Poor infant and young child nutrition practices are an important contributor to poor nutrition which in turn leads to poor survival outcomes and poor long term outcomes such as school performance and wages in adulthood [1-3]. Undernourished children suffer from ill-health which is associated with over 50% of deaths in the under-five age group [4]. The period between conception and two years is the critical period in a child’s life when interventions to improve nutrition must be delivered [5]. Though Kerala is a state with high female literacy, declining rates of early initiation of breastfeeding and shifting partially or completely to formula feed before the completion of six months of age have been observed according to National Family Health Survey (NFHS) 2007-2008 and District Level Household Survey (DLHS 3) [6,7]. In Ernakulam district where the study was carried out, only 51.8% of newborns were breastfed within one hour of birth and children exclusively breastfed up to six months was only 16.9% in comparison to the state of Kerala statistics of 65.3% and 22.3%, respectively [7]. This is in sharp contrast to the 100% institutional delivery in Ernakulam district and female literacy rate of 90.7% [7].
There is a complex relationship between intrinsic characteristics of the child, competence of the mother in providing child care and social support in determining growth and nutritional outcomes of children [8]. Socio-cultural norms, embedded networks of support influence infant and young child feeding practices [9]. In order for women to be successful in breastfeeding they should have correct information and support for early initiation and maintenance of exclusive breastfeeding [10]. Breastfeeding in India is almost universal but the rate of early initiation of breastfeeding, exclusive breastfeeding up to 6 months and timely complementary feeding are very poor [11]. Breastfeeding is an evidence based intervention that has been found to significantly reduce neonatal and thereby child deaths and provides short-term and long-term economic and environmental advantages to society [9,12].
Breastfeeding protection, promotion and support must be available in the community, and forms an important part of a comprehensive support approach [13]. Hence, addressing these issues through behaviour change communication is important and so is targeting not only mothers of under-three children but also key influencers in the family who are responsible for decisions relating to infant and young child feeding. Studies using Peer counselling methods and behaviour change communication approaches have been successful in improving various aspects of infant and young child feeding [9,14]. However, behaviour change communication approaches through the Integrated Child Development Services (ICDS) unit, Anganwadi has not been considered for the delivery of the intervention to improve breastfeeding, infant and young child feeding practices. The other novelty of the study includes taking the opinion of key influencers in tailoring the behaviour change communication approach.
Therefore, the objectives of the study were to assess the impact of a tailored intervention using the Behaviour Change Communication (BCC) approach on the awareness and practice of initiation of breastfeeding and exclusive breastfeeding among mothers of under-three children and antenatal women. The secondary objectives included assessing the impact of BCC on the awareness and practice of feeding of colostrum, concept of 1000 days, bottle feeding and other IYCF practices.
Materials and Methods
An interventional study was carried out in a coastal, self-administration unit (Njarackal) with a population of 22,596 and 16 wards in Ernakulam district of Kerala, India. The study was of one year duration from December 2011-December 2012 followed by a dissemination workshop in December 2013. A detailed written informed consent was obtained from each of the willing respondents. All aspects of the study were examined by a department committee and also overseen by UNICEF office. This was an educational service project and does not contravene the Helsinki principles.
The study population included mothers of children under three years of age, antenatal women and their influencers in the study area. A before and after interventional study design was carried out. Expecting a 20% increase in initiation of breastfeeding within 1 hour and exclusive breastfeeding based on District level Household-level survey findings the minimum sample size varied from 30-50 with 95% confidence and 80% power [3]. In order to ensure at least 80% coverage of the panchayat, 12 of the 16 wards in the self-administration unit were randomly selected for the study and such listed women in these wards were included in the study. The key influencers were the most important people who influenced the mother in issues relating to pregnancy and childcare. All the included participants signed an informed consent form and the houses that were locked after two visits were excluded from the study.
Intervention
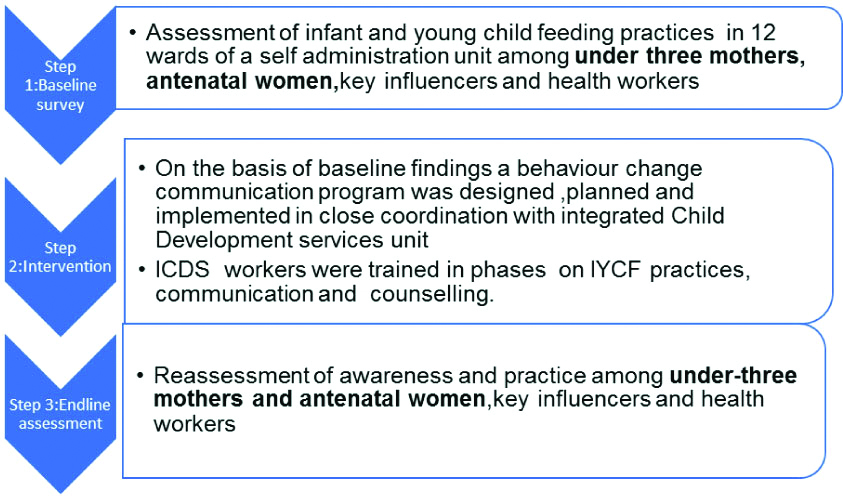
After carrying out a baseline survey a BCC exercise tailored to the findings of the baseline survey was carried out with the following content. The content focused on the 1000 day concept, diet during pregnancy and lactation, initiation of breastfeeding within one hour, exclusive breastfeeding, breastfeeding position and attachment, expressed breast milk, complementary food items, consistency and frequency of feeding, hygiene, feeding during illness, dangers of artificial feeding. The modes of intervention were carried out in close coordination with the local integrated child development services unit (ICDS) in the randomly selected wards. The personnel in the ICDS unit (Anganwadi worker) underwent two-days training on IYCF practices, communication and fundamentals of counselling in a phased manner. Initially, mothers and key influencers meeting were conducted in the Anganwadi with specially designed flip charts, flashcards whose content was tailored to the baseline study findings and intervention content. This was followed by street plays on the key content in each of the wards [Table/Fig-1]. The Anganwadi workers then visited the mothers who were facing difficulty in breastfeeding with a checklist and advised the mothers on breast attachment, necessity to feed at night etc. These messages were reinforced by different methods as like home visits, individual counselling, cable network. The period of intervention was three months which was followed two months later by the endline survey. All the antenatal and under three mothers in the selected area, meeting the inclusion and exclusion criteria were interviewed at baseline and endline. There were 351 mothers with children under three years of age and 87 antenatal women (8 mothers belonged to both categories) at baseline; 361 mothers with children under three years of age and 63 antenatal mothers (11 mothers belonged to both categories) respectively at endline. The follow-up loss was due to travel during school vacations, pregnancy etc. The health workers of the primary health centres in the area were also sensitised on the intervention content. A detailed interview schedule of 75 items for the antenatal mother/pregnant women, 45 items for the influencers and 56 for the health workers were developed for baseline and endline assessment. The baseline and endline assessment consisted of knowledge and practice questions related to the content of the BCC exercise.
Statistical Analysis
Data was entered in MS Excel and analysed on SPSS 20.0. Statistical analysis was carried out by comparison of mean, proportions before and after the study. Mc Nemar’s chi-square was done on variables with significant improvement followed by multivariate logistic regression, p-value <0.05 was considered as level of significance.
Results
The mean age of the mothers was 27.42±4.53 years. The median age of under three children was 1.5 years. The socio-demographic profile of the study population at baseline and endline were comparable with no significant differences [Table/Fig-2].
Socio-demographic characteristics of the population before and after the intervention.
| | Baseline | Endline | |
|---|
| Characterstrics of the participants | | n=430 | n=413 | p-value |
|---|
| Mean age of mother (in years) | | 27.36 | 27.42 | 0.85 |
| Religion | Hindu (%) | 58.75 | 60.3 | 0.65 |
| Christian (%) | 40.4 | 39.4 | 0.77 |
| Muslim (%) | 0.9 | 0.3 | 0.26 |
| Schooling (in years) | 8-10 (%) | 33 | 34.1 | 0.74 |
| 10-12 years (%) | 23.2 | 21.5 | 0.55 |
| Bachelors degree (%) | 26.5 | 31.5 | 0.11 |
| Working status of mothers (%) | | 7.4 | 10.7 | 0.09 |
| Mothers with children under three years of age | | n=351 | n=361 | |
| Mean age of under three children (years) | Median | 1.5 | 1.3 | 0.42 |
| 0-1 years (%) | 38.2 | 42.6 | 0.26 |
| 1.1-3 years (%) | 61.8 | 57.4 | 0.24 |
| Gender of the child | Male (%) | 49.1 | 53 | 0.64 |
| Female (%) | 50.9 | 47 | 0.62 |
Among antenatal mothers, dietary practices, source of antenatal care, intake of Iron and Folic Acid (IFA) and utilisation of Anganwadi services were assessed. All the mothers (an increase from 98.8%) reported consumption of IFA tablets on the day before the visit. There was a 15.6% increase in the number of antenatal mothers who had modified their diet. A substantial proportion modified diet by addition of milk (66.7%), fruits (55.6%), eggs (27.8%). However, though use of pulses and GLV was low at 16.7% and 22.2%, it showed a substantial increase from 8.2% and 4.9%, respectively. Post-intervention, there was a marginal decrease (71.3% to 69.8%) in the percentage of women who had availed antenatal care from private providers. There was a significant increase in knowledge regarding key concepts such as 1000 day concept, initiation and exclusive breastfeeding among the mothers with children under three years of age [Table/Fig-3].
Impact of intervention on awareness of IYCF.
| Parameters | Before | After | p-value |
|---|
| (n=351) | (n=361)* | |
|---|
| No (%) 95%CI | No(%)95% CI | |
|---|
| Initiation within 1 hr | 264 (75.3) 71.31,79.4 | 335 (92.9) 88.9,94.2 | ≤0.001** |
| Exclusive breastfeeding | 318 (90.7) 86.8,92.4 | 344 (95.2) 92.6,96.8 | 0.01** |
| 1000 day concept | 2 (0.5) 0.33,0.79 | 74 (20.6) 22.1,30.5 | 0.001** |
| Breastfeeding options for a working mother | 97 (27.7) 23.2,31.6 | 180 (49.9) 44.36,53.9 | 0.001** |
| Ill effects of bottle feeding | 254 (72.3) 65.5,74.1 | 306 (84.9) 80.1,87.2 | 0.001** |
| Ill effects of commercial feeding | 291 (83)79.1,86.2 | 328 (90.8) 86.8,92.6 | 0.001** |
*The increase in the number of mothers after the intervention is due to the fact that during vacation families go to their relatives, their parents house etc. After vacation they come back and all the women participated in the endline survey including the 10 additional women had been a part of the main intervention; **Significant
About half 47.9% of the mothers had initiated breastfeeding within one hour of birth registering a marginal increase from 45.2%. Reasons cited for non-initiation (n=187) were caesarean section (84.5%), child in intensive care unit (10.7%), delay in getting baby (2.1%) and no breast milk (1.07%). Although prelacteal feeds are an accepted sociocultural norm in Kerala, a decline in this practice was observed from 28.9% to 23.4% after the intervention. The pre lacteal feeds given included gold (63.2%), water (35.6%), calamus (20.7%) and honey (17.2) [Table/Fig-4a].
Impact of intervention on infant and young child feeding practices.
| Parameters | Before | After | p-value |
|---|
| No (%) 95% CI | No (%) 95% CI | |
|---|
| Antenatal | n=87 | n=63 | |
| Modified diet during pregnancy | 61 (70.1) 65.5, 74.1 | 54 (85.7) 81.4, 88.3 | 0.01* |
| Under three mothers | n=351 | n=361 | |
| Initiation of breastfeeding within 1 hr | 159 (45.2) 40.4, 49.8 | 173 (47.9) 42.4, 52.1 | 0.466 |
| Prelacteal feeds | 101 (28.9) 24.1, 32.5 | 84 (23.4) 19.2, 27.3 | 0.001* |
| Colostrum given | 331 (94.4) 91.5, 96.03 | 350 (96.9) 93.8, 97.6 | 0.61 |
| Exclusive | | | |
| Breastfeeding | 195 (55.5) 50.3, 59.7 | 208 (57.5) 52.3, 61.8, 0.587 | |
| No bottle feeding | 252 (71.8) 66.7, 75.7 | 50 (79.3) 75.1, 82.8 | 0.016* |
| Age at which complementary feeding started (in months) |
| Other fluids | 4.6, 3.9, 4.9 | 4.1, 3.5,4.6 | 0.26 |
| Semisolid | 6.2, 5.2, 8.3 | 7.5, 6.3,8.1 | 0.51 |
| Solid | 9, 8.5, 11 | 10.1, 9.5,12 | 0.11 |
*Significant
Due to the short duration of follow-up and as less number of children would have been newly born following intervention, there was only a marginal increase from 55.5% to 57.5% in the babies that were exclusively breastfed; which can be considered a success. Out of 139 babies who were not exclusively breastfed, major reasons ‘related to mothers’ such as, insufficient breastmilk (35.2%), working/studying mother (8.6%) and other co-morbidities (2.2%). Reasons ‘related to child’ were child is hungry (32.4%), doctor’s advice (5.04%), inadequate weight gain (2.9%) and laziness of the child to take milk/no appetite (1.4%). The practical experience in the community also revealed that some hospitals and doctors encouraged mothers to give artificial feeds. Inspite of this, bottle-fed children showed a significant decline from 28.4% to 20.7% [Table/Fig-4a].
Hygiene and Diarrhoeal Diseases
The improvement in handwashing practices and hygiene was expected to logically lead to a decline in the diarrhoeal episodes and as expected diarrhoeal diseases (during three months prior to endline survey) recorded a decline though not significant from an already low rate of 21.7% to 17.7%. Though there was a decline in diarrhoeal diseases, Zinc supplementation was poor at 17.7% indicating that with the appropriate use of Zinc supplementation this can be brought down further; whereas there was an increase of more than 3 episodes of respiratory infections from 4.5% to 7.2% though not significant. The increase may be due to other reasons such as increased exposure to tobacco smoke within the homes which increased from 18.2% to 25.3% [Table/Fig-4b].
Impact of intervention on Hygiene, Diarrhoeal Diseases and Respiratory infections.
| Parameters | Before | After | p-value |
|---|
| No (%) 95% CI | No (%) 95% CI | |
|---|
| Washing hands with soap before feeding the child | 298 (84.9) 84.1, 90.4 | 330 (91.4) 87.9, 93.40 | 0.002* |
| Washing hands with soap before preparing food | 290 (82.6) 81.7, 88.5 | 327 (90.6) 87.2, 93.20 | 0.001 |
| Washing hands after going to toilet | 344 (98) 96.3, 99.1 | 356 (98.6) 96.2, 99.10 | 0.23 |
| Washing hands with soap after cleaning the child | 296 (84.3) 80.4, 87.3 | 323 (89.5) 85.7, 91.70 | 0.034* |
| Episodes of ADD | 76 (21.7) 17.5, 25.2 | 64 (17.7) 13.8, 21.10 | 0.175 |
| Respiratory infection |
| 1-2 episodes | 112 (31.8) 26.9, 35.6 | 103 (28.5) 23.9, 32.60 | 0.333 |
| >3 episodes | 16 (4.5) | 26 (7.2) | |
*Significant
Key Influencers
At endline, 86.9% of key influencers reported that initiation of breastfeeding should be within an hour compared to 77.6% at baseline. Across the study groups of under three mothers and key influencers, the reasons cited for not being able to breastfeed were similar. It included delivery through caesarean section (71.5%), mothers illness and other complications (27.3%) and delay in breast milk production (16.1%) though the percentage of respondents who gave these responses were found to have decreased from 74.6%, 32.2% and 21.2%, respectively.
Inspite of the short duration of follow-up, a decrease was also demonstrated in the percentage of the key influencers that had given pre lacteal feeds from 32.5% to 27.8%. Colostrum was a ‘must have’ for newborns according to 96.6% of key influencers as compared to 90.9% at baseline. The duration of exclusive breastfeeding was known to 87.3% as opposed to only 76.9% at baseline. The barriers stated for inability to breast feed exclusively were child is hungry, not enough breast milk and working mother. Though the intervention was able to reduce the barriers namely not enough breast milk from 65.5% to 57.7% and working mother from 46.9% to 39.7%; ‘the child is hungry premise’ continued to persist in the minds of the key influencers. Majority of the influencers (89.3%) knew the right time for introducing complementary feeding and this had increased from 79.5% at baseline. Regarding bottle feeding and commercially produced infant food, only 19.2% and 14.8% favoured its use as against 32.9% and 21.9% at baseline. The role of the key influencer’s in decision making also increased appreciably from 44% to 67.6%.
Among the mothers with children under three years of age and antenatal women the IYCF practices that showed improvement such as Antenatal (vis a vis modified diet during pregnancy), pre-lacteal feeds, colostrum given, bottle feeding etc., [Table/Fig-5a] were taken up for Mcnemar’s chi-square followed by Logistic regression. Pregnant women belonging to nuclear families was an independent predictor of improvement of antenatal care vis a vis diet (p=0.011, OR=0.045, 95% CI 0.004, 0.493). On applying regression ‘no bottle feeding’ was found to be an independent predictor of decrease in pre-lacteal feeds (p<0.001, OR:10.94, (95% CI 3.99-29.97) and vice versa [Table/Fig-5b]. As expected improvement in the practice of handwashing before feeding was significantly associated with awareness of the same.
Factors determining favourable change in IYCF.
| Improvement in diet of antenatal women | | | p-value |
|---|
| | Yes | |
| Type of family | Nuclear | 3 (75%) | 0.011* |
| Joint | 7 (11.9%) | |
| Age of mother | <26 yrs | 0 (0%) | <0.001* |
| >26yrs | 10 (38.5%) | |
| Decrease in bottle feeding | | Yes | |
| Exclusive breastfeeding | Same | 19 (5.5%) | <0.001* |
| Improvement | 8 (100%) | |
| Colostrum given | Same | 20 (5.9%) | <0.001* |
| Improvement | 7 (70%) | |
| Prelacteal feeds | Same | 19 (5.7%) | <0.001* |
| Improvement | 8 (40%) | |
| Decrease in prelacteal feeds |
| Colostrum given | Same | 10 (2.9%) | <0.001* |
| Improvement | 10 (100%) | |
| Exclusive breastfeeding | Same | 12 (3.5%) | <0.001 |
| Improvement | 8 (100%) | |
| No bottle feeding | Same | 12 (3.7%) | <0.001 |
| Improvement | 8 (29.6%) | |
| Practice of washing hands before feeding child |
| Awareness of washing hands | Aware | 22 (26.2%) | <0.001 |
| Not aware | 0 (0%) | |
*Significant
Independent predictors of change in IYCF practices.
| Antenatal:diet modification | | OR | 95% CI | p-value |
|---|
| Type of family | Joint | 1 (Ref) | | 0.011* |
| Nuclear | 0.045 | 0.004-0.493 | |
| No bottle feeding |
| Prelacteal feeds | No change | 1 (Ref) | | |
| Decreased | 10.9 | 3.9-29.9 | 0.001* |
*Significant
Discussion
The study showed a consistent increase in awareness and practice of key IYCF practices following the educational intervention among the antenatal women, mothers with children under three years of age and influencers.
The awareness of all key IYCF parameters such as initiation of breastfeeding within 1 hour, Exclusive Breastfeeding, 1000 days concept, breastfeeding options for a working mother, ill effects of bottle feeding increased significantly by 17.6%, 4.5%, 21.1%, 22.2%, 12.6%, respectively. In a study in Africa where conventional clinic-based Growth Monitoring Promotion (GMP) was replaced by participatory Community Based Growth Promotion (CBGP) a higher knowledge on early breastfeeding initiation was observed in the CBGP group at 54% versus 28% in GMP, exclusive breastfeeding was 73% in CBGP group versus 56% in GMP [15]. Long-term interventional studies demonstrate a higher increase in knowledge regarding IYCF.
A great majority of mothers (94.4%) had given colostrum to their babies and these figures correspond to the NFHS 3 and DLHS 3 data for Kerala (97%) and Ernakulam District (90%) [6,7]. A significant reduction in use of pre-lacteal feeds by 5.5% was observed in this study similar to Khushwaha KP et al., where there was a substantial reduction from 85% to 33% at the end of a year of peer counselling [9]. Another interventional study in Northern India by Khan MH et al., found that only 34% had been given prelacteals in the intervention group compared to 83% in the control group [14].
Inspite of early initiation of breastfeeding being beneficial for both the baby and the mother, only 39% of newborns in the developing world are put to the breast within one hour of birth [16]. In the present study, although all deliveries took place in hospitals, only 45.2% had been breastfed within the first hour of birth compared to the rural Kerala NFHS, DLHS Ernakulam statistics of 66.1% and 51.8%, respectively [6,7]. Reasons cited for delay were Caesarean section (84.5%), child in ICU (10.7%), delay in getting baby (2.1%) and no breast milk (1.07%). Other researchers have also cited similar reasons such as caesarean section, complications of delivery, baby in NICU and milk not produced immediately [17,18]. It is the highest in this study at 84.5% perhaps due to the higher prevalence rates of caesarean section [19]. Developed countries such as Australia also report Caesarean section to be a persistent barrier [20].
An increase in early initiation of breastfeeding after the intervention was observed by 2.7% which can be considered successful due to the short follow-up period and institutional deliveries. An increase in initiation of breastfeeding has been demonstrated in hospitals by providing antepartum breastfeeding counselling support [21]. Community based studies using peer counsellors and behavioural change intervention package have also demonstrated an increase in initiation of breastfeeding [9,14]. Though all hospitals in the District were Baby Friendly Hospitals (BFHI), delay in initiation of breastfeeding is a cause for concern [22]. The practical experience during the mothers meeting also revealed that some hospitals and doctors encouraged mothers to give artificial feed indicating the need to reorient health professionals about breastfeeding practices.
This study demonstrated an increase in exclusively breastfed children from 55.5% to 57.5% in a short follow-up period of 2 months. This is much higher than the DLHS 3 report of 16.9% in Ernakulam district, NFHS-3 report of 46.3% in Kerala and 40% in rural Bangalore [6,7,23]. The short period of the study may be responsible for the marginal increase since a change in practice would take a longer time to appear in a community. A systematic review determined that breastfeeding education and or support increased EBF rates and decreased significantly ‘no breastfeeding rate’ at birth, <1 month and 1-5 months [24].
Among the IYCF practices, there was a significant decrease in prelacteal feeds (p<.001), no bottle feeding (p<0.016), and a significant increase in all hygienic practices such as washing hands with soap before feeding the child (p<0.002), before preparing food (p<0.001), after cleaning the child (p<0.034). The two breastfeeding sensitive morbidities respiratory infections and diarrhoeal diseases registered a decrease though not significant. Thus, breastfeeding is economically justifiable, as the never breastfeeding group may require additional costs for use of health care services to the order of US$331 to US$475 per infant [25].
Post-intervention, nuclear families was an independent predictor of improvement in the diet of pregnant women (p=0.011, OR=0.045, 95% CI 0.004, 0.493). A marginal decrease (71 to 69.8%) was observed in the reliance on private hospitals for antenatal care. However, over a decade a 20% increase in antenatal care through private sector was observed in the same area [26]. In IYCF practice, decrease in bottle feeding was independently predicted by decrease in prelacteal feeds and vice versa (p<0.001, OR:10.94, (95% CI 3.99-29.97).
Studies in Bangladesh by Sanghvi T et al., have shown that to achieve behaviour change it is important to tailor strategies to the local situation and considering the opinion of not only mothers but also influential family and community members [27]. The follow-up of the study in Bangladesh has also indicated that large scale social and behavioural change communication intervention can have sustained impact on infant and young child feeding practices [28]. During the period of the study, there were no new government programs in the area nor was there mass migration.
Limitation(s)
The limitations of this study include the short period of follow-up and lack of a control group. Further studies of longer duration and with a control group can help in determining the sustainability of the intervention.
Conclusion(s)
A complex behaviour like breastfeeding is best addressed through a multilevel, multi-sectoral approach that includes attention to community, social/cultural and population coverage needs [29]. Follow-up mentoring and encouragement is necessary to continue and strengthen this trend of improvement of IYCF indicators [29].
*The increase in the number of mothers after the intervention is due to the fact that during vacation families go to their relatives, their parents house etc. After vacation they come back and all the women participated in the endline survey including the 10 additional women had been a part of the main intervention; **Significant
*Significant