Correlation of Auditory Event Related Potential (P300) and Mini Mental State Examination to Measure Cognitive Function in Healthy Young Adults: A Pilot Study
Jitender Sorout1, Sudhanshu Kacker2, Neha Saboo3, Harsha Soni4
1 Student, RUHS College of Medical Sciences, Jaipur, Rajasthan, India.
2 Professor, Department of Physiology, RUHS College of Medical Sciences, Jaipur, Rajasthan, India.
3 Assistant Professor, Department of Physiology, RUHS College of Medical Sciences, Jaipur, Rajasthan, India.
4 Postgraduate, Department of Physiology, RUHS College of Medical Sciences, Jaipur, Rajasthan, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Sudhanshu Kacker, Professor, Department of Physiology, RUHS College of Medical Sciences, Jaipur, Rajasthan, India.
E-mail: sudhanshukacker@gmail.com
Introduction
Cognition is composed of intellectual function, memory, speech and language, complex perception, orientation, attention, judgment, planning and decision-making. Behaviour is the exhibition of these cognitive functions. Cognitive function can be assessed by different methods. The most commonly used are P300 and Mini Mental State Examination (MMSE). As both measures evaluate cognitive functions but objective method P300 evaluate endogenously and give the best picture of cognitive functions.
Aim
To check the correlation between the results of MMSE with event related potential (P300).
Materials and Methods
A prospective cross-sectional study was done on 100 healthy young adult subjects of both genders, aged between 18-25 years after taking written informed consent from January 2019 to June 2019. Cognitive functions were assessed by using MMSE questionnaire through face to face interview and event related potential (P300) latency and amplitude were assessed by using octopus NCV/EMG/EP- 4 Ch. Machine (model- CMEMG 01). Pearson correlation was performed to identify correlation.
Results
The mean MMSE score was 24.28±2.89. The mean P300 (latency and amplitude) was 269.61±43.11 ms and 3.1±4.13 μV. Pearson correlation were used to calculate the correlation between P300 (latency and amplitude) with MMSE. The inverse correlation (-0.086) was in between P300 latency and MMSE. There was no correlation between P300 amplitude and MMSE.
Conclusion
There was no correlation established between P300 amplitude and MMSE and inverse correlation was seen between P300 latency and MMSE. Hence, P300 cannot replace the MMSE in clinical settings.
Cognition, Event related potential, Mini mental state examination
Introduction
The higher-order capacities of the human brain can be captured under the terms cognition and behaviour. Cognition is composed of intellectual function, memory, speech and language, complex perception, orientation, attention, judgment, planning and decision-making. Behaviour is the exhibition of these cognitive functions [1]. Cognitive functions play a critical role in everyday activity and these changes during lifetime and it usually improves as person grows [2]. During the age of 20s or 30s, some cognitive functions such as executive functions and working memory are at the peak. There are numerous conditions in which Cognitive functions get affected like in ageing, stress and in sleep disturbance and in certain diseases like hypertension, dementia, Parkinson’s disease, diabetes etc. Perceived cognitive impairment can hamper the daily living activities [3,4]. Previous studies have demonstrated that higher cognitive functions in children and young adults are positively correlated with higher academic achievements [5,6].
Cognitive function can be assessed by the different methods. The most commonly used are P300 and MMSE. P300 is a sensitive tool for monitoring cognition and maybe an indicator in the analysis of cognitive deterioration [7-10]. P300 latency and amplitude are often considered to be importantly related to higher cortical functioning. A decrease in amplitude and increase in latency corresponds to cognitive decrement. The MMSE is a brief cognitive screening instrument frequently used to evaluate cognitive disorders. It is a subjective method of cognition assessment tool. This comprises of 11 questions and assesses 6 cognitive functional areas: awareness, focus, immediate memory, short-term recall, vocabulary, and ability to follow basic verbal and written commands. The assessment is developed as a standardised instrument which offers a total score that allows the patient to be put on a cognitive functional scale. Each MMSE-evaluated cognitive function has related brain structures that are responsible for this function. While MMSE is not a diagnostic but a screening tool, it maybe helpful for medical students, residents, and clinicians to have a better overall understanding of what specific brain area has been tested while MMSE administers specific cognitive tasks [11]. During the assessment of cognitive functions, the subject is asked simple questions and problems in a number of areas, the time and place of test, repeating lists of words, arithmetic such as serial sevens, language use and comprehension and basic motor skill. Maximum score is 30 and scores <24 are associated with cognitive impairment [12].
As both measures evaluate cognitive functions, but objective method P300 evaluate endogenously and give best picture of cognitive functions. However, it is not possible to use this method in daily clinical setups due to its high cost and practical expertise. So through this study, the present authors tried to set-up a correlation between the results of commonly used cognitive status assessment test, MMSE with event related potential (P300).
Materials and Methods
A pilot study was conducted on a single group of 100 healthy young adults. Subjects of both genders; aged between 18-25 years were recruited for the study after taking written informed consent. The study was approved by the Institutional Ethical Committee (EC/P-47/2018) of RUHS College of Medical Sciences, Jaipur, Rajasthan, India. The duration of study was six months from January 2019 to June 2019. The subjects of Neuropsychological, hearing, cardio-respiratory disorders and use of alcohol, smoking, drugs, and taking sedative or sleeping pills were excluded from the study.
Anthropometric Measurements
Weight and height were measured in accordance with National Health and Nutrition Examination Survey (NHANES) anthropometric measuring guidelines with help of weighing machine and stadiometer [13].
Mini Mental State Examination (MMSE) [
11]
Mini Mental State Examination (MMSE) is a brief cognitive function assessment tool introduced by Folstein MF in 1975 [11]. It consists of 11-questions, which evaluate 6 areas of cognitive functions: orientation, registration, attention, recall, calculation and language. MMSE is divided into two sections, the first of which requires vocal responses only and covers orientation, memory, and attention; the maximum score is 21. The second part tests ability to name, follow verbal and written commands, write a sentence spontaneously, and copy a complex polygon similar to a Bender-Gestalt Figure; the maximum score is 9. So the total score is 30. Questions were asked through face-to-face interview. The mean scores were recorded and analysed. Score ‘0’ was given for the following reasons: Incorrect response, I don’t know. And score ‘1’ was given for each correct answer.
Event Related Potential (P300)
Whole test procedure was conducted in a silent acoustic environment at Neurophysiology lab of Department of Physiology.
Moreover, instructions for the last 24-hours were given to the participants to refrain from consuming caffeinated products and excessive physical activity as these can also contribute to changes in P300 wave. The data of all the subjects were collected at the same time (8-10 am) of day. They were instructed to sit comfortably to close their eyes and not to sleep during the whole test procedure [14]. The scalp was cleaned properly for decreasing the resistance. Then electrodes were placed with the help of conducting paste that’s so why conductivity increases. Ag-AgCl disc electrodes were used for recording. Common reference electrode was placed on Cz position of scalp for active electrodes. Two active electrodes were placed on each mastoid process (A1 and A2). Ground was placed on Fpz position. Subjects were also asked to wear a headphone, through which they heard the rare and frequent sound of different loudness or pitch. And subjects were instructed to recognise the rarer type of the sound and raise the finger with the dominant hand each time they heard it. The auditory Event Related Potential (ERP) were recorded during a task involving standard auditory oddball paradigm on Octopus NCV/EMG/EP- 4 Ch. Machine (model- CMEMG 01). Auditory ERPs were recorded at the standard settings. Environmental factors which influence ERP such as temperature, noise, or strong luminosity were controlled during each recording.
The subjects were asked to come in the morning or 2-3 hours after the last meal. The subjects were asked not to take any medication before the test and refrain from sedative drugs or caffeinated products, excessive exercise 24 hours before the test. Then test protocol was explained to the subject and demonstrated the same. Test procedure was conducted in a silent acoustic room. Pearson’s correlation analysis was performed to access the correlation between auditory event related potential and MMSE by using Microsoft excel 2007.
Results
A total of 100 subjects (75 males and 25 females) with (mean age=19.81±1.80 years, mean weight=68.52±12.89 kg, mean height=170.03±8.66 cm. and mean BMI=21.99±4.21 (kg/m2) was assessed for MMSE and ERP (P300) [Table/Fig-1,2].
Distribution of demographic data.
| Veriables | Mean±SD |
|---|
| Age (year) | 19.81±1.80 |
| Weight (kg) | 68.52±12.89 |
| Height (cm) | 170.03±8.66 |
| BMI (kg/m2) | 21.99±4.21 |
Mean and SD scores for MMSE and Event Related Potential (P300 latency and amplitude).
| Test | Mean | SD |
|---|
| MMSE | 24.28 | 2.89 |
| P300 lat (ms) | 269.61 | 43.11 |
| P300 amp (μV) | 3.1 | 4.13 |
The distribution of data was normal. Pearson’s correlation was calculated assess the association between the MMSE and auditory event related potential P300 i.e., wave latency and amplitude [Table/Fig-3,4].
Correlation between MMSE and Auditory ERP (P300) latency and amplitude.
| MMSE |
|---|
| P300 lat (ms) | -0.086 | p=0.39 |
| P300 amp (μV) | -0.0103 | p=0.91 |
Pearson correlation coefficient between MMSE and P300 latency showing poor inverse association (r=-0.086, p>0.05).
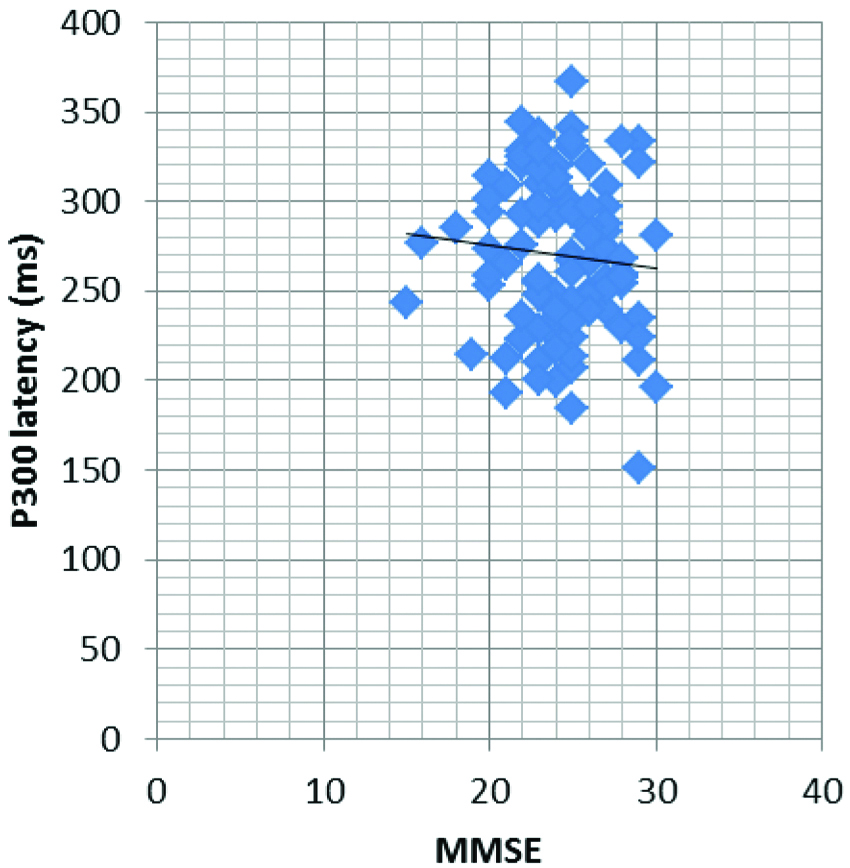
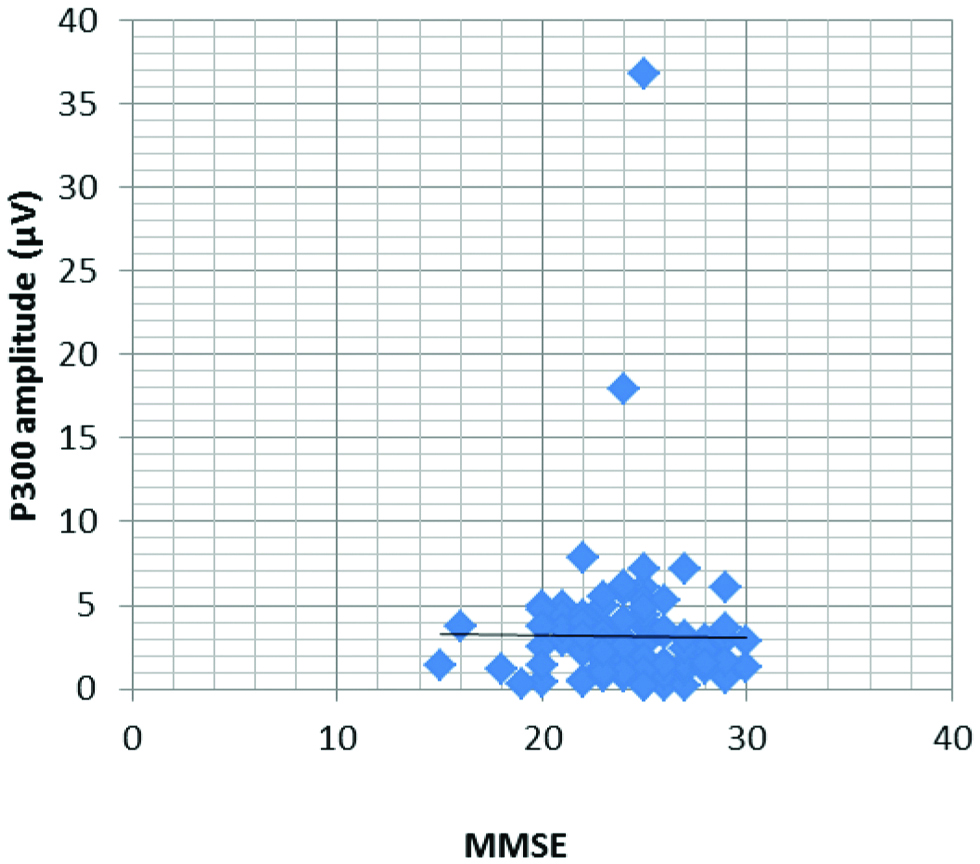
Interestingly inverse poor correlation were found between latency of P300 and MMSE score; representing that when MMSE score increases the latency time decreases. The relationship between MMSE and P300 amplitude was calculated but didn’t show any association [Table/Fig-3,5].
Pearson correlation coefficient between MMSE and P300 amplitude showing no association (r=-0.0103, p>0.05).
Discussion
In the present cross-sectional study, the present authors correlate the two cognitive function assessing tests in healthy young adults. MMSE and auditory ERP (P300) were used for assessment cognition. Various scales are used in clinical or research settings to screen cognitive status at various domains (Appels B 2010) [12,15]. These are paper pencil test, MMSE, Digital Symbol Substitution Test (DSST), Letter Cancellation Task (LCT), Trail Making Test (TMT) and fMRI, Event Related Potential (ERP). The MMSE scale was most commonly used in clinics of India [16].
In this study mean MMSE score was nearby to the cut-off value (MMSE >24) which represent the normality in cognition. Kochhann R et al., reported that the mean MMSE score of young adults was 28.8±0.12, which was higher than present study (24.28±2.89) for higher educational level [17]. The score difference was 4.52±2.77. Gupta PP et al., founded mean MMSE 27.85±1.51 and mean P300 latency was 265.69±15.49 ms in healthy subjects [18]. In this study, the mean P300 latency and amplitude was 269±43.11 ms and 3.1±4.13 μV. which indicates good cognitive status than the present study results.
Kumar N et al., reported that the mean P300 (latency; amplitude) values were as of male (282.04±8.46 ms; 6.01±3.14 μV), female (279.14±9.38 ms; 5.43±3.09 μV) [19]. And Saha S et al., reported the mean P300 latency 307.82±33.87 ms of healthy young adults [20]. Uvaish AN et al., provided normative mean values of P300 latency (358.06±33.79 ms) and amplitude (8.99±4.48 μV) for Indian young adults, which was higher than this present study [21]. Braveman RE suggested that the P300 latency may be an important screening indicator of impaired/borderline memory or dementia [22]. A P300 latency decrement and MMSE score increment shows the better cognitive functions. The present study results showed the inverse poor association between MMSE and P300 latency. However, the results were not significant (p>0.05). Same type of correlation was suggested by Gupta PP et al., study done on 40 healthy volunteers but the results were not significant [18].
Limitation(s)
Small sample size was the limitation for this study.
Conclusion(s)
There was no correlation established between P300 amplitude and MMSE and inverse correlation was seen between P300 latency and MMSE. Hence P300 cannot replace the MMSE in clinical settings. This study also appeal further studies on larger group of individuals should be conducted in young population for best correlation results.
Author Declaration:
Financial or Other Competing Interests: None
Was Ethics Committee Approval obtained for this study? Yes
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. NA
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Nov 05, 2019
Manual Googling: Jan 21, 2020
iThenticate Software: Feb 07, 2020 (15%)
[1]. Evans JJ, Basic concepts and principles of neuropsychological assessmentHandbook of Clinical Neuropsychology 2003 Oxford, UKUniversity Press:15-26.10.1093/acprof:oso/9780199234110.003.0220708670 [Google Scholar] [CrossRef] [PubMed]
[2]. Hedden T, Gabrieli JDE, “Insights into the ageing mind: A view from cognitive neuroscience.”Nat Rev Neurosci 2004 5(2):87-96.10.1038/nrn132314735112 [Google Scholar] [CrossRef] [PubMed]
[3]. Millan JCC, Maseda A, Rochette S, Vazquez GA, Sánchez A, Lorenzo T, Mental and psychological conditions, medical comorbidity and functional limitation: Differential associations in older adults with cognitive impairment, depressive symptoms and coexistence of bothInt J Geriatr Psyc 2011 26(10):1071-79.10.1002/gps.264621905101 [Google Scholar] [CrossRef] [PubMed]
[4]. Johansson MM, Marcusson J, Wressle E, Cognitive impairment and its consequences in everyday life: Experiences of people with mild cognitive impairment or mild dementia and their relativesInt Psychogeriatr 2015 27(6):949-58.10.1017/S104161021500005825644289 [Google Scholar] [CrossRef] [PubMed]
[5]. Rohde TE, Thompson LA, “Predicting academic achievement with cognitive ability.”Intelligence 2007 35(1):83-92.10.1016/j.intell.2006.05.004 [Google Scholar] [CrossRef]
[6]. Bangirana P, Menk J, John CC, Boivin MJ, Hodges JS, The association between cognition and academic performance in Ugandan children surviving malaria with neurological involvementPLoS One 2013 8(2):e5565310.1371/journal.pone.005565323383342 [Google Scholar] [CrossRef] [PubMed]
[7]. Dinteren RV, Arns M, Jongsma MLA, Kessels RPC, P300 development across the lifespan: A systematic review and meta-analysisPLoS One 2014 9(2):01-13.10.1371/journal.pone.008734724551055 [Google Scholar] [CrossRef] [PubMed]
[8]. Vecchio F, Määttä S, The use of auditory event-related potentials in Alzheimer’s disease diagnosisInt J Alzheimers Dis 2011 2011(653173):01-08.10.4061/2011/65317321629759 [Google Scholar] [CrossRef] [PubMed]
[9]. Rossini PM, Rossi S, Babiloni C, Polich J, Clinical neurophysiology of aging brain: From normal aging to neurodegenerationProg Neurobiol 2007 83(6):375-400.10.1016/j.pneurobio.2007.07.01017870229 [Google Scholar] [CrossRef] [PubMed]
[10]. Picton TW, Hillyard SA, Human auditory evoked potentials IIEffects of attention. Electroencephalogr Clin Neurophysiol 1974 36(2):191-99.10.1016/0013-4694(74)90156-4 [Google Scholar] [CrossRef]
[11]. Folstein MF, Folstein SE, McHugh PR, “Mini-mental state: A practical method for grading the cognitive state of patients for the clinician,”J Psychiatr Res 1975 12(3):189-98.10.1016/0022-3956(75)90026-6 [Google Scholar] [CrossRef]
[12]. Shulman KI, Herrmann N, Brodaty H, Chiu H, Lawlor B, Ritchie K, IPA survey of brief cognitive screening instrumentsInt Psychogeriatr 2006 18(2):281-94.10.1017/S104161020500269316466586 [Google Scholar] [CrossRef] [PubMed]
[13]. National Health and Nutrition Examination Survey (NHANES)- Anthropometry Procedures Manual, January 2007 [Google Scholar]
[14]. Lee HJ, Kim L, Kim YK, Suh KY, Han J, Park MK, Auditory event-related potentials and psychological changes during sleep deprivationNeuropsychobiology 2004 50(1):01-05.10.1159/00007793315179012 [Google Scholar] [CrossRef] [PubMed]
[15]. Appels BA, Scherder E, The diagnostic accuracy of dementia-screening instruments with an administration time of 10 to 45 minutes for use in secondary care: A systematic reviewAm J Alzheimer Dis Other Dement 2010 25(4):301-16.10.1177/153331751036748520539025 [Google Scholar] [CrossRef] [PubMed]
[16]. Creavin ST, Wisniewski S, Noel-Storr AH, Trevelyan CM, Hampton T, Rayment D, Mini-Mental State Examination (MMSE) for the detection of dementia in clinically unevaluated people aged 65 and over in community and primary care populationsCochrane Database Syst Rev 2016 13(1):CD01114510.1002/14651858.CD011145.pub226760674 [Google Scholar] [CrossRef] [PubMed]
[17]. Kochhann R, Varela JS, de Macedo Lisboa CS, Chaves MLF, The Mini Mental State Examination: Review of cutoff points adjusted to schooling in a large Southern Brazilian sampleDement and Neuropsychol 2010 4(1):35-41.10.1590/S1980-57642010DN4010000629213658 [Google Scholar] [CrossRef] [PubMed]
[18]. Gupta PP, Sood S, Atreja A, Agarwal D, A comparison of cognitive functions in non-hypoxemic chronic obstructive pulmonary disease (COPD) patients and age-matched healthy volunteers using minimental state examination questionnaire and event-related potential, P300 analysisLung India 2013 30(1):05-11.10.4103/0970-2113.10611923661909 [Google Scholar] [CrossRef] [PubMed]
[19]. Kumar N, Singh M, Sood S, Beena Sakshi Roy PS, Effect of acute moderate exercise on cognitive P300 in persons having sedentary lifestylesInt J Appl Basic Med Res 2012 2(1):67-69.10.4103/2229-516X.9681323776814 [Google Scholar] [CrossRef] [PubMed]
[20]. Saha S, Muradi V, Gowda LBP, Kalra P, A comparative study of event-related potential P300 between normal individuals and individuals with prediabetesNatl J Physiol, Pharm Pharmacol 2018 8(2):171-76.10.5455/njppp.2018.8.0309817082017 [Google Scholar] [CrossRef]
[21]. Uvais NA, Nizamie SH, Das B, Praharaj SK, Katshu MZUH, Auditory P300 event-related potential: Normative data in the Indian populationNeurol India 2018 66(1):176-80.10.4103/0028-3886.22287429322983 [Google Scholar] [CrossRef] [PubMed]
[22]. Braverman RE, Blum K, P300 (latency) Event Related Potential: An accurate predictor of memory impairmentClin Encephalogr 2003 34(3):124-39.10.1177/15500594030340030614521274 [Google Scholar] [CrossRef] [PubMed]