Introduction
In day to day interactions, dark-shaded teeth are one of the major perceptible dental disharmonies [1]. In order to improve teeth colour, various in-office dental bleaching techniques can be employed [2]. For this therapy, hydrogen peroxide (20-38%) is the most commonly used agent [3]. While, numerous commercial presentations are available in the market, hydrogen peroxide remains the most commonly employed active ingredient [4]. What differentiates one bleaching agent from another is its handling properties and the additional components, such as thickeners, pigments, pH stabilisers and vehicle [5,6].
The bleaching gels act by oxidation which, when in contact with the teeth, dissociate into water and oxygen. They also generate other reactive molecules such as hydroxyl (OH-), peridroxyl (HO2-) and superoxide (O2-) ions [2,3]. The bleaching agents penetrate the dental surface due to their low molecular weight and protein denaturation. These characteristics of whitening gels facilitate the passage of the substance until it reaches the pigment molecules [2,3].
Thus, large pigmented molecules are broken down into smaller molecules and eliminated from dental structures by diffusion [3]. Pigmented molecules reflect a specific wavelength of light and are responsible for the colour of the enamel stain [7]. Therefore, chemical reversal of tooth darkening occurs due to the permeability of enamel and dentin, which requires close contact between the bleaching agent and mineralised dental tissues [4,6,7].
Regardless of the commercial agent used, the biochemical principle of the agents must be considered [8]. The success of tooth bleaching could depend on several factors, such as the age of the patient, degree of tooth darkening and correct use of the technique [5]. In addition, the permanence time of the gel on the teeth is also a determining factor for the success of the bleaching treatment [9].
Some studies showed that the aesthetic results were similar regardless of the commercial type of bleaching gel used, however, these studies evaluated only two bleaching gels [5,10]. Therefore, while choosing the bleaching agent, the clinician should consider selecting the one with the best manipulative form [2]. The viscosity of the agent is an important factor when choosing the bleaching gel [2,5]. Viscosity allows the gel to remain on the tooth without flowing onto the soft tissues, and has no effect on the outcome of the bleaching treatment [5].
However, with of so many commercial presentations available in the market, it is common for clinicians to be confused about selecting the best and most effective in-office bleaching gel. Thus, the present case series was carried out to evaluate the effect of 8 in-office bleaching gels using the split-mouth design (on 4 patients). And to check if there is greater effectiveness of some particular concentration, viscosity and/or bleaching protocol as recommended by the manufacturers.
Case Report
A total of 4 patients of the same age (22 years) with good general and oral health conditions were included in this study. The patients visited the dental school of the Faculdade de Odontologia de Pernambuco (FOP/UPE) between March and July 2019. All of them had the same dental colour (A2, in the upper central incisors), had not undergone any previous bleaching treatment, had no extensive restorations on the anterior teeth and no contraindications to undergoing in-office dental bleaching procedure.
Prior to the start of the bleaching procedures, the patients provided written consent for the treatments to be performed. Overall, 3 in-office teeth bleaching sessions were held with 7-day intervals between the sessions. In each patient, 2 different bleaching agents were applied, using the split-mouth design, on the left and right hemiarches (maxillary and mandibular), respectively, following manufacturers’ recommendations for use [Table/Fig-1].
In-office bleaching gels.
| Bleaching gels | Composition | Protocol | Lot |
|---|
| Whiteness HP (FGM, Santa Catarina, Brazil) | 35% Hydrogen Peroxide, Thickener, Red Dye, Glycol, and Water | Three 15-minute applications | 260719 |
| Whiteness HP Blue (FGM, Santa Catarina, Brazil) | 35% Hydrogen Peroxide, Violet Inert Pigment, Neutralising Agents, Calcium Gluconate, Glycol, and Deionized water | A 45-minute application | 180419 |
| Whiteness HP Maxx (FGM, Santa Catarina, Brazil) | 35% Hydrogen Peroxide, Thickeners, Mixture of Dyes, Glycol, Inorganic Filler, and Deionized Water | Three 15-minute applications | 250119 |
| Pola Office Plus (SDI, Victoria, Australia) | 37.5% Hydrogen Peroxide, Thickener, Catalysts, Dyes, Desensitising Agents, and Water | Three 8-minute applications | 190822103309 |
| Total Blanc Office (DFL, Rio de Janeiro, Brazil) | 35% Hydrogen Peroxide, Thickener, Plant Extracts, Amide, Glycol, Dye, and Water | A 45-minute application | 19080924 |
| Mix One Supreme (Villevie, Santa Catarina, Brazil) | 35% Hydrogen Peroxide, Thickeners, Humectant, Emollient, pH Corrector, Food Colouring Cl 19140 (tartrasine yellow), and Flavouring | Three 15-minute applications | 175 |
| Potenza Bianco Pro (PHS, Santa Catarina, Brazil) | 35% Hydrogen Peroxide, Thickener, Dye, Glycol, and Water | Three 15-minute applications | 30092019 |
| Opalescence Boost (Ultradente, Utah, USA) | 40% Hydrogen Peroxide, Sodium Fluoride, Potassium Nitrate, Thickeners, Dyes, and Water | A 20-minute application | D08W2 |
Before and after each bleaching session, the dental colour was recorded for the two upper central incisors (11 and 21) three times to get an average score. The colour was measured using a digital spectrophotometer (Vita Easy Shade, VITA Zahnfab-rik, Bad Sackingen, Germany), by placing the equipment on the central portion of each tooth before and after the bleaching treatment [Table/Fig-2-C,3-C,4-C, 5-C].
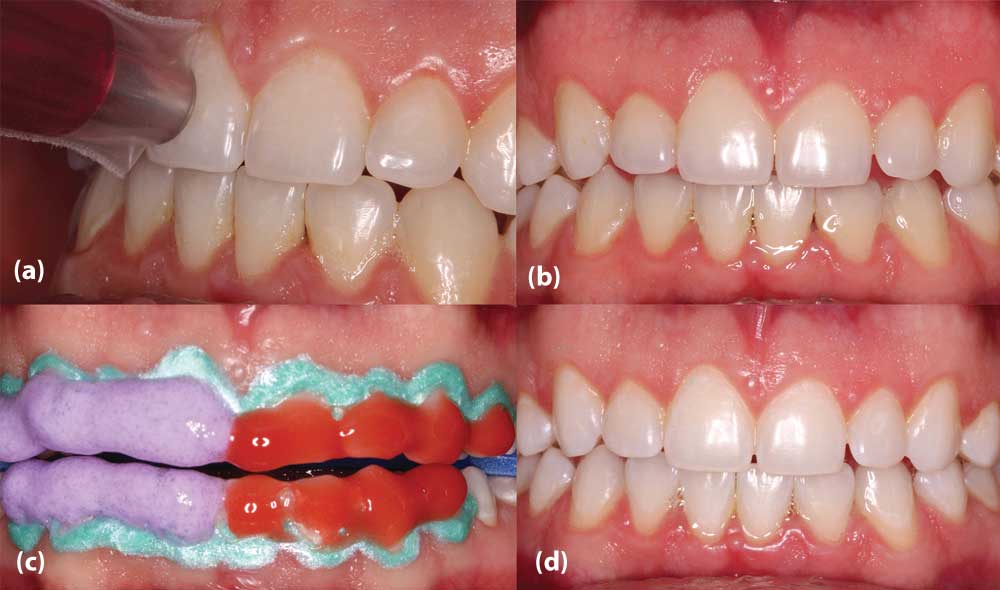
(a) Colour measurement with digital spectrophotometer; (b) Initial clinical aspect; (c) Application of bleaching gels; (d) Final clinical aspect after the third in-office bleaching session. (Patient #1 bleaching with Whiteness HP (FGM) and Potenza Bianco Pro (PHS) bleaching gels).

(a) Colour measurement with digital spectrophotometer; (b) Initial clinical aspect; (c) Application of bleaching gels; (d) Final clinical aspect after the third in-office bleaching session. (Patient #2 bleaching with Whiteness HP Maxx (FGM) and Mix One Supreme (Villevie) bleaching gels).

(a) Colour measurement with digital spectrophotometer; (b) Initial clinical aspect; (c) Application of bleaching gels; (d) Final clinical aspect after the third in-office bleaching session. (Patient#3 bleaching with Whiteness HP Blue (FGM) and Opalescence Boost (Ultradent) bleaching gels).
(a) Colour measurement with digital spectrophotometer; (b) Initial clinical aspect; (c) Application of bleaching gels; (d) Final clinical aspect after the third in-office bleaching session. (Patient #4 bleaching with Pola Office Plus (SDI) and Total Blanc Office (DFL) bleaching gels).

For in-office bleaching, a simple randomisation (sealed brown envelopes) was performed to allocate the bleaching gels to the patients. The details of the bleaching agents used are given in [Table/Fig-1].
In all cases, prophylaxis was performed with pumice paste and water before each bleaching session, followed by soft tissue protection using lip retractor, lingual protector, suction and gingival barrier. After these, initial procedures were completed, the envelopes were opened and the agents were applied as directed. The first agent drawn was applied to the right hemi-arches and the second to the left hemi-arches. After the application time, the gels were removed with an aspiration cannula and the teeth were rinsed with water.
Patients were instructed to avoid foods that can stain teeth (red wine, coffee, coke, açaí, chocolate) or drinks with an acidic pH (lemon and orange juice). In addition, patients were instructed to refrain from smoking.
In subsequent sessions, the same gels were used for the same hemiarches. After each whitening session, patients were instructed to complete a visual analog scale assessment for post-operative sensitivity (1 hour, 2 hours, 6 hours and 12 hours after the whitening procedure). The analysis of the results was carried out for descriptive and qualitative purpose.
Results
Patient #1
A 22-year-old male patient underwent bleaching with Whiteness HP (FGM) and Potenza Bianco Pro (PHS) bleaching gels.
Patient #2
A 22-year-old male patient underwent bleaching with Whiteness HP Maxx (FGM) and Mix One Supreme (Villevie) bleaching gels.
Patient #3
A 22-year-old male patient underwent bleaching with Whiteness HP Blue (FGM) and Opalescence Boost (Ultradent) bleaching gels.
Patient 4
A 22-year-old female patient underwent bleaching with Pola Office Plus (SDI) and Total Blanc Office (DFL) bleaching gels.
Colour variations were determined using the CIELab system parameters (L*a *b*), where L * corresponds to brightness, with values ranging from 0 (black) to 100 (white), the value of a * corresponds to the green red axis and b * to the yellow-blue axis. A high ΔE value indicates a large colour difference. The colour variation (∆E) and lightness variation (∆L) were determined by the following equation [6]:
∆E= {(L*2–L*1)2+(a*2–a*1)2+(b*2–b*1)2}1/2E∆L= (L*2–L*1)(Subscripts 1 and 2 refer to the colour coordinates before and after bleaching, respectively.)
Colour measurements as well as ∆E and ∆L are shown in [Table/Fig-6].
Initial /final colour evaluations, colour variation (∆E), and lightness variation (∆L) after bleaching treatments.
| Patient 1 | Patient 2 | Patient 3 | Patient 4 |
|---|
| Tooth 11 | Tooth 21 | Tooth 11 | Tooth 21 | Tooth 11 | Tooth 21 | Tooth 11 | Tooth 21 |
|---|
| Baseline | A2 | A2 | A2 | A2 | A2 | A2 | A2 | A2 |
| Final | B1 | B1 | B1 | B1 | B1 | B1 | B1 | B1 |
| ∆E | 4.78 | 4.60 | 4.56 | 4.41 | 4.36 | 4.75 | 3.23 | 3.52 |
| ∆ L | 4.3 | 4.3 | 4.2 | 4.2 | 4.2 | 4.3 | 3.1 | 3.2 |
Baseline: Before bleaching treatment; Final: After 3 weeks of bleaching treatment
Discussion
In this study, a split-mouth design was used that consists of subdividing the dentition into halves (right and left), where more than one treatment modality is assigned to the same patient [11]. The split-mouth design allows the evaluation of different therapeutic protocols under similar oral health conditions [2]. According to Zhu H et al., the split-mouth design has the advantage of minimising the variables among the study participants [12].
A digital spectrophotometer was used for colour assessments, which facilitates an accurate recording of dental colours. Visual colour assessments depend on many subjective factors, such as the observer’s colour perception, lighting conditions, optical properties of the materials, and manufacturing of colour guides [13]. According to Brandt J et al., the VITA Easyshade spectrophotometer is one of the most reliable colour assessment instruments used in-vitro and in-vivo [13].
In all the 4 cases, no differences in shades were observed between the hemiarches treated with different bleaching gels. These results were consistent with the clinical trial by Penha ES et al., who evaluated two in-office bleaching agents using the split-mouth design, and attributed this result to the active principle ingredient of the bleaching gels (hydrogen peroxide), independent of the other constituents of the gel [10].
In another split-mouth clinical study, at-home bleaching was compared with combined bleaching (in-office + at-home). No statistically significant differences were observed between the hemiarches treated with different protocols [14]. Similarly, another study evaluated the influence of light source on the result of the bleaching treatment, and found no significant difference between the different protocols tested [15]. These findings suggested that the result of bleaching treatment was related to the physiology of each patient rather than the bleaching agent, protocol or technique used.
All bleaching agents employed in this study had a hydrogen peroxide concentration of 35%, except for Pola Office Plus (37.5%) and Opalescence Boost (40%). However, the small differences in the concentrations of the bleaching agents did not affect the final bleaching colour. Borges AB et al., evaluated different concentrations of hydrogen peroxide bleaches (20%, 25%, 30% and 35%) on the enamel microhardness and colour change, but did not observe any statistically significant differences in these parameters [16].
Regarding post-operative sensitivity, no patient reported any difference in sensitivity between the hemiarches. The results of the present study were consistent with those of other studies, where no difference in sensitivity was observed when different bleaching agents were used [10,17].
In this study bleaching agents with different viscosities were used. However, the viscosity of the bleaching gel did not influence the result of the bleaching treatment in any case. These results are consistent with the study by Kwon SR et al., wherein the efficacies of the bleaching gels with different viscosities (low, medium and high) were evaluated, and no statistically significant differences were observed between them [5]. In this study, different concentrations of bleaching gels and different application protocols employed also do not seem to influence the result of the tooth bleaching treatment.
Therefore, it is up to the clinician to choose affordable bleaching gels with good viscosity and easy handling.
Whiteness HP Blue, Opalescence Boost, and Total Blanc bleaching gels come in the form of two attached syringes, and the homogenised gels transfer the contents from one syringe to the other. Pola Office Plus is a double-barrelled syringe with a self-mixing tip that allows for homogenisation at the same time when the gel is applied to the dental tissues. Mix One Supreme is brush-shaped, and the bleaching agent is homogenised in the bristles that are brushed on the teeth. These agents appear to be more practical to use as they are pre-dosed from the factory and have the advantage of no risk of incorrect gel and thickener delivery.
On the other hand, Whiteness HP, Whiteness HP Maxx, and Potenza Bianco bleaching gels are handled by self mixing in a container with a spatula in the ratio of 3:1 drops of peroxide to thickener and are operator-dependent.
One of the limitations of the present study was the number of patients analysed. Randomised controlled trials should be encouraged for further scientific evidence. However, these cases raise the hypotheses about the effectiveness of the myriad bleaching agents available in the market.
Conclusion(s)
The different commercial presentations of the in-office bleaching gels showed similar results. The different compositions of the bleaching gels did not seem to influence the treatment result. Therefore, the clinician should opt for relatively more affordable bleaching gels with good viscosity and easy handling properties.
[1]. Ferraz NKL, Nogueira LC, Neiva IM, Ferreira RC, Moreira NA, Magalhães CS, Longevity, effectiveness, safety, and impact on quality of life of low-concentration hydrogen peroxides in-office bleaching: A randomized clinical trialClin Oral Investig 2019 23(5):2061-70.10.1007/s00784-018-2607-730238417 [Google Scholar] [CrossRef] [PubMed]
[2]. Espíndola-Castro LF, Silva MPDS, Oliveira JFG, Melo Filho SMC, Monteiro GQM, Influência da mudança de protocolo de clareamentodentárioemconsultório no resultadoestético: CasoclínicoRevistaUningá 2018 55(3):130-39. [Google Scholar]
[3]. Rezende M, Ferri L, Kossatz S, Loguercio AD, Reis A, Combined bleaching technique using low and high hydrogen peroxide in-office bleaching gelOper Dent 2016 41(4):388-96.10.2341/15-266-C26919081 [Google Scholar] [CrossRef] [PubMed]
[4]. Mena-Serrano AP, Parreiras SO, Nascimento ED, Borges CPF, Berger SB, Loguercio AD, Effects of the concentration and composition of in-office bleaching gels on hydrogen peroxide penetration into the pulp chamberOper Dent 2015 40(2):E76-82.10.2341/13-352-L25535786 [Google Scholar] [CrossRef] [PubMed]
[5]. Kwon SR, Pallavi FNU, Shi Y, Oyoyo U, Mohraz A, Li Y, Effect of bleaching gel viscosity on tooth whitening efficacy and pulp chamber penetration: An in vitro studyOper Dent 2018 43(3):326-34.10.2341/17-099-L29676980 [Google Scholar] [CrossRef] [PubMed]
[6]. Loguercio AD, Servat F, Stanislawczuk R, Mena-Serrano A, Rezende M, Prieto MV, Effect of acidity of in-office bleaching gels on tooth sensitivity and whitening: A two-center double-blind randomized clinical trialClin Oral Investig 2017 21(9):2811-18.10.1007/s00784-017-2083-528303471 [Google Scholar] [CrossRef] [PubMed]
[7]. Bicer CO, Oz FD, Attar N, Effects of two different bleaching agents on surface roughness and microhardness of different novel nano-restorative materialsEuropean J Gen Dent 2017 6(2):86-91. [Google Scholar]
[8]. Majeed A, Farooq I, Grobler SR, Rossouw RJ, Tooth-bleaching: A review of the efficacy and adverse effects of various tooth whitening productsJ Coll Physicians Surg Pak 2015 25(12):891-96. [Google Scholar]
[9]. Chisini LA, Conde MCM, Meireles SS, Dantas RVF, Sarmento HR, Della Bona A, Effect of temperature and storage time on dental bleaching effectivenessJ Esthet Restor Dent 2019 31(1):93-97.10.1111/jerd.1243930379397 [Google Scholar] [CrossRef] [PubMed]
[10]. Penha ES, Pinto WR, Santos RL, Guênes GMT, Medeiros LA, Lima AMA, Avaliação de diferentessistemas de clareamento dental de consultórioRevista da Faculdade de Odontologia-UPF 2015 20(3):281-86.10.5335/rfo.v20i3.4286 [Google Scholar] [CrossRef]
[11]. Pozos-Guillén A, Chavarría-Bolaños D, Garrocho-Rangel A, Split-mouth design in paediatric dentistry clinical trialsEur J Paediatr Dent 2017 18(1):61-65. [Google Scholar]
[12]. Zhu H, Zhang S, Ahn C, Sample size considerations for split-mouth designStat Methods Med Res 2017 26(6):2543-51.10.1177/096228021560113726303156 [Google Scholar] [CrossRef] [PubMed]
[13]. Brandt J, Nelson S, Lauer HC, Von Hehn U, Brandt S, In vivo study for tooth colour determination-visual versus digitalClin Oral Investig 2017 21(9):2863-71.10.1007/s00784-017-2088-028265772 [Google Scholar] [CrossRef] [PubMed]
[14]. Machado LS, Anchieta RB, Santos PH, Briso ALF, Tovar N, Janal MN, Clinical comparison of at-home and in-office dental bleaching procedures: A randomized trial of a split-mouth designInt J Periodontics Restorative Dent 2016 36(2):251-60.10.11607/prd.238326901303 [Google Scholar] [CrossRef] [PubMed]
[15]. Mondelli RFL, Francisconi AC, Almeida CMD, Ishikiriama SK, Azevedo JED, Comparative clinical study of the effectiveness of different dental bleaching methods-two year follow-upJ Appl Oral Sci 2012 20(4):435-43.10.1590/S1678-7757201200040000823032205 [Google Scholar] [CrossRef] [PubMed]
[16]. Borges AB, Zanatta RF, Barros ACSM, Silva LC, Pucci CR, Torres CRG, Effect of hydrogen peroxide concentration on enamel color and microhardnessOper Dent 2015 40(1):96-101.10.2341/13-371-L25136902 [Google Scholar] [CrossRef] [PubMed]
[17]. Reis A, Kossatz S, Martins GC, Loguercio AD, Efficacy of and effect on tooth sensitivity of in-office bleaching gel concentrations: A randomized clinical trialOper Dent 2013 38(4):386-93.10.2341/12-140-C23327226 [Google Scholar] [CrossRef] [PubMed]