The CAD remains the major cause of death and disability in developing countries. In India 20% deaths are due to CAD [1]. Diabetes remains one of the major factor in CAD and its complications, further the mortality risk is increased to 2-4 folds in CAD patients due to diabetes [1]. Diabetes mellitus and CAD are widely distributed diseases that occur in many persons all over the world. Despite the advances in the diagnosis and management, cardiovascular diseases remain the main important cause of mortality and morbidity in diabetic persons [2,3].
Epicardial Fat (EF) is the visceral fat deposits surrounding the heart which is accumulated between the visceral pericardium and the myocardium, and does not have any separate layer to distinguish it from the myocardium and the epicardial vessels [4]. It has the potential to initiate atherosclerosis over the coronaries through its local inflammatory properties. EF thickness can be measured using Echocardiography (ECG), Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) [5]. Transthoracic ECG has advantage over CT and MRI, because of it’s easy availability, low cost and high reproducibility above all no radiation risk [4,5]. SYNTAX-II scoring system which is an angiographic internet based calculator (www.syntaxscore.com), is used to calculate the severity of CAD based on anatomical features of coronary artery as found by angiogram along with demographic and clinical variable like gender, ejection fraction peripheral vascular disease smoking etc., There are studies [2,3,6-10] that used syntax scoring system and Gensini score to assess the correlation between the EFT and CAD; where the clinical and demographic variable were not individually studied.
Present study was taken up with aim to study the correlation between severity of CAD using SYNTAX-II scoring system and increased EFT in diabetic patients, as not many studies were done exclusively in diabetic patients who are at high risk of CAD.
Materials and Methods
This prospective observational study was conducted in the Department of General Medicine and cardiology in a tertiary care hospital between April 2018 and March 2019. Ethical Approval Number: 12/2017/122. After obtaining written informed consent, all diabetic patients diagnosed with CAD were enrolled, patients who were admitted in the department of general medicine and cardiology underwent coronary angiogram were also included in the study. Patients with cardiomyopathy, pericardial effusion, chronic kidney disease, non-diabetes and not willing to participate were excluded from the study.
Sample Size and Sampling Technique: After applying inclusion and exclusion criteria, one hundred patients were enrolled and subjected to detailed history of presenting symptoms, past history of CAD, PVD, clinical examination, anthropometry, lab investigation- HBA1C, blood urea, serum creatinine, ECG, 2D-ECHO and Coronary Angiogram (CAG).
Considering prevalence of Ischemic heart disease in diabetic patients 70% as per study done Jabbad HH et al., [11].

Sample size was rounded to 100
Where:
Z=Z value 1.96 for 95% confidence level
p=70% from previous study of prevalence of Ischemic heart disease in diabetic patients
c=confidence interval, expressed as decimal 0.1 (10%) allowable error
Transthoracic 2D-ECG
Each subject underwent detailed conventional transthoracic two-dimensional ECG with the subjects in left lateral decubitus position in the Department of Cardiology, done by same cardiologist for all 100 patients. EF pad thickness was identified as echo free space between the outer layer of myocardial wall and the visceral layer of the pericardium which was measured on the free wall of the right ventricle from both parasternal long and short axis views at mid ventricle during end diastole [9]. The maximum values at each site were measured and the average value was consider. The p-value <0.05 were considered as significant.
Coronary Angiogram (CAG)
As a part of management of CAD, participants were subjected to CAG, the angiogram results were used for syntax scoring with the help of cardiologist. The SYNTAX score II is a clinical tool that combines clinical variables with the anatomical SYNTAX score, providing expected four-year mortality for both CABG and PCI [1,6,12].
Statistical Analysis
Data was entered and analysed using SPSS version 16 (IBM) software. Pearson correlation test was used to analyse the correlation between EFT and severity of CAD. A p-value <0.05 was considered statistically significant.
Results
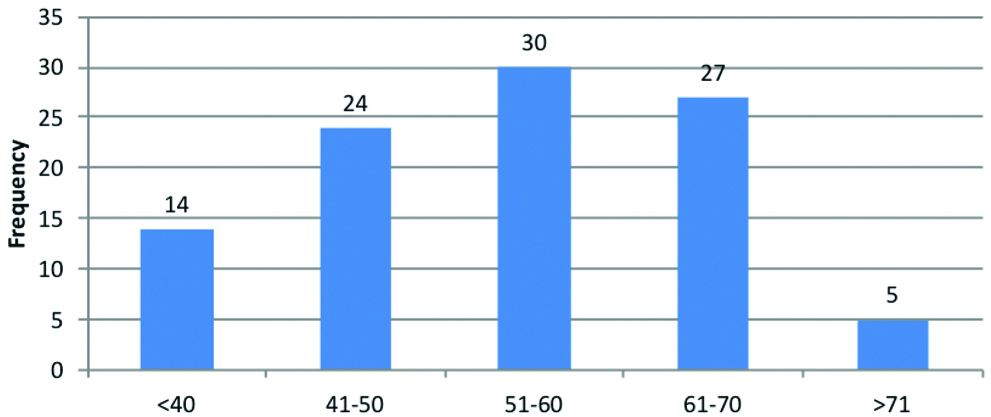
This study consisted of individuals with CAD with diabetes. A total of 100 subjects were included in the final analysis. The mean age was 54.22 years ranging from 33 to 80 years. The most common age group was 51-60 years accounting for 30% [Table/Fig-1]. Almost 77% of study population were males.
Age (years) distribution in the study population.
The mean EFT was 4.35 mm. The minimum thickness that noted was 2.50 mm and the maximum thickness was 6.20 mm with standard deviation of 0.71 [Table/Fig-2].
Epicardial fat thickness (EFT) in study population.
| Table | N | Minimum | Maximum | Mean | Std. deviation | CI 95% Lower bound | CI 95% Upper bound |
|---|
| EFT | 100 | 2.50 | 6.20 | 4.35 | 0.71 | 4.21 | 4.49 |
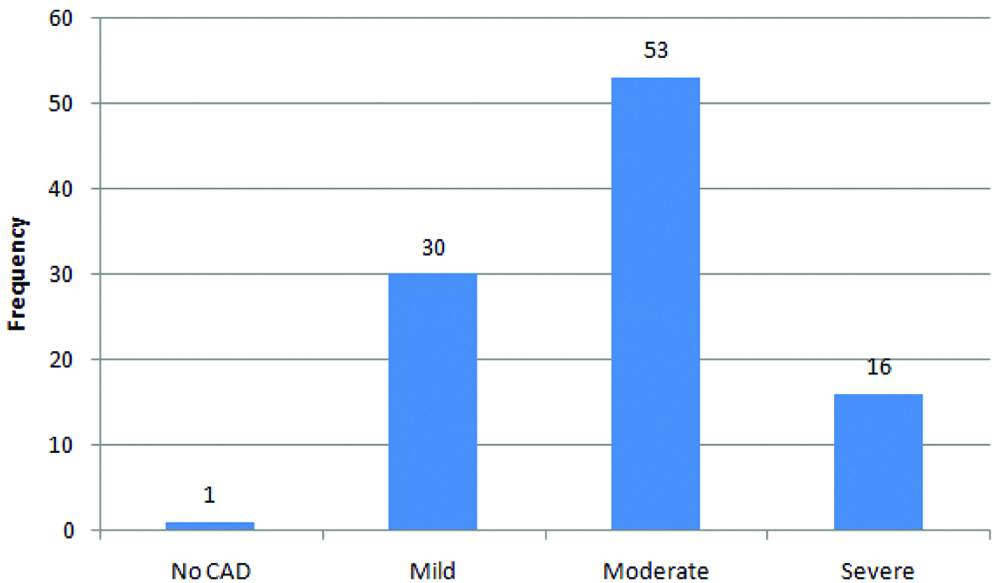
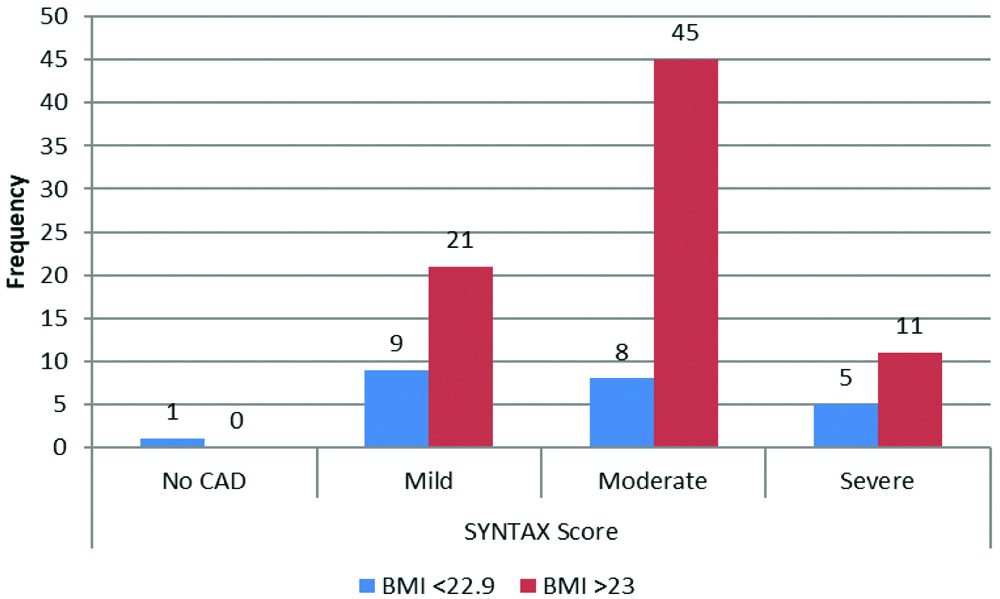
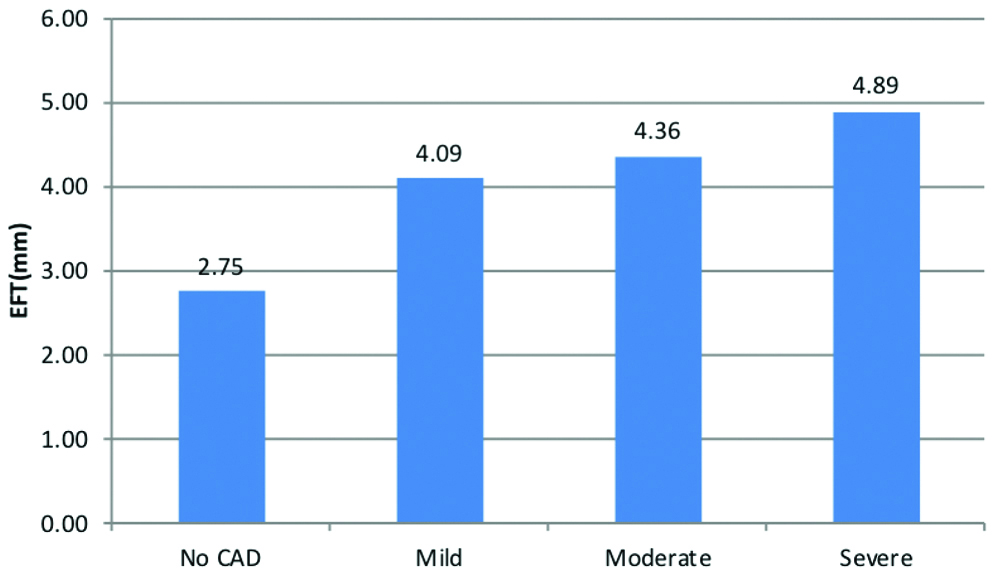
Among the study population, based on SYNTAX-II score, 53 cases had moderate CAD [Table/Fig-3]. The comparison between BMI and SYNTAX-II scoring system clearly explains the incidence of CAD and severity to be increased in subjects with BMI >23, p-value-0.083 [Table/Fig-4]. The [Table/Fig-5] depicts that with an increase in EFT the severity of CAD also increases.
Syntax scoring in study population.
Comparison between BMI and SYNTAX-II scoring.
Comparison between EFT and severity of CAD using syntax score-II.
| CAD | N | Mean | Std. deviation | 95% Confidence interval for mean | Minimum | Maximum |
|---|
| Lower bound | Upper bound |
|---|
| No CAD | 1 | 2.75 | | | | 2.75 | 2.75 |
| Mild | 30 | 4.09 | 0.55 | 3.89 | 4.30 | 3.40 | 5.65 |
| Moderate | 53 | 4.36 | 0.70 | 4.18 | 4.56 | 2.50 | 5.50 |
| Severe | 16 | 4.89 | 0.66 | 4.54 | 5.25 | 3.90 | 6.20 |
| Total | 100 | 4.35 | 0.71 | 4.21 | 4.50 | 2.50 | 6.20 |
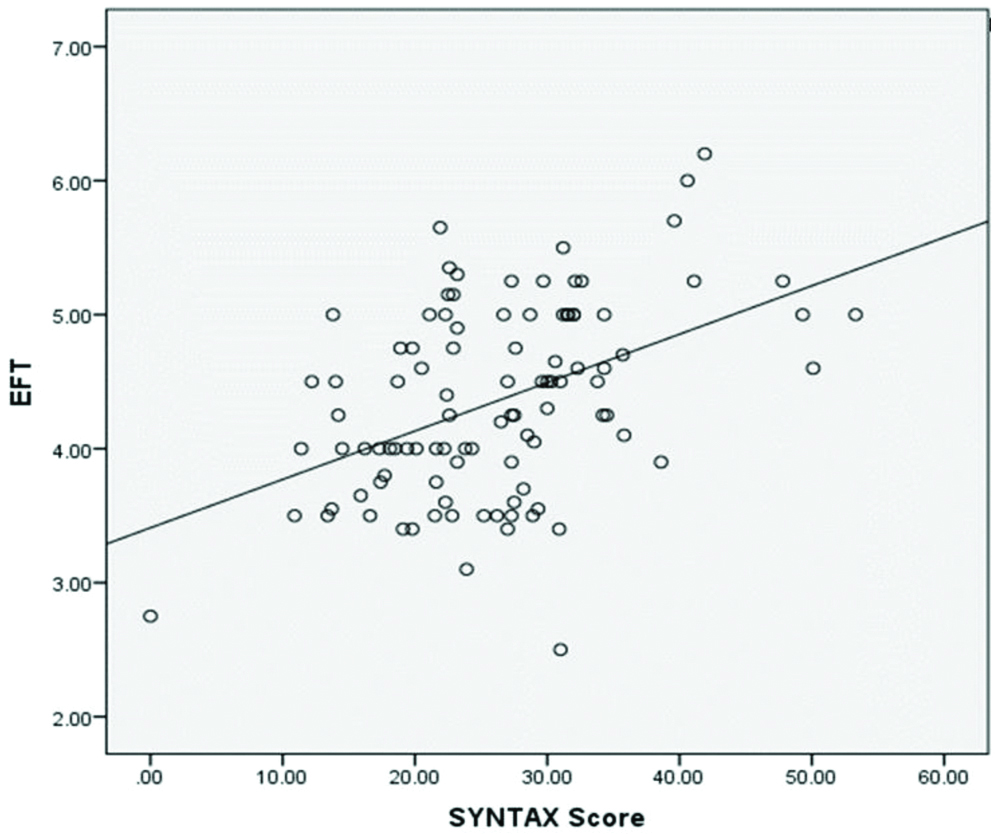
[Table/Fig-6,7] show a linear correlation between EFT and severity of CAD (p-value <0.0001).
Comparison between EFT and severity of CAD using SYNTAX-II scoring system.
Linear correlation between EFT and syntax scoring II system.
Discussion
EF has been recognised as a vital tool in early diagnosis and predicting outcome in CAD [5]. The results of this study build the existing evidence that the severity of CAD significantly correlates with the increase in thickness of EF. The subjects with severe CAD had increased EFT when compared to mild CAD which is consistent with similar worldwide studies [1,6,7]. This study had 77% obese patients. In this study, 77% of CAD patients were males with the mean age of 54.22 years, similar to study done in Iran [8], this increase in severity of CAD in males is due to the additional risk factors like smoking, alcohol consumption and sedentary life styles (but these factors were not considered in this study).
A 2D-ECHO was used for the measurement of EFT which has its own advantage over CT/MRI imaging, which have easy accessibility, cost effective and reproducible [8]. Moreover, drawbacks like observers variation, difficulty to measure the EFT in morbidly obese subjects and women with dense breast tissues could be overcome by measuring the EF by same cardiologist and positioning the patient in left lateral decubitus position. This adaptation helps in standardisation of measurement [4,5].
In this study EFT more than 4 mm predicts the CAD risk. Increased severity score significantly increases the EFT [2,5,10,13-15]. Due to several discrepancy regarding the cut-off value for EFT to find the extend of CAD, few studies reported EFT >5 mm associated with cardiovascular disease and deaths [2,9]. The study used quantitative SYNTAX-II scoring system to measure severity of CAD, significant correlation between EFT and CAD was noted [3,11].
Limitation(s)
This study was done only in diabetic subjects; other risk factors were not addressed. CT/MRI assessment of EFT would be more specific than conventional 2D-ECHO especially in morbidly obese subjects.
Conclusion(s)
Epicardial Fat (EF) increases the severity of CAD, prevention of which requires adequate lifestyle modification and intervention. Despite the availability of various new technologies, simple non-invasive 2D-ECHO can be used to identify the presence of cardiovascular disease even before the onset of symptoms especially in high risk populations. It also shares the potential to monitor the response to intervention. Longitudinal prospective study of progression of EFT with severity of CAD may throw some light on the pathogenesis of CAD.