira R, Ramachandran S, Srinivasan MR, Anatomical variations of mandibular premolars in Chennai populationIndian J Dent Res 2006 17(1):07-10.10.4103/0970-9290.2989816900889 [Google Scholar] [CrossRef] [PubMed]
[9]. Singh S, Pawar M, Root canal morphology of South Asian Indian mandibular premolar teethJ Endod 2014 40(5):1338-41.10.1016/j.joen.2014.03.02125043328 [Google Scholar] [CrossRef] [PubMed]
[10]. Gulabivala K, Aung TH, Alavi A, Ng YL, Root and canal morphology of Burmese mandibular molarsInt Endod J 2001 34:359-70.10.1046/j.1365-2591.2001.00399.x11482719 [Google Scholar] [CrossRef] [PubMed]
[11]. Ingle JI, Walton RE, Lambert GL, Lambert C, Taintor JF, Zidell JD, Preparation for endodontic therapy. In: Ingle JI, editorEndodontics 1985 3rd edPhiladelphiaLea and Febiger:54-101. [Google Scholar]
[12]. Vertucci FJ, Gegauff A, Root canal morphology of the maxillary first premolarJ Am Dent Assoc 1979 99(2):194-98.10.14219/jada.archive.1979.0255287737 [Google Scholar] [CrossRef] [PubMed]
[13]. Mittal N, Jain J, Antibiotics as an intracanal medicament in endodontics: A reviewInd J Dent 2013 4(1):29-34.10.1016/j.ijd.2012.03.002 [Google Scholar] [CrossRef]
[14]. Mittal N, Arora S, Endodontic treatment of mandibular second premolar with three root canals using dental operating microscopeEndodontology 2009 2:80-83. [Google Scholar]