Caution in Interpreting Diethylenetriamine Pentaacetic Acid Renal Scan in Renal Failure
Gautamram Choudhary1, Himanshu Pandey2, Suresh Goyal3, Prateek Gupta4
1 Associate Professor, Department of Urology, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
2 Associate Professor, Department of Urology, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
3 Senior Resident, Department of Urology, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
4 Senior Resident, Department of Urology, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Prateek Gupta, Department of Urology, All India Institute of Medical Sciences, Jodhpur-342005, Rajasthan, India.
E-mail: prateekgupta8@gmail.com
Since the invention and use of dynamic radionuclide renal imaging techniques, the diagnosis of urinary tract obstruction has become easier. Amongst this, diuretic renogram using Technetium 99 m Diethylenetriaminepenta-Acetic acid (99 mTc-DTPA) is the most widely used for detecting upper urinary tract obstruction. This is even widely used amongst paediatric population for its higher diagnostic success. But, even these techniques might misdiagnose or may reveal incomplete data of the renal derangement causing increased morbidity and mortality.
We present a case of a 34-year-old male patient with impaired renal function for which DTPA scan was done twice, which revealed partial obstructive nephropathy with hydronephrosis of left kidney. But a retrograde pyelogram was performed which showed complete obstruction at the upper part of the ureteric segments. This required a robot assisted pelvi-ureteric anastomosis to release the hydronephrosis. Here the DTPA scan findings were misleading on both occasions. This does emphasise the need for an array of investigations to evaluate or exclude any clinical suspicion.
Obstructive nephropathy, Percutaneous nephrostomy, Pelvi-ureteric anastomosis
Case Report
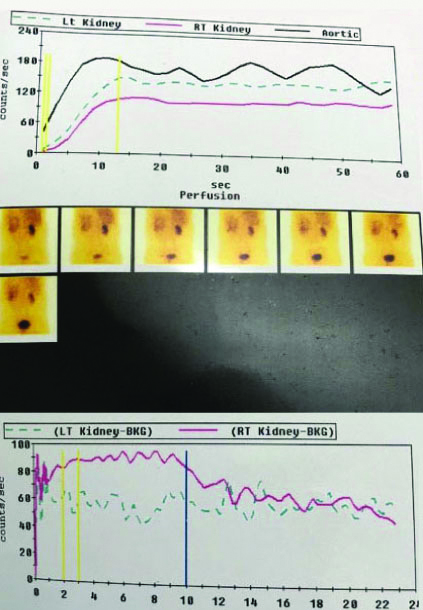
A 34-year-old male patient, with 65 kg body weight, was hospitalised with complaints of vague abdomen pain with elevated serum creatinine values (2.4 mg/dL). In past, right Percutaneous Nephrolithotomy (PCNL) was performed in January 2017 (serum creatinine: 1.3 mg/dL). In March 2017, left PCNL was performed for residual stones and it was repeated again in July 2017 during which the nephrostomy was kept in situ (output: 1000-1300 cc/day). In August 2017, DTPA scan was done (GFR: 15 mL/min out of total 37.69 mL/min) [Table/Fig-1]. This was followed by, left open pyeloplasty in September 2017 and patient was later referred to this hospital for further management.
DTPA renal scan showing partial improvement of function with delayed clearance done on August 2017.
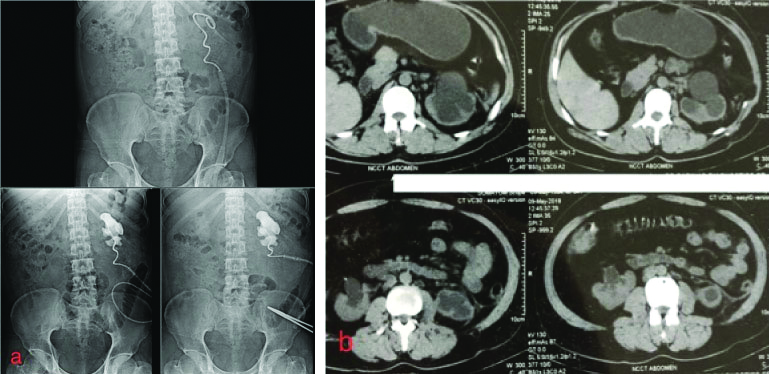
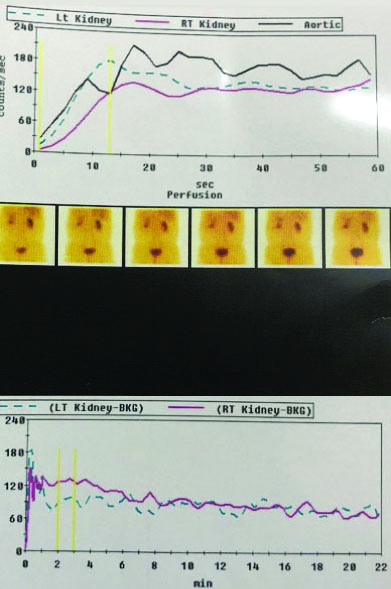
A left Percutaneous Nephrostomy (PCN) was performed, which drained 150-200 cc urine per day. After a month, PCN output increased marginally (200-300 cc per day) and the Nephrostogram revealed complete cut-off at Pelvi-Ureteric Junction (PUJ) level [Table/Fig-2a] with grossly hydronephrotic left kidney [Table/Fig-2b], DTPA renal scan was done again on June 2018 (GFR: 17.9 mL/min out of total 42 mL/min), which revealed partial improvement of function with delayed clearance [Table/Fig-3]. Yet, it was decided to perform a Retrograde Pyelography (RGP) and proceed.
a) Left sided nephrostogram showing complete cut-off at pelvi ureteric junction; b) Non-contrast computed tomography images showing thinned out renal parenchyma and grossly dilated pelvicalyceal system.
DTPA renal scan done on June 2018.
Under general anaesthesia, a left side RGP was performed along with nephrostogram, which showed complete occlusion at the small, upper most ureteric segment. For this, a Robot assisted pelvi-ureteric anastomosis was done with polyglactin 4-0 suture in an interrupted manner and the lower pole of kidney was stitched to psoas muscle.
Discussion
Obstructive nephropathy can pose a threat of partial or complete loss of renal functioning. Hence timely diagnosis is the key which is required for management and protecting the renal parenchyma from permanent destruction. For suspected PUJ obstruction, renal scintigraphy provides differential glomerular function and drainage pattern. Nonetheless, selecting the type of scintigraphy method depends on the serum creatinine level, availability of the test and trend of routine practice. In the present case, the patient had impaired renal function, for whom Technetium 99mDTPA (99mTc-DTPA) method was done twice but it mislead the diagnosis.
Accurate assessment of Glomerular Filtration Rate (GFR) is important in detecting the exact cause of the signs and symptoms, detecting its severity, deciding the management of the condition and assessing the prognosis of the disease [1]. There are certain non-invasive tests such as Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation and Modification of Diet in Renal Disease (MDRD) equation [2]. While there are certain renal dynamic imaging techniques using technetium labelled agents used for renal scintigraphy to estimate GFR, differential renal function and urinary drainage. However, sometimes it is difficult to choose which one is better. As in this case, DTPA scan gave inadequate data while RPG helped in identifying the extent of occlusion. These dynamic imaging techniques have certain benefits as they achieve the data of unilateral renal blood flow and kidney function, they are quick and less time consuming and the outcomes are independent of the diet of the patient [3,4]. The DTPA scan allows having a constant monitoring during the entire scan procedure and provides information not only of the renal functioning but also about the pelvi-ureteric drainage. In these procedures, fewer amounts of radiations are used, hence they have minimum risk of nephrotoxicity [5].
Nevertheless, 99mEthylene di-Cysteine (EC) and 99mTc-Mercaptoacetyltriglycine (MAG3) are better than 99mTc-DTPA in evaluating function and drainage in patients with impaired renal disorders. Also, there are differences in scan quality despite the use of the same radiopharmaceutical, comparable equipment and identical billing [6,7]. Xie P et al., in a study on 149 patients measured GFR by: (a) dual plasma sample clearance method (tGFR); (b) renal 99mTc-DTPA method (dGFR); (c) CKD-EPI equation (eGFR) and patients were categorised into 2 subgroups based on the GFR (GFR <60 and >60) [3]. On comparison of dGFR with eGFR, percentage of eGFRs within 30% and 15% of tGFR was not higher than that of dGFR (71.14% vs 66.44% for 30% accuracy, p=0.419; 48.99% vs 41.61% for 15% accuracy, p=0.207) The precision of eGFR was not significantly lower than that of dGFR (14.34 ml·min-1·(1.73m2)-1 vs 15.39 mL·min-1·(1.73 m2)-1; F=1.152, p=0.831) and they conclude that both CDK-EPI equation and renal dynamic imaging can be used to determine the GFR of CKD patients, CDK-EPI equation is more accurate than renal dynamic imaging.
In another study done by Yildiz G et al., compared estimated GFR (eGFR) calculated with the formulas of Cockcroft-Gault (C&G), MDRD, CKD-EPI and Mayo Clinic Quadratic (Mayo Q) and GFR (mGFR) that was scintigraphically measured with creatinine clearance (CrCl) and 99mTc-DTPA [8]. The values of 99mTc-DTPA based on mGFR were compared with eGFR values of the formulas. Significant correlations were found with the values of 99mTc-DTPA, mGFR, CrCl, MDRD, CKD-EPI, Mayo Q and C&G eGFR. The best estimate was made with MDRD-6 in the cases with 99mTc-DTPA, mGFR was <30 mL/min/1.73 m2 and with MDRD-4 in the cases with 99mTc-DTPA, mGFR was ≥30 mL/min/1.73m2 [4]. These two above mentioned studies and many others suggests that DTPA perform well in diagnosing even in impaired renal function.
But in the above-mentioned case, twice DTPA was performed and at both occasions it failed to detect the pathology thus causing failure in diagnosis. In this case, kidney function deteriorated with time and even the urine output also decreased significantly, however DTPA falsely showed high GFR compared to prior one [Table/Fig-2a,b]. One of the possible reasons for this could be the impaired renal function which reduces the response to the diuretics administered. Due to obstruction, the entire collecting system might be dilated. Hence when the 99mTc-DTPA is passed till 20 minutes post-administration, the chances that the entire collecting system wouldn’t be completely filled with the tracer [4].
But these are just hypothesis which require further clinical trials for confirmation. The urologist plays a key role is analysing the clinical presentation and the investigation values apart from the negative findings on imaging. Multiple and varied imaging tests should be conducted to rule out any possibilities of any false negative results. In this scenario, 99mEC or 99mTc-MAG3 would have been a preferred moiety over 99mTc-DTPA. Creatinine clearance of PCN output could have been performed.
Conclusion(s)
In patients with impaired renal function, renal DTPA can be a non-invasive tool to evaluate renal function; however it has its limitations and should be considered as an adjunctive tool for work-up. Diversion with PCN gives exact urine output of that moiety. Apart from recent advances in scan technique,analysing the clinical and laboratory parameters aid in early diagnosis which could salvage the poorly functioning renal moiety.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Oct 28, 2019
Manual Googling: Jan 23, 2020
iThenticate Software: Feb 12, 2020 (16%)
[1]. Inker LA, Schmid CH, Tighiouart H, Eckfeldt JH, Feldman HI, Greene T, Estimating glomerular filtration rate from serum creatinine and cystatin CN Engl J Med 2012 367(1):20-29.10.1056/NEJMoa111424822762315 [Google Scholar] [CrossRef] [PubMed]
[2]. Gomez Marcos MA, Rodriguez Sanchez E, Recio Rodriguez JI, Martin Cantera M, Ramos Blanes R, Garcia Ortiz L, Differences between the CKD-EPI and the MDRD equations when estimating the glomerular filtration rate in hypertensive patientsNefrologia 2010 30(4):458-62. [Google Scholar]
[3]. Xie P, Huang JM, Liu XM, Wu WJ, Pan LP, Lin HY, (99m)Tc-DTPA renal dynamic imaging method may be unsuitable to be used as the reference method in investigating the validity of CDK-EPI equation for determining glomerular filtration ratePLoS One 2013 8(5):e6232810.1371/journal.pone.006232823658724 [Google Scholar] [CrossRef] [PubMed]
[4]. Lin KJ, Huang JY, Chen YS, Fully automatic region of interest selection in glomerular filtration rate estimation from 99mTc-DTPA renogramJ Digit Imaging 2011 24(6):1010-23.10.1007/s10278-011-9361-621274591 [Google Scholar] [CrossRef] [PubMed]
[5]. Lin CC, Shih BF, Shih SL, Tsai JD, Potential role of Tc-99 m DTPA diuretic renal scan in the diagnosis of calyceal diverticulum in childrenMedicine (Baltimore) 2015 94(24):e98510.1097/MD.000000000000098526091475 [Google Scholar] [CrossRef] [PubMed]
[6]. Taylor AT, Radionuclides in nephrourology, part 1: Radiopharmaceuticals, quality control, and quantitative indicesJ Nucl Med 2014 55(4):608-15.10.2967/jnumed.113.13344724549283 [Google Scholar] [CrossRef] [PubMed]
[7]. Taylor AT, Radionuclides in nephrourology, Part 2: Pitfalls and diagnostic applicationsJ Nucl Med 2014 55(5):786-98.10.2967/jnumed.113.13345424591488 [Google Scholar] [CrossRef] [PubMed]
[8]. Yildiz G, Mağden K, Abdulkerim Y, Ozcicek F, Hür E, Candan F, Glomerular filtration rate: which method should we measure in daily clinical practice?Minerva Med 2013 104(6):613-23. [Google Scholar]