Gastric Volvulus with Torsion of Wandering Spleen: A Rare Case of Acute Abdomen
Vijaya L Patil1, Prasad Sasnur2, Shruti G Sheelin3, Nagaraj Biradar4
1 Professor, Department of General Surgery, BLDEU’s Shri B. M. Patil Medical College, Hospital and Research Centre, Vijayapur, Karnataka, India.
2 Assistant Professor, Department of General Surgery, BLDEU’s Shri B. M. Patil Medical College, Hospital and Research Centre, Vijayapur, Karnataka, India.
3 Junior Resident, Department of General Surgery, BLDEU’s Shri B. M. Patil Medical College, Hospital and Research Centre, Vijayapur, Karnataka, India.
4 Junior Resident, Department of General Surgery, BLDEU’s Shri B. M. Patil Medical College, Hospital and Research Centre, Vijayapur, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vijaya L Patil, Department of General Surgery, BM Patil Medical College, Vijayapur-586103, Karnataka, India.
E-mail: drvijayapatil@yahoo.com
Gastric volvulus with splenic torsion presenting as acute abdomen is a rare entity. Gastric volvulus is characterised by rotation of more than 180° either along long axis (organo-axial) or short axis (mesentrico-axial), resulting in partial or complete obstruction of the gastric lumen. If untreated, it results in strangulation, ischemia, necrosis, and finally gastric perforation with increased mortality. Wandering spleen is also a rare entity characterised by underdevelopment or absence of one or all of the ligaments that hold the spleen in its normal position, which may rarely lead to splenic torsion. It requires urgent diagnosis and treatment to overcome life threatening complications. Here we report a case of a 17-year-old females patient with acute gastric volvulus, presenting with perforative peritonitis with torsion of wandering spleen as seen in Contrast enhanced computed tomography of abdomen which showed pneumoperitoneum, raised left dome of diaphragm with organo-axial gastric volvulus, with non-visualisation of spleen in its normal position with ascites. Upper GI Endoscopy confirmed that visualised part of mucosa to be gangrenous, scope was partially negotiable till fundus. Patient was posted for emergency laparotomy. On laparotomy-spleen was seen anterior to fundus and gangrenous with visible torsion of splenic pedicle.
Gastric lumen, Perforative peritonitis, Splenic torsion
Case Report
A 17-year-old female presented to emergency room with abdominal pain, abdominal distention, vomiting, etching of two days duration and one episode of melena. She gave history of recurrent abdominal pain and vomiting since past one year.
On examination, patient was in shock, BP-86/50mmHg, tachycardia (PR-138/min), tachypnea (RR-28/min). Abdominal examination revealed grossly distended abdomen, diffuse abdominal tenderness, guarding with absent bowel sounds. Patient was resuscitated in emergency room with intravenous fluids and was started on inotropic support with Inj Noradrenaline at 4 mL/hr and Inj Dopamine at 4 mL/hr.
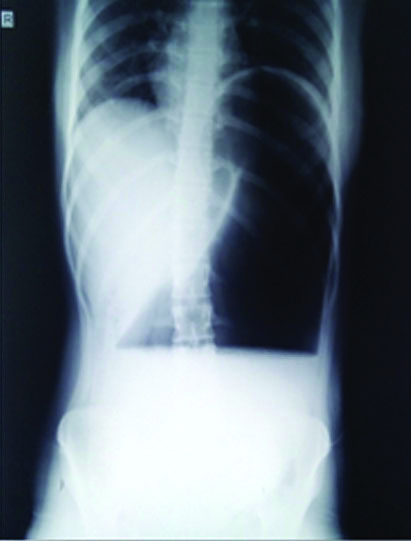
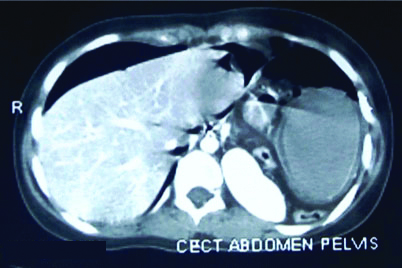
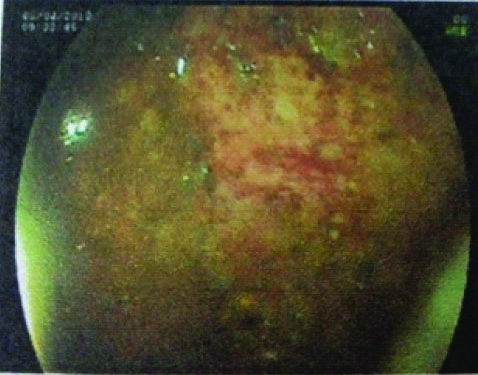
Laboratory investigations revealed Haemoglobin 12.5 gm%, total count of 11,100 cells/cumm with predominant neutrophils 85%, Platelet count of 1,92,000 cells/cumm. Serum electrolytes, renal parameters, urine analysis were within normal range. X-ray of abdomen [Table/Fig-1] showed raised left dome of diaphragm, with huge dilated stomach. Ultrasound of abdomen showed massively dilated stomach, with spleen in ectopic position with whirl appearance and free fluid in abdomen. Contrast enhanced computed tomography of abdomen [Table/Fig-2] showed pneumoperitoneum, raised left dome of diaphragm with organoaxial gastric volvulus, with non-visualisation of spleen in its normal position with ascites. Upper GI Endoscopy [Table/Fig-3] was confirmatory which showed, visualised part of mucosa to be gangrenous, scope was partially negotiable till fundus, not negotiated till duodenum.
Erect X-ray abdomen showing huge distended stomach.
Axial view of contrast enhanced computed tomography scan of abdomen and pelvis.
Upper GI endoscopy showing necrosis of gastric mucosa.
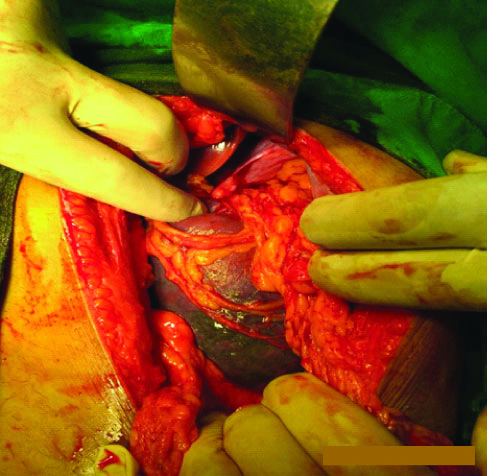
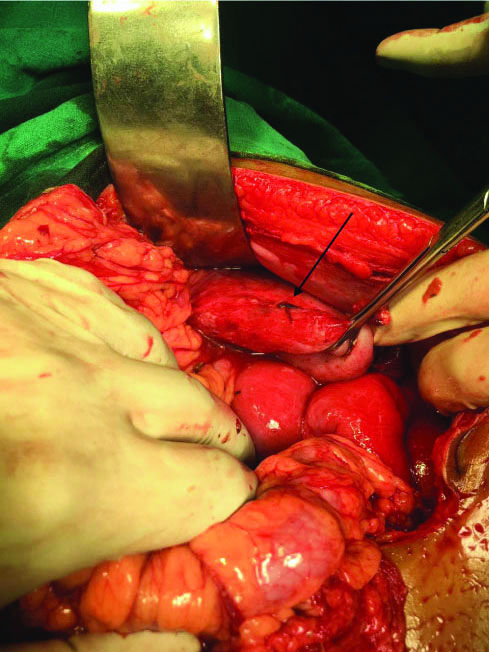
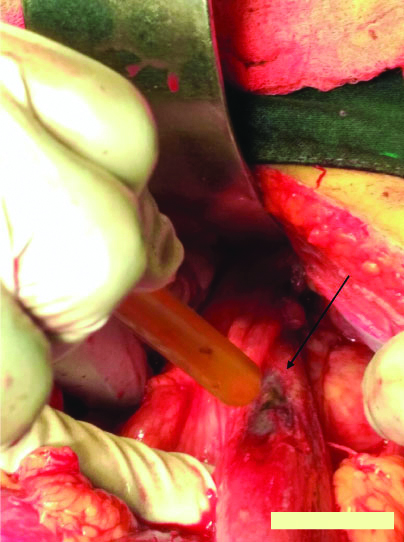
With diagnosis of acute gastric volulus and gastric perforative peritonitis, patient was posted for emergency laparotomy. On laparotomy-spleen was seen anterior to fundus [Table/Fig-4], was gangrenous with visible torsion of splenic pedicle [Table/Fig-5], no ligamentous attachments to the spleen were seen, after splenectomy visualised stomach was distended with organoaxial volvulus and perforation of size 4×4 mm seen on posterior surface of body [Table/Fig-6a,b]. Stomach was decompressed, derotated and opened which showed whole of stomach mucosa to be gangrenous with no bleeding from cut edge.
Laparotomy image showing wandering spleen with splenic infarction.
Laparotomy image showing torsion of splenic pedicle.

Perforation (arrow) over posterior surface of body of stomach.
Laparotomy image showing perforation (arrow) over posterior surface of body of stomach.
On account of total gangrene of stomach with splenic torsion, splenectomy with total gastrectomy with Roux-n-Y oesophago-jejunostomy with jejuno-jejunostomy was done.
Postoperatively, patient was on inotropic support. On post-operative day five, she showed signs of pneumonia with septicaemia and succumbed to death due to cardiorespiratory failure.
Discussion
An abnormal rotation of stomach of more than 180° is defined as gastric volvulus. It can be organo-axial, mesentrico-axial or combined. Organo-axial (59%) is more common than mesentrico-axial (29%), comprising 2/3rd of cases. Gastric volvulus was 1st described by Berti in 1866, it is an extremely rare condition presenting as acute abdomen [1,2].
If untreated, it results in strangulation, ischemia, necrosis and finally perforation [3]. Mortality rates can be 30-50% [4]. Wandering spleen is another rare condition with incidence of about 0.2% [5]. It mainly affects children, who make-up one-third of all cases with increased female preponderance [6]. In adults it is more common in women of reproductive age group.
It is characterised by excessive mobility of spleen and displacement from original position to another location caused by under-development or absence of gastro-splenic, spleno-renal, spleno-colic ligaments resulting in hyper mobile spleen [7]. In presence of elongated splenic pedicle, torsion may occur resulting in acute abdominal pain and may lead to splenic infarct which is a potentially fatal condition [8,9]. It has incidence of around 0.25% [3]. This condition has bimodal incidence which include children less than 10 years of age and women of childbearing age [4].
Mortality secondary to ischemia and gastric necrosis range about 42%-56% [10]. There exists a rare association between gastric volvulus and wandering spleen. These two entities share common cause i.e., failure of fusion of dorsal mesentry with posterior body during foetal development which leads to failure/incomplete intra-peritoneal visceral ligaments [2,11].
Association of gastric volvulus with splenic torsion is extremely rare and is a diagnostic challenge for surgeons [12]. This index case is unique, being a female adolescent patient and there was torsion of wandering spleen along with gastric volvulus.
The diagnosis of this rare clinical entity is very challenging. Imaging plays an important role in diagnosis. Gastric volvulus presenting with acute abdomen requires immediate surgical intervention. The most approved surgical treatment is anterior gastropexy [7]. Subtotal or total gastrectomy is done when stomach appears gangrenous [2,11]. Splenopexy for wandering spleen is the ideal treatment, splenectomy is indicated if there is torsion/splenic infarction [13,14].
Conclusion(s)
Gastric volvulus is rarely associated with wandering spleen which may lead to splenic torsion. We should keep in mind the possibility of gastric volvulus and wandering spleen in young patients who present with recurrent episodes of abdominal pain where early diagnosis and timely intervention can prevent mortality.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Feb 19, 2019
Manual Googling: Jan 16, 2020
iThenticate Software: Feb 28, 2020 (11%)
[1]. Warren C, Wallace W, Campbell WJ, Splenic laceration with a twist: A lesson learnt from gastric volvulusAnn R Coll Surg Engl 2012 94(2):e88-89.10.1308/003588412X1317122158897422391367 [Google Scholar] [CrossRef] [PubMed]
[2]. Ooka M, Kohda E, Iizuka Y, Nagamoto M, Ishii T, Saida Y, Wandering spleen with gastric volvulus and intestinal non rotation in an adult male patientActa Radiol Short Rep 2013 2(7):01-04.10.1177/204798161349975524349711 [Google Scholar] [CrossRef] [PubMed]
[3]. Flores-Rios E, Méndez-Díaz C, Rodríguez-García E, Pérez-Ramos T, Wandering spleen, gastric and pancreatic volvulus and right sided descending and sigmoid colonJ Radiol Case Rep 2015 9(10):18-25.10.3941/jrcr.v9i10.247526629290 [Google Scholar] [CrossRef] [PubMed]
[4]. Shukla RM, Mandal KC, Maitra S, Ray A, Sarkar R, Mukhopadhyay B, Gastric volvulus with partial and complete gastric necrosisJournal of Indian Association of Paediatric Surgeons 2014 19(1):49-51.10.4103/0971-9261.12596824604987 [Google Scholar] [CrossRef] [PubMed]
[5]. Sharma A, Salerno G, A torted wandering spleen: A case reportJ Med Case Rep 2014 8(1):13310.1186/1752-1947-8-13324886115 [Google Scholar] [CrossRef] [PubMed]
[6]. Yilmaz O, Bayrak V, Daştan E, Kotan C, Torsion of wandering spleen as a rare reason for acute abdomen; A presentation of two casesUlus Cer Derg 2013 29(4):200-02.10.5152/UCD.2013.4725931877 [Google Scholar] [CrossRef] [PubMed]
[7]. Omata J, Utsunomiya K, Kajiwara Y, Takahata R, Miyasaka N, Sugasawa H, Acute gastric volvulus associated with wandering spleen in an adult treated laparoscopically after endoscopic reduction: A case reportSurg Case Rep 2016 2:14710.1186/s40792-016-0175-027221130 [Google Scholar] [CrossRef] [PubMed]
[8]. Anyfantakis D, Kastanakis M, Katsougris N, Papadomichelakis A, Petrakis G, Bobolakis E, Acute torsion of a wandering spleen in a postpartum female: A case reportInt J Surg Case Rep 2013 4(8):675-77.10.1016/j.ijscr.2013.05.00223792478 [Google Scholar] [CrossRef] [PubMed]
[9]. Leci-Tahiri L, Tahiri A, Bajrami R, Maxhuni M, Acute abdomen due to torsion of the wandering spleen in a patient with Marfan SyndromeWorld J Emerg Surg 2013 8(1):3010.1186/1749-7922-8-3023915457 [Google Scholar] [CrossRef] [PubMed]
[10]. Farag S, Fiallo V, Nash S, Navab F, Gastric perforation in a case of gastric volvulusAm J Gastroenterol 1996 91(9):1863-64. [Google Scholar]
[11]. Lianos G, Vlachos K, Papakonstantinou N, Katsios C, Baltogiannis G, Godevenos D, Gastric volvulus and wandering spleen: A rare surgical emergencyCase Reports in Surgery 2013 2013:5617524 pages10.1155/2013/56175223476875 [Google Scholar] [CrossRef] [PubMed]
[12]. Gorsi U, Bhatia A, Gupta R, Bharathi S, Khandelwal N, Pancreatic volvulus with wandering spleen and gastric volvulus: An unusual triad for acute abdomen in a surgical emergencySaudi J Gastroenterol 2014 20(3):195-98.10.4103/1319-3767.13302624976284 [Google Scholar] [CrossRef] [PubMed]
[13]. Lam Y, Yuen KK, Chong LC, Acute torsion of a wandering spleenHong Kong Med J 2012 18:160-62. [Google Scholar]
[14]. Dahiva N, Karthikeyan D, Vijay S, Kumar T, Vaid M, Wandering spleen: Unusual presentation and course of eventsAbdom Imaging 2002 12(3):359-62. [Google Scholar]