Comparison of Static Conformal Beam and Intensity Modulated Radiation Therapy for Intracranial Stereotactic Radiosurgery
Pramod Kumar Gupta1, SA Yoganathan2, KJ Maria Das3, Shaleen Kumar4
1 Assistant Professor, Department of Radiation Oncology, Super Speciality Cancer Institute and Hospital, Lucknow, Uttar Pradesh, India.
2 Medical Physicist (Scientist-1), Department of Radiotherapy, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, Uttar Pradesh, India.
3 Professor, Department of Radiotherapy, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, Uttar Pradesh, India.
4 Professor, Department of Radiation Oncology, Super Speciality Cancer Institute and Hospital, Lucknow, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Pramod Kumar Gupta, Department of Radiation Oncology, Super Speciality Cancer Institute and Hospital, Lucknow, Uttar Pradesh, India.
E-mail: drpkg_kgmu@yahoo.co.in
Introduction
Stereotactic Radiosurgery (SRS) by high end Linear Accelerator is very common. There are different treatment planning and delivery options for doing Linear accelerator based SRS namely by Conformal beam or dynamic conformal arc or Intensity Modulated Radiotherapy (IMRT).
Aim
To perform a dosimetric comparison between the static conformal beam and fixed field IMRT for intracranial SRS planning.
Materials and Methods
A retrospective study was conducted in which four patients treated for single lesion brain metastasis by frame-based SRS (18 Gy) on a 6 MV linear accelerator equipped with microMLC (3 mm) were included. All these patients were planned using BrianLAB iPlan system (PBC algorithm with heterogeneity correction) using 9-14 non-coplanar static conformal fields. For each case, fixed-field IMRT plans were also generated using the same field arrangement. Target coverage V95% (target volume receiving 95% dose) and D95 (dose to 95% target volume), normal tissue sparing 80% dose volume (V80%), 50% dose volume (V50%) and 25% dose volume (V25%) and treatment efficiency (total Monitor Units (MU)) were compared between conformal fields and IMRT.
Results
The median target volume for all the lesions was 10.67cc, range 2.90-28.85 cc. Target coverage of conformal beam and IMRT was almost similar (p=0.78). V95% and D95 of conformal beam plan were 96.9±1.7 % and 17.4±0.3 Gy; whereas the readings for IMRT were 98.9±1.6 and 17.7±0.3 Gy, respectively (p=0.18). V80%, V50% and V25% of conformal beam plan were 21.9±18.5cc, 41.1±33.4cc, and 121.5±89.3cc, respectively; on contrary the same for IMRT were 23.9±18.5cc, 45.8±33.8cc, and 122.5±94.5cc. (p= 0.11) When comparing the treatment efficiency, the conformal beam plan resulted in a significantly smaller total MU. The total MU of conformal beam plan was 3080.5±306.8 MU (median: 3172.5 MU); whereas the same for IMRT was 4905.3±360.1 MU (median: 5034 MU) (p=0.04).
Conclusion
Conformal beam SRS planning is no different from fixed field IMRT plan in terms of target coverage and normal tissue sparing; however conformal beam plan resulted in a significantly smaller total MU which may have a clinical impact.
Dosimetric comparison, Fixed-field intensity modulated radiotherapy planning, Monitor units, Target coverage
Introduction
The SRS refers to precise, conformal and focused delivery of high dose of radiation in a single session to an intra or extra-cranial target while minimising the dose to surrounding normal tissues [1,2]. There are 3 main types of machines that can do SRS treatment; CyberKnife, GammaKnife and high-end Linear Accelerator. SRS by high-end Linear Accelerator is very common in practice throughout the world. Further, there are different treatment planning and delivery options for doing Linear accelerator-based SRS namely by Conformal beam or dynamic conformal arc or IMRT (fixed field/Arc). Linear accelerators having a Multileaf Collimator (MLC) allow the use of noncircular apertures, resulting in more conformal dose distributions to target tissue sparing organs at risk. Conformal beam and IMRT (fixed field/Arc) are the most common types of SRS planning [3-8]. Minimal literature is available to compare the use of fixed-field IMRT with static conformal beam SRS planning, hence the present study was carried out with an aim to perform a dosimetric comparison between static conformal beam and fixed field IMRT for intracranial SRS planning in terms of Target coverage, normal tissue sparing and treatment efficiency (total MU).
Materials and Methods
A retrospective study was conducted in which four consecutive patients treated within the department between June 2008-June 2010 were taken. Consent for intracranial SRS treatment was taken from each patient according to department and institute protocol. Metastatic infiltrating ductal carcinoma or adenocarcinoma of breast or lung primary with single lesion brain metastasis treated by frame-based SRS (18 Gy) on a 6 MV linear accelerator equipped with microMLC (3 mm) were included in the study. Patients with multiple brain metastasis or brain primary were excluded.
All patients were planned using BrianLAB iPlan system (PBC algorithm with heterogeneity correction) using 9-14 non-coplanar static conformal fields. For each case, fixed-field IMRT plans were also generated using the same field arrangement. For Target coverage V95% (target volume receiving 95% dose) & D95 (dose to 95% target volume), Dmax (Gy) and Dmin (Gy) were compared. To see normal tissue sparing 90% dose volume (V90%), 80% dose volume (V80%), 50% dose volume (V50%) and 25% dose volume (V25%) and treatment efficiency (total MU) were compared between static conformal fields and fixed field IMRT plans.
Statistical Analysis
Statistical analysis was done using the Statistical Package for the Social Sciences; (SPSS) IBM Corporation, New York, USA) version 22. A two tailed paired t-test was used to analyse the differences between the static conformal beam and fixed field IMRT plans. p-value <0.05 was considered as significant.
Results
In present study, the median target volume for all the lesions was 10.67cc, range 2.90-28.85 cc. Target coverage of conformal beam and IMRT was almost similar (p=0.78) V95% and D95 of conformal beam plan were 96.9±1.7 % and 17.4±0.3 Gy; whereas the same for IMRT was 98.9±1.6 and 17.7±0.3 Gy, respectively (p=0.18,0.36). V80%, V50% and V25% of conformal beam plan were 21.9±18.5cc, 41.1±33.4cc, and 121.5±89.3cc, respectively; on contrary the same for IMRT were 23.9±18.5cc, 45.8±3.8cc, and 122.5±94.5cc. (p=0.11, 0.09, 0.08, respectively.) When comparing the treatment efficiency, the conformal beam plan resulted in a significantly smaller total MU. The total MU of conformal beam plan was 3080.5±306.8 MU (median: 3172.5 MU); whereas the same for IMRT was 4905.3±360.1 MU (median: 5034 MU) (p=0.04) [Table/Fig-1].
Target coverage, normal tissue sparing and treatment efficiency (total MU) values obtained from the analysed metrics.
| | Patient-1 | Patient-2 | Patient-3 | Patient-4 | All Patients (n=4) | p-value |
|---|
| | Conformal beam | IMRT | Conformal beam | IMRT | Conformal beam | IMRT | Conformal beam | IMRT | Conformal beam | IMRT | |
| Target | Target vol (cc) | 13.081 | 13.081 | 28.85 | 28.85 | 8.252 | 8.252 | 2.904 | 2.904 | 10.67cc (median) | 10.67cc (median) | 0.78 |
| V95 (%) | 94.9 | 99.9 | 98.5 | 99.6 | 96 | 96.5 | 98.1 | 99.4 | 96.9±1.7 | 98.9±1.6 | 0.18 |
| D95 (Gy) | 17.2 | 17.34 | 17.78 | 17.86 | 17.14 | 17.23 | 17.4 | 17.7 | 17.4±0.3 | 17.7±0.3 | 0.36 |
| Dmax (Gy) | 19.5 | 19.75 | 19.55 | 18.9 | 19.39 | 18.38 | 19.63 | 19.26 | 19.52±0.5 | 19.07±0.7 | 0.38 |
| Dmin (Gy) | 13.92 | 16.85 | 14.23 | 15.53 | 14.6 | 15.28 | 15.07 | 15.51 | 14.46±0.4 | 15.79±0.5 | 0.14 |
| Normal tissue (in cc) | V90 | 16.7 | 20.415 | 39.294 | 39.325 | 10.407 | 11.122 | 4.05 | 4.372 | 17.61±.6.6 | 18.81±6.9 | 0.12 |
| V80 | 20.968 | 26.49 | 47.873 | 48.64 | 13.25 | 14.618 | 5.391 | 5.819 | 21.9±18.5 | 23.9±18.5 | 0.11 |
| V50 | 40.04 | 51.117 | 87.848 | 91.997 | 25.561 | 28.206 | 10.795 | 11.828 | 41.1±33.4 | 45.8±33.8 | 0.09 |
| V25 | 167.083 | 134.3 | 222.679 | 249.18 | 68.616 | 75.636 | 27.49 | 30.695 | 121.5±89.3 | 122.5±94.5 | 0.08 |
| Plan parameters | No Fields | 9 | 9 | 14 | 14 | 12 | 12 | 11 | 11 | 11±1 | 11±1 | 0.80 |
| Total MU | 3295 | 5124 | 2658 | 5168 | 3050 | 4385 | 3319 | 4944 | 3080.5±306.8 | 4905.3±360.1 | 0.04 |
A two tailed paired t-test was used
Discussion
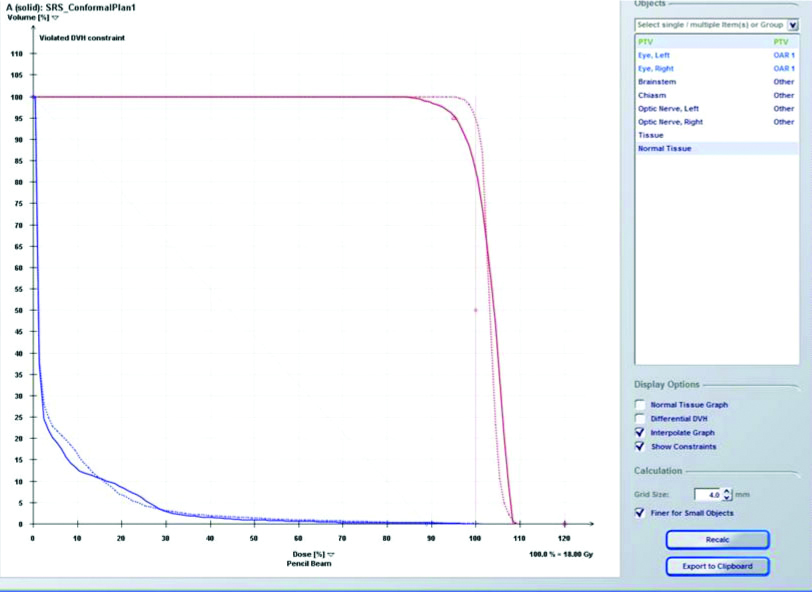
In present study, the target volume was same for both plans making it more objective for the comparison of both plans. Target coverage of the conformal beam and IMRT plans were similar with no statistically significant difference [Table/Fig-2]. In a conformal beam plan, conformally shaped photon beams are placed on a single isocenter with avoidance of the overlapping volumes between the entrance and exit beam [9-11]. Marks LB et al., and Bourland JD and McCollough KP, have shown that using manual beam placement with several equally-spaced coplanar beams good conformity can be achieved [10,12]. However, manually placing non-coplanar beams often becomes difficult. Static field IMRT plan is delivered using, automatic, iterative beam placement and optimisation to modulate the radiation beam [9-13]. In present study, no statistical significant difference between static conformal beam and fixed-field IMRT plan was found for target volume V95 (%), D95 (Gy), Dmax (Gy), Dmin (Gy) and for normal tissue V90, V80, V50, V25 [Table/Fig-3,4].
Dose Volume Histogram comparison of static conformal beam and Fixed field Intensity Modulated Radiation Therapy SRS planning.
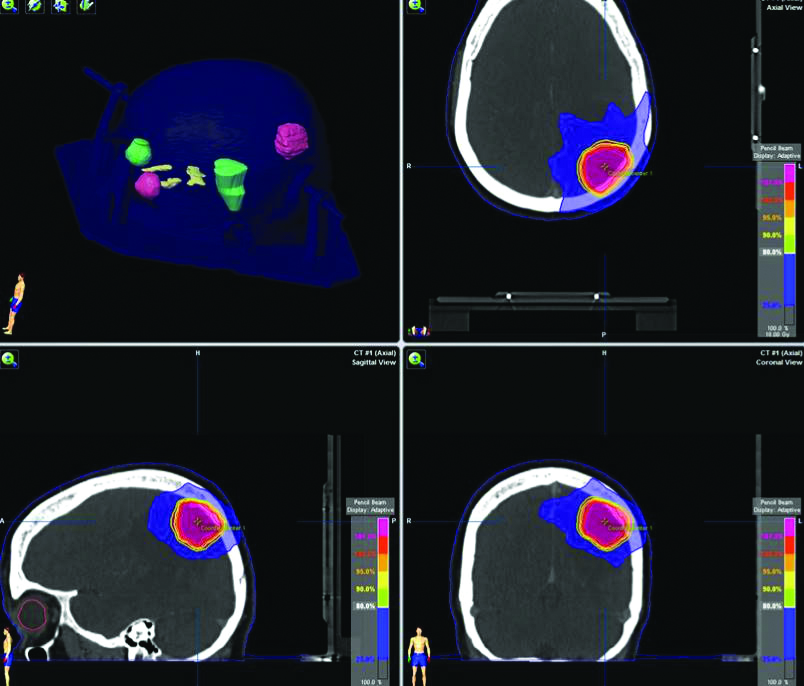
Dose colour wash of static conformal beam SRS Planning.
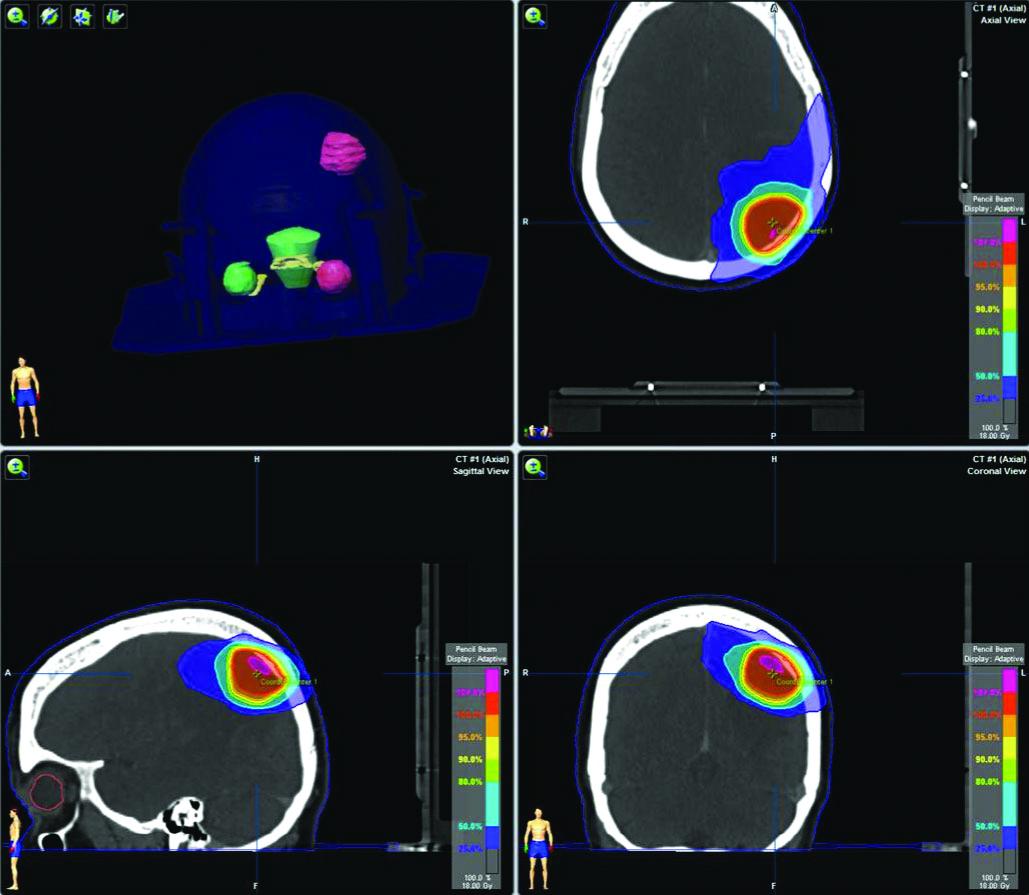
Dose colour wash of Fixed field Intensity Modulated Radiation Therapy SRS planning.
Little DJ et al., in their study have found that IMRT plans improved conformity for the majority of patients but did not significantly improve conformity for the entire patient group. The mean 50% CI was 11.1 for Conformal beam plans vs. 9.1 for IMRT plans (p 0.001) [14]. In present study comparison of the treatment efficiency showed that the conformal beam plan resulted in significantly smaller total MU as compared to fixed-field IMRT SRS plan which may have a clinical impact later on. This is in agreement with previous studies using static conformal or dynamic conformal arc fields [14-18]. Present study finding is supported by study by previous study Woo SY et al. They have shown that a conventional radiosurgery planning is no different from intensity modulated planning for a single small target [15].
Limitation(s)
It was a retrospective study with only 4 patients with 4 intracranial lesions. A larger prospective study should be done to validate the findings of this study.
Conclusion(s)
The results of the present study indicate that fixed field IMRT plan was similar to conformal beam SRS planning in terms of target coverage and normal tissue sparing; however later is associated with higher MU delivery which may have a clinical impact. The present study findings may be useful for the centres who want to start intracranial SRS treatment plans using the BrianLAB iPlan system (PBC algorithm with heterogeneity correction) using 9-14 non-coplanar static conformal fields.
A two tailed paired t-test was used
Author Declaration:
Financial or Other Competing Interests: None
Was Ethics Committee Approval obtained for this study? No
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. NA
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jan 11, 2020
Manual Googling: Feb 08, 2020
iThenticate Software: Feb 24, 2020 (11%)
[1]. Leksell L, The stereotaxic method and radiosurgery of the brainActa Chir Scand 1951 102(4):316-19. [Google Scholar]
[2]. Meeks SL, Pukala J, Ramakrishna N, Willoughby TR, Bova FJ, Radiosurgery technology development and useJ Radiosurg SBRT 2011 1(1):21-29. [Google Scholar]
[3]. Smyth G, Evans PM, Bamber JC, Bedford JL, Recent developments in non-coplanar radiotherapyBr J Radiol 2019 92:2018090810.1259/bjr.2018090830694086 [Google Scholar] [CrossRef] [PubMed]
[4]. Kramer BA, Wazer DE, Engler MJ, Tsai JS, Ling MN, Dosimetric comparison of stereotactic radiosurgery to intensity modulated radiotherapyRadiat Oncol Investig 1998 6:18-25.10.1002/(SICI)1520-6823(1998)6:1<18::AID-ROI3>3.0.CO;2-L [Google Scholar] [CrossRef]
[5]. Benedict SH, Cardinale RM, Wu Q, Zwicker RD, Broaddus WC, Mohan R, Intensity-modulated stereotactic radiosurgery using dynamic micro-multileaf collimationInt J Radiat Oncol Biol Phys 2001 50:751-58.10.1016/S0360-3016(01)01487-0 [Google Scholar] [CrossRef]
[6]. Ernst-Stecken A, Lambrecht U, Ganslandt O, Mueller R, Fahlbusch R, Sauer R, Radiosurgery of small skull-base lesions. No advantage for intensity-modulated stereotactic radiosurgery versus conformal arc techniqueStrahlenther Onkol 2005 181:336-44.10.1007/s00066-005-1371-115900431 [Google Scholar] [CrossRef] [PubMed]
[7]. Gevaert T, Levivier M, Lacornerie T, Verellen D, Engels B, Reynaert N, Dosimetric comparison of different treatment modalities for stereotactic radiosurgery of arteriovenous malformations and acoustic neuromasRadiother Oncol 2013 106:192-97.10.1016/j.radonc.2012.07.00222884842 [Google Scholar] [CrossRef] [PubMed]
[8]. Clark B, McKenzie M, Robar J, Vollans E, Candish C, Toyota B, Does intensity modulation improve healthy tissue sparing in stereotactic radiosurgery of complex arteriovenous malformations?Med Dosim 2007 32:172-80.10.1016/j.meddos.2006.12.00217707196 [Google Scholar] [CrossRef] [PubMed]
[9]. Das SK, Marks LB, Selection of coplanar or noncoplanar beams using three-dimensional optimization based on maximum beam separation and minimised nontarget irradiationInt J Radiat Oncol Biol Phys 1997 38(3):643-55.10.1016/S0360-3016(97)89489-8 [Google Scholar] [CrossRef]
[10]. Marks LB, Sherouse GW, Das S, Bentel GC, Spencer DP, Turner D, Conformal radiation therapy with fixed shaped coplanar or noncoplanar radiation beam bouquets: a possible alternative to radiosurgeryInt J Radiat Oncol Biol Phys 1995 33(5):1209-19.10.1016/0360-3016(95)02084-5 [Google Scholar] [CrossRef]
[11]. Wagner TH, Meeks SL, Bova FJ, Friedman WA, Buatti JM, Bouchet LG, Isotropic beam bouquets for shaped beam linear accelerator radiosurgeryPhys Med Biol 2001 46(10):2571-86.10.1088/0031-9155/46/10/30511686276 [Google Scholar] [CrossRef] [PubMed]
[12]. Bourland JD, McCollough KP, Static field conformal stereotactic radiosurgery: Physical techniquesInt J Radiat Oncol Biol Phys 1994 28(2):471-79.10.1016/0360-3016(94)90074-4 [Google Scholar] [CrossRef]
[13]. Solberg TD, Boedeker KL, Fogg R, Selch MT, DeSalles AA, Dynamic arc radiosurgery field shaping: A comparison with static field conformal and noncoplanar circular arcsInt J Radiat Oncol Biol Phys 2001 49:1481-91.10.1016/S0360-3016(00)01537-6 [Google Scholar] [CrossRef]
[14]. Little DJ, Chang MF, Lii EL, Maor MH, Shiu AS, Comparison of intensity-modulated and shaped beam conformal stereotactic radiotherapy plans for complex intracranial lesionsInt J Radiat Oncol Biol Phys 2003 57:S37610.1016/S0360-3016(03)01292-6 [Google Scholar] [CrossRef]
[15]. Woo SY, Grant WH, Bellezza D, Grossman R, Gildenberg P, Carpentar LS, A comparison of intensity modulated conformal therapy with a conventional external beam stereotactic radiosurgery system for the treatment of single and multiple intracranial lesionsInt J Radiat Oncol Biol Phys 1996 35:593-97.10.1016/S0360-3016(96)80023-X [Google Scholar] [CrossRef]
[16]. Calvo-Ortega JF, Delgado D, Moragues S, Pozo M, Casals J, Dosimetric comparison of intensity modulated radiosurgery with dynamic conformal arc radiosurgery for small cranial lesionsJ Can Res Ther 2016 12:852-57.10.4103/0973-1482.16368027461663 [Google Scholar] [CrossRef] [PubMed]
[17]. Wiggenraad RG, Petoukhova AL, Versluis L, van Santvoort JP, Stereotactic radiotherapy of intracranial tumors: A comparison of intensity-modulated radiotherapy and dynamic conformal arcInt J Radiat Oncol Biol Phys 2009 74:1018-26.10.1016/j.ijrobp.2008.09.05719217219 [Google Scholar] [CrossRef] [PubMed]
[18]. Sarkar B, Pradhan A, Munshi A, Do technological advances in linear accelerators improve dosimetric outcomes in stereotaxy? A head-on comparison of seven linear accelerators using volumetric modulated arc therapy-based stereotactic planningIndian J Cancer 2016 53(1):166-73.10.4103/0019-509X.18081527146771 [Google Scholar] [CrossRef] [PubMed]