Variable Antenatal Sonographic Findings of Thanatophoric Dysplasia- A Case Series
Richa Verma1, Navneet Sharma2
1 Assistant Professor, Department of Radiodiagnosis, Maharishi Markandeshwar Medical College and Hospital, Kumarhatti, Solan, Himachal Pradesh, India.
2 Assistant Professor, Department of Radiodiagnosis, Maharishi Markandeshwar Medical College and Hospital, Kumarhatti, Solan, Himachal Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Richa Verma, A14, MMU Campus, Kumarhatti, Solan, Himachal Pradesh, India.
E-mail: drrichaaverma88@gmail.com
Thanatophoric dysplasia is a lethal osteochondral dysplasia which occurs sporadically in 1/64,000-100,000 total live births and it is very common of the congenital lethal skeletal dysplasias. It is diagnosed on antenatal ultrasound based of findings of cloverleaf skull, macrocephaly, hydrocephalus, narrow thorax, shortened limbs, thickened subcutaneous tissue of extremities, platyspondyly and polyhydramnios. Two subtypes have been recognised on the basis of presence of bowing of shortened femur and cloverleaf skull. Type I is more frequent than Type II. Autosomal dominant mutations in the fibroblast growth factor Receptor 3 gene result in both subtypes. This condition has characteristic sonographic features that suggest the diagnosis prenatally. It is lethal condition with most neonates being dead within the first few hours or days of life. At present no specific treatment regimen is available. This condition can be diagnosed by ultrasonography in mid gestation scan. So the radiologist should carefully scan the fetus for any features of this entity and proper patient counselling should be done regarding prognosis of fetus and future implications. The present authors report three cases depicting antenatal findings of Thanatophoric dysplasia which include both subtypes. One of the cases includes twin pregnancy with one fetus being normal and another showing sonographic feature of thanatophoric dysplasia.
Clover leaf skull, Hydrocephalus, Polyhydramnios, Sonography
Introduction
Thanatophoric dysplasia was first described by Maroteaux et al., in 1967. A Greek word ‘Thanatophores’ meaning constantly bearing death lead to derivation of name of this deadly condition. The incidence of Thanatophoric dysplasia ranges from 1in 64000 to 1 in 100000 of total live births [1,2]. Besides shortening and bowing of limbs and cloverleaf skull, thanatophoric dysplasia is characterised by narrow thorax and protuberant abdomen. Polyhydramnios, macrocephaly, large anterior fontanel, frontal bossing, cloverleaf skull, prominent eyes, hypertelorism, flat facies with low nasal bridge, trident hand with brachydactyly, redundant skin folds, narrow, bell-shaped thorax with short ribs, generalised hypotonia, small pelvis small scapulae, severe platyspondyly, horizontal acetabular roofs, small sacroiliac notches, irregular metaphysis and short broad tubular bones in hands and feet are also associated with thanatophoric dysplasia [3].
Case Series
Case 1
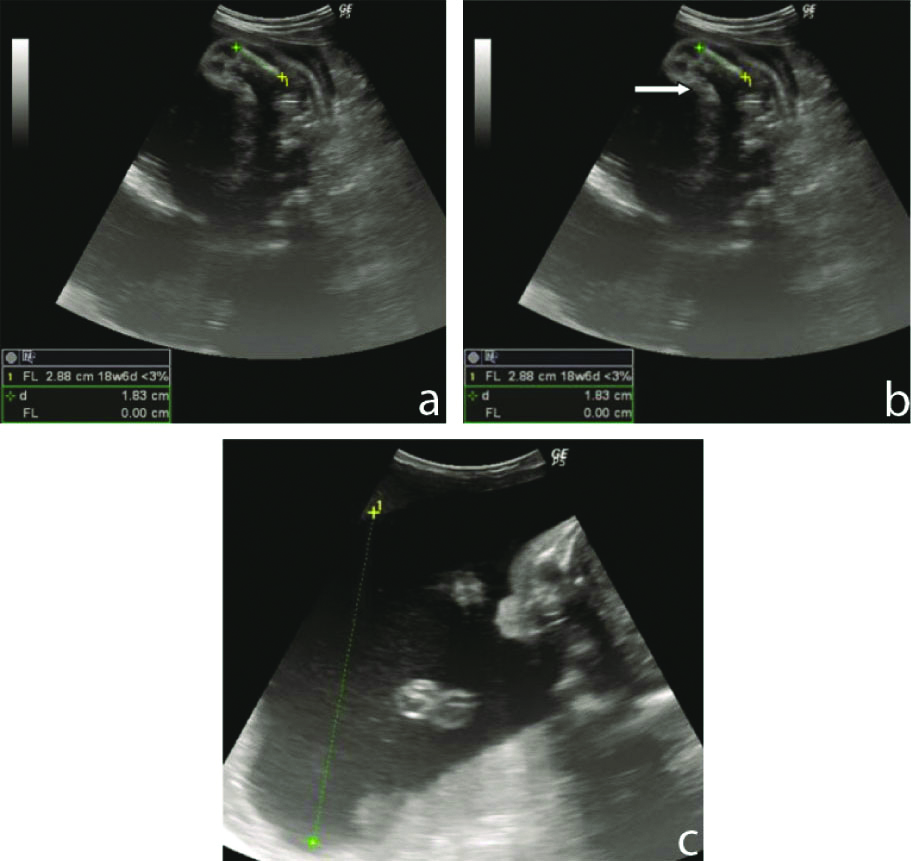
A 29-year-old female with a history of previous normal childbirth came for routine antenatal sonographic examination at period of gestation of 26 weeks. The height of uterus was noted to be more than gestational. Previous ultrasound scan at 11 weeks was normal. Present ultrasound examination revealed single live fetus with cloverleaf skull with hydrocephalus and macrocephaly [Table/Fig-1a]. Biparietal Diametre (BPD) and Head Circumference (HC) measured 8.44 cm and 30.68 cm corresponding to 34 weeks and 34 weeks 2 days respectively. Abdominal circumference corresponded to 26 weeks measuring 21.41 cm. The femur was shortened with femur length measuring 2.88 cm corresponding to gestation of 18 weeks 6 days. Femur was straight with thickened soft tissue of lower limbs [Table/Fig-1b]. There was also presence of polyhydramnios with AFI of 25 cm [Table/Fig-1c]. Based on these findings possibility of Thanatophoric Dysplasia Type 2 with ultrasound gestation age of 28 weeks 2 days was given.
a) Ultrasonogram showing single live fetus with cloverleaf skull with hydrocephalus and macrocephaly, b) Shortened femur with thickened subcutaneous tissue (arrow), c) Polyhdramnios.
Case 2
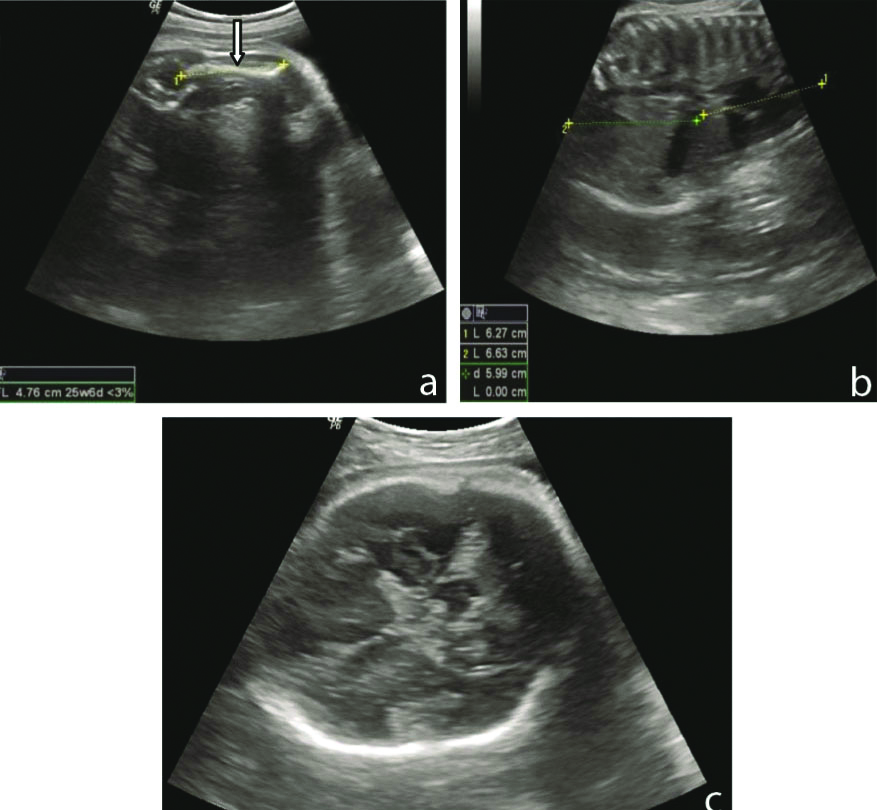
This case comprised sonography of a 23-year-old primigravida with gestation of 36 weeks which yielded the result of curved shortened humerus measuring 4.76 cm corresponding to 25 weeks 6 days [Table/Fig-2a] with other shortened limb bones. Femur length measured 4.81 cm corresponding to 26 weeks 1 day. Narrow thoracic cavity with protuberant abdomen was also seen [Table/Fig-2b]. Abdominal circumference was 9.76 cm corresponding to 31 weeks 5 days. There was presence of macrocephaly without cloverleaf skull or hydrocephalus [Table/Fig-2c]. Biparietal diameter and head circumference were also enlarged measuring 9.76 cm and 33.85 cm corresponding to 40 weeks and 39 weeks, respectively. These findings were suggestive of Type 1 Thanatophoric Dysplasia with ultrasound gestation age of 35 weeks 1 day.
a) Antenatal sonogram showing, Curved shortened humerus (white arrow), b) Narrow thoracic cavity with protuberant abdomen, c) Macrocephaly without hydrocephalus and cloverleaf skull.
Case 3
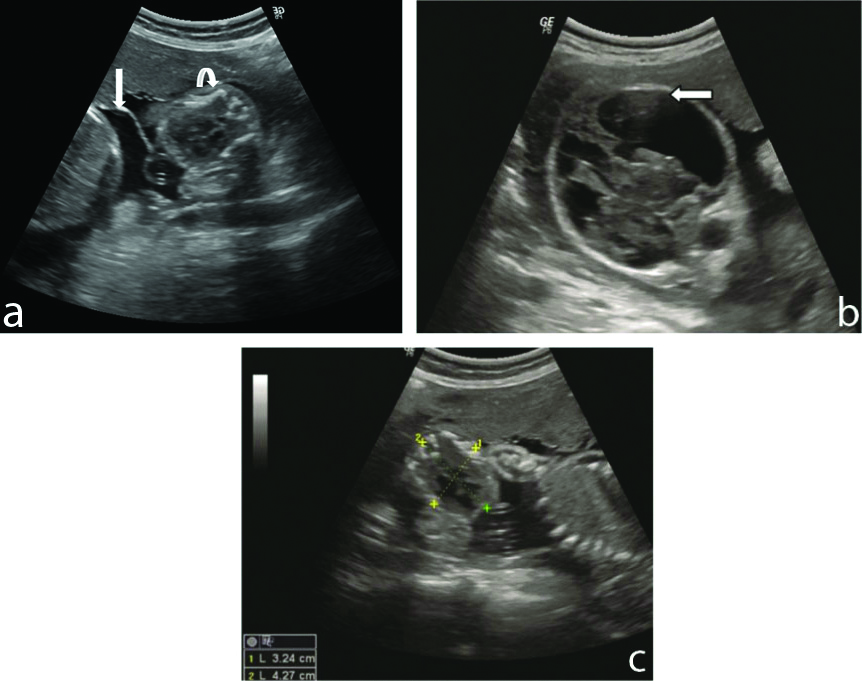
This was the interesting case involving a 27-year-old primigravida with period of gestation 27 weeks. On ultrasound, there was evidence of dichorionic diamniotic twin pregnancy [Table/Fig-3a]. One of the fetuses was abnormal showing hydrocephalus [Table/Fig-3b] BPD and HC measured 8.05 cm and 30.30 cm corresponding to 32 weeks and 3 days and 33 weeks and 1 day. Abdominal circumference revealed 35 weeks and 3 days gestational age measuring 31.44 cm. Curved shortened femur was observed measuring 1.76 cm corresponding to 15 weeks 2 days [Table/Fig-3a]. Other extremities were also shortened. The thoracic cavity was also narrowed [Table/Fig-3c]. Another foetus was absolutely normal with foetal age corresponding to period of gestation. So the abnormal foetus was assigned the diagnosis of Type 1 Thanatophoric Dysplasia with ultrasound gestational age of 33 weeks and 6 days.
a) Ultrasound showing, Diamniotic twin fetusesshowing intertwin membrane (black arrow) with abnormal fetus showing curved shortened femur (white arrow), b) Abnormal fetus showing hydrocephalus (white arrow), c) Abnormal fetus with narrow thoracic cavity with reduced AP diameter.
The routine labouratory investigations such as haemoglobin, ESR, routine blood sugar, liver function tests, renal function tests, thyroid function tests, urine tests were within normal limits in all three cases. All these cases delivered dead neonates with thanatophoric dysplasia. Unfortunately, post-birth images could not be obtained. Still all the cases represented the imaging spectra of both subtypes of Thanatophoric Dysplasia which are virtually diagnostic of this fatal condition.
Discussion
The polyhydramnios is supposed to be caused by compression of oesophagus by the small and the abdomen balloons out in bell shaped fashion. Due to respiratory insufficiency caused by reduced thoracic capacity and compression of brainstem, most of the thanatophoric babies die within the first few hours or days of life. Only sporadic case of thanatophoric has been reported yet [3]. Maternal Rubella infection has been proposed to be a probable aetiological factor [4].
De novo autosomal dominant mutations in the fibroblast growth factor receptor 3 gene mapped to chromosome band 4p16.3 are responsible for both subtyped of thanatophoric dysplasia [3]. No specific treatment regimen exists presently.
Two subtypes of thanatophoric dysplasia have been observed based on skull shape and femur morphology. Type I Thanatophoric dysplasia is having relative incidence of 80% and characteristically shows short-curved long bones especially femur giving telephone receiver appearance, with underdevelopment of vertebral column and pelvic bones. Cloverleaf skull is not necessarily present, whereas in Type 2 TD, the skull is cloverleaf giving tri-lobed configuration due to premature closure of lambdoid and coronal sutures. The long bones are normal in configuration in Type 2 [2]. Cloverleaf skull is distinct sonographic feature of Type 2, while it may or may not be present in Type 1. The other reported varieties are Torrance, San-Diego, and Luton types [4]. If shortened femur is found on antenatal ultrasound assessment, the radiologist should keep in mind the possibility of short limb dwarfism. The fetal spine, head, thorax, hands, and feet should be carefully evaluated to determine the exact type and prognosis of bony dysplasia [5].
One of the fetuses in twin or triplet pregnancy has increased risk of fetal malformations and bony dysplasia in comparison to the fetus in singleton pregnancy [6,7]. Thanatophoric dysplasia like genetic disorders remains a diagnostic dilemma because of their variations and unknown cause as the aetiology of these disorders lies in the disturbances in the complex processes of skeletal development, growth and homeostasis [8].
Cultured amniotic fluid cells or cord blood cells depict a missense mutation of 742C-->T (Arg248Cys) in all cases with Thanatophoric dysplasia 1 and a missense mutation of 1948A-->G (Lys650Glu) in the case with Thanatophoric dysplasia 2. This information is obtained by molecular analysis of the fibroblast growth factor receptor 3 gene by restriction enzyme digestion analysis and direct sequencing on the sample collected by amniocentesis or chorionic villous sampling. These adjunctive applications of molecular genetic analysis of the gene are useful for prenatal diagnosis of Thanatophoric dysplasia besides ultrasound [Table/Fig-3] [9-11].
Differential diagnosis includes achondrogenesis, achondroplasia, asphyxiating thoracic dystrophy (Jeune syndrome), hypophosphatasia, Osteogenesis imperfecta [2]. Cloverleaf skull, telephone receiver appearance of long bones and small thorax are characteristic ultrasound features to differentiate other causes of micromelia.
Thickened redundant skin fold limbs and craniofacial anomalies are visualized more clearly by three-dimensional ultrasound, thus giving an added advantage to detect thanatophoric dysplasia [4]. Three- dimensional ultrasound may be better than two -dimensional ultrasound as it allows review in a standard anatomic orientation to depict abnormal spatial features such as short ribs, splayed digits, and absent bones [2].
Proper counselling of the family, management of the pregnancy, and directing the appropriate postnatal radiologic evaluation should be the main aim of prenatal evaluation of thanatophoric dysplasia. If possible, postnatal examination and detailed radiographic examination of the fetus is also useful to precisely diagnose the type of skeletal dysplasia for genetic counselling [5].
Details of few cases of thanatophoric dysplasia reported earlier in literature from world along with comparison with present case series is shown in [Table/Fig-4].
Review of cases of thanatophoric dysplasia reported earlier in literature worldwide.
| Author’s name and year | Age of baby/babies | Diagnostic modalities | Outcome |
|---|
| Verma A et al., 2007 [1] | 32 weeks | Radiographs and clinical features | Still born |
| Mafinezhad S et al., 2012 [4] | 32 weeks, Dichorionic diamniotic twins | Clinical features and radiographs | Twin1-live and showed features of TD and died on day2.Twin 2-live and showed features of TD and died within hours. |
| Abdulkadir AY et al., 2008 [5] | 30 weeks | Ultrasound and radiographs | Dead fetus |
| Cho I et al., 2014 [6] | 39 weeks, Dichorionic twins | Ultrasound, Molecular studies via amniocentesis at 15 weeks | Twin1-showed features of TD and selective fetal termination done at 19 weeks and dead baby was delivered at 39 weeks.Twin2- healthy baby |
| Oga M et al., 1995 [7] | 30 weeks, Triplets | Ultrasound | 1st baby showed features of TD and died 34 minutes after birth.Other two babies were normal and healthy |
| Present cases, 2019 | Case1-diagnosed at 26 weeks | Ultrasound | Dead fetus |
| Case 2-diagnosed at 36 weeks | Ultrasound | Dead fetus |
| Case3-dichorionic diamniotic twins diagnosed at 27 weeks | Ultrasound | Twin1-showed TD and dead at time of birth.Twin2-Healthy fetus |
Conclusion(s)
Thanatophoric dysplasia is lethal skeletal dysplasia which can be diagnosed accurately by antenatal ultrasound. Ultrasound also helps in finding its subtypes as well as differentiating from other non-lethal dysplasias, Three dimensional ultrasound further compliments the two dimensional ultrasound to recognise other features of thanatophoric fetus. Molecular studies carried out via amniocentesis and chorionic villous sampling allows early diagnosis of this condition. All these modalities should be used to help the parents to have proper counselling and knowledge of this condition and decision making regarding the continuation of pregnancy.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Nov 26, 2019
Manual Googling: Feb 19, 2020
iThenticate Software: Feb 26, 2020 (10%)
[1]. Verma A, Mohan S, Kumar S, Thanatophoric dysplasia: Case report and review of literatureJournal of Clinical and Diagnostic Research 2007 1(4):308-10. [Google Scholar]
[2]. Badal S, Roy S, Singh D, Thanatophoric DysplasiaNepal Paediatr Soc 2015 35(3):304-06.10.3126/jnps.v35i3.11946 [Google Scholar] [CrossRef]
[3]. Arya S, Pandey K, Gupta D, Pande S, Thanatophoric dysplasia: A rare entityInt J Reprod Contracept Obstet Gynecol 2014 3(1):251-53.10.5455/2320-1770.ijrcog20140353 [Google Scholar] [CrossRef]
[4]. Mafinezhad S, Bozorgnia Y, Gharaee R, Thanatophoric dysplasia in newborn twins: Case report and literature reviewIranian Journal of Neonatolog 2012 3(1):36-40. [Google Scholar]
[5]. Abdulkadir AY, Isyaku K, Dare A, Abdullahi SG, Idris SK, Tabari AM, Prenatal third trimester sonographic behavior of a thanatophoric dwarfsJournal of Prenatal Medicine 2008 2(4):42-46. [Google Scholar]
[6]. Cho I, Shim JY, Kim GH, Yoo HW, Lee EJ, Won HS, Thanatophoric dysplasia in a dichorionic twin confirmed by genetic analysis at the early second trimester: A case report and literature reviewObstet Gynecol Sci 2014 57(2):151-54.10.5468/ogs.2014.57.2.15124678489 [Google Scholar] [CrossRef] [PubMed]
[7]. Oga M, Takai N, Yoshimatsu J, Fujisawa K, Gholbzouri K, Miyakawa I, Infant with thanatophoric dwarfism in triplet pregnancyGynecol Obstet Invest 1995 39(4):274-76.10.1159/0002924257635373 [Google Scholar] [CrossRef] [PubMed]
[8]. Warman ML, Cormier-Daire V, Hall C, Krakow D, Lachman R, LeMerrer M, Nosology and classification of genetic skeletal disorders: 2010 revisionAm J Med Genet A 2011 155A(5):943-68.10.1002/ajmg.a.3390921438135 [Google Scholar] [CrossRef] [PubMed]
[9]. Sharma M, Jyoti Jain R, Devendra Thanatophoric dysplasia: A case reportJournal of Clinical and Diagnostic Research 2015 9(11):QD01-03.10.7860/JCDR/2015/13201.670226675119 [Google Scholar] [CrossRef] [PubMed]
[10]. Gopal G, Belavadi GB, Thanatophoric dysplasia in the newbornJ of Evolution of Med and Dent Sci 2014 3(14):3665-69. [Google Scholar]
[11]. Chen CP, Chern SR, Shih JC, Wang W, Yeh LF, Chang TY, Prenatal diagnosis and genetic analysis of type I and type II thanatophoric dysplasiaPrenatal Diagnosis 2001 21(2):89-95.1097-0223(200102)21:2<89::AID-PD21<3.0.CO;2-9 [Google Scholar] [CrossRef]