Tuberous sclerosis is a rare autosomal dominant genetic disorder caused by mutation of TCS1 or TCS2 gene. The birth incidence is estimated to be 1 in 6000. It is a multisystem neurocutaneous disorder characterised by widespread hamartomas, cutaneous changes and neurological manifestations. It may present as seizures in adult patients and being a rare aetiology, presents a diagnostic challenge to physicians. Here, the authors report a case of a 48-year-old male who presented with recent onset of seizures and subsequently was found to have tuberous sclerosis. He was managed with oral levetiracetam and remained asymptomatic during follow-ups, over a period of two years.
Adenoma sebaceum, Genetic disorder, Hypopigmented skin lesions, mTOR, Phakomatosis
Case Report
A 48-year-old male, presented with a history of two episodes of Generalised Tonic Clonic Seizure (GTCS) and weakness in the last two months. He was apparently well till two months ago and had no other ailments, only hypertension for which he was on regular medications. He had no habituations or addictions. There was no family history of epilepsy. Cognitive function appeared to be normal.
On examination, he was found to have moderate pallor with systemic examination revealing no apparent abnormalities. Thorough general examination revealed well-defined, multiple, nodular growths on the nose, face and forehead suggestive of angiofibromas [Table/Fig-1]. Sessile and firm nodular growths of varying sizes were observed in the upper and lower extremities suggestive of periungual fibromas [Table/Fig-2]. Ash leaf spots were seen on the back [Table/Fig-3], and multiple hypopigmented macules were seen on the chest [Table/Fig-4].


Ash-leaf spots at the back.

Hypopigmented macules on the chest.

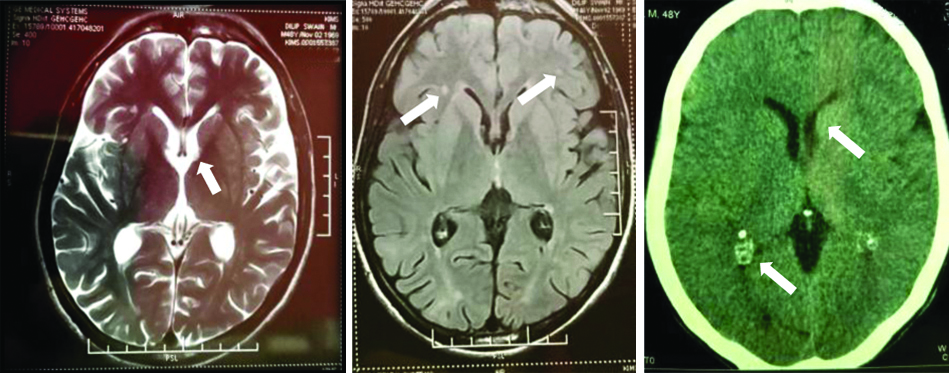
In view of the history of GTCS and cutaneous findings, he underwent further evaluation to identify the aetiology of GTCS. Haematological investigations revealed iron deficiency anaemia and normal serum electrolytes. EEG revealed abnormal inter-ictal epileptiform activity. CSF study was found to be within normal limits. Upper GI endoscopy showed mild gastritis and partially healed prepyloric ulcer. Ultrasound of abdomen and contrast-enhanced CT abdomen revealed a complex left renal cyst [Table/Fig-5]. Non-contrast CT and MRI of brain was done and showed subependymal nodules and cortical tubers [Table/Fig-6]. With the clinical features and imaging findings fulfilling the clinical diagnostic criteria for tuberous sclerosis [Table/Fig-7], the diagnosis was established [1].
USG abdomen showing complex left renal cyst.

Sub ependymal nodules and cortical tubers.
Updated diagnostic criteria for tuberous sclerosis complex 2012 [1].
| Major criteria | Minor criteria |
|---|
| Hypomelanotic macules (≥3, at least 5 mm diameter) | “Confetti” skin lesions |
| Angiofibromas (≥3) or fibrous cephalic plaque | Dental enamel pits (>3) |
| Ungual fibromas (≥2) | Intraoral fibromas (≥2) |
| Shagreen patch | Retinal achromic patch |
| Multiple retinal hamartomas | Multiple renal cysts |
| Cortical dysplasias* | Nonrenal hamartomas |
| Subependymal nodules | |
| Subependymal giant cell astrocytoma | |
| Cardiac rhabdomyoma | |
| Lymphangioleiomyomatosis† | |
| Angiomyolipomas (≥2)† | |
Definite diagnosis: Two major features or one major feature with ≥2 minor features; Possible diagnosis: Either one major feature or ≥2 minor features; *Includes tubers and cerebral white matter radial migration lines; †A combination of the two major clinical features (LAM and angiomyolipomas) without other features does not meet criteria for a definite diagnosis
The patient was managed conservatively. He was started on oral levetiracetam 500 mg twice daily and had no further episodes of seizures. He was counseled regarding the diagnosis of tuberous sclerosis and a family screening was advised along with regular follow-up visits. Improvement in symptoms and no further episodes of seizures were noted during follow-up visits over a period of two years.
Discussion
Seizures with onset in the adult life require special attention as they usually have an identifiable aetiology. The usual causes include trauma, Central Nervous System (CNS) infections, space-occupying lesions, Cerebro Vascular Accidents (CVA), metabolic disorders, and drugs [2]. Recent onset seizure in an older adult in the absence of these causes is a rare presentation.
Tuberous Sclerosis Complex (TSC) is an autosomal dominant disorder of cellular differentiation and proliferation with multiple system involvement. The reported incidence is 1 case per 6,000 live births [3] with no sexual or ethnic preponderance. The underlying cause is mutation in TSC1 (encoding hamartin) or TSC2 (encoding tuberin) which act as tumour growth suppressors regulating proliferation and differentiation. Diagnosis can be made by either the genetic or clinical criteria. TSC can not be excluded by conventional genetic testing as it does not identify mutations in 10-25% cases of TSC [1]. The index case was diagnosed as a definite case of tuberous sclerosis based on clinical criteria.
Hake S, in the study on cutaneous manifestations of tuberous sclerosis observed that ash-leaf spots are the most common manifestation present in about 90% cases of TSC. Ungual fibromas, found in about 50% cases, is highly suggestive of TSC [4].
The cutaneous manifestations found in this case were ash leaf spots, facial angiofibromas, confetti spots and ungual fibromas. Shagreen patch was absent. Cases of TSC vary considerably in their manifestations and clinical findings.
Wataya-kaneda M et al., in a study on 166 patients over a period of 10 years in Japan, observed that proportion of patients who were overlooked in childhood and newly diagnosed in adulthood had increased [5]. The index case had an identical course with skin manifestations being ignored for years untill he had seizures.
Hake S, reported a case of TSC in a middle-aged female whose presenting complain was growth on every digit of both feet. She had a history of seizures since childhood and was on antiepileptics but the diagnosis of TSC was established when ungual fibroma was noted [4]. The present case had no history of seizures until two months prior to hospitalisation, although the cutaneous manifestations were longstanding highlighting the unpredictable course of neurological symptoms in such cases.
The classical Vogt’s triad of TSC i.e., skin lesions, mental retardation and seizures is present in about one-third of patients [6]. Seizures present early and usually occur before 2 years of age. Zaroff CM et al., in their study noted a significant correlation between bilateral cortical tubers and age of onset of seizures with mental retardation [7]. The present case had bilateral cortical tubers but did not have mental retardation.
Onset of seizures in adulthood in cases of TSC as seen in the index case is a rare presentation. The varying nature of TSC epilepsies was highlighted in the Tuberous Sclerosis Registry to Increase Disease Awareness (TOSCA) study. In 2216 patients across 31 countries, seizure onset in adult patients was only in 0.6% cases [8].
Radiological findings of Tuberous sclerosis include calcification seen on skull X-ray in about 50% of cases. Periventricular sub-ependymal nodules, parenchymal hamartomas or cortical tubers, ventriculomegaly are frequently noted in MRI and CT scans [9]. Sub-ependymal giant cell astrocytomas can also be seen but are rare. This case had multiple sub-ependymal nodules and calcified tubers.
Tuberous sclerosis may also have renal, cardiac and pulmonary involvement. Mühler EG et al., in their study on 21 patients, observed that 14 cases had multiple rhabdomyomas, 3 were equivocal and 4 were normal in echocardiographic examination [10]. However, the index case had no echocardiographic abnormalities.
Renal problems are very frequent in patients with TSC. Various studies have reported the prevalence of renal angiomyolipoma in TSC to be 55 to 80% [11]. The present case had no evidence of renal angiomyolipoma or renal symptoms. Pulmonary manifestations like spontaneous pneumothorax, haemoptysis are associated with poorer outcomes. Regular fundoscopic examination is recommended as TSC is associated with visual impairment due to retinal detachment, vitreous haemorrhage and associated complications. A thorough evaluation did not reveal any such organ involvement in this case.
The management of these patients requires a multidisciplinary approach with mTOR inhibitors showing promising results in meta-analysis studies [12]. The prognosis in cases of TSC is determined by the severity of manifestations and the extent of organ involvement. About 75% of cases die before 25 years of age [13].
Conclusion(s)
Recent onset seizure in an older adult in the absence of usual causes like trauma, infections, stroke may be due to an uncommon aetiology like Tuberous sclerosis. Although TSC is usually associated with seizures at an early age, it may rarely have an atypical presentation of new onset seizures in adults. The organ involvement in TSC is variable. The cutaneous manifestations of otherwise asymptomatic TSC tend to be ignored by patients. Awareness in the community regarding skin manifestations of TSC is essential to ensure prompt diagnosis and appropriate follow-up in all such cases.
Definite diagnosis: Two major features or one major feature with ≥2 minor features; Possible diagnosis: Either one major feature or ≥2 minor features; *Includes tubers and cerebral white matter radial migration lines;
†A combination of the two major clinical features (LAM and angiomyolipomas) without other features does not meet criteria for a definite diagnosis
Author Declaration:
Financial or Other Competing Interests: None
Was Ethics Committee Approval obtained for this study? NA
Was informed consent obtained from the subjects involved in the study? NA
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Dec 16, 2019
Manual Googling: Jan 16, 2020
iThenticate Software: Jan 29, 2020 (11%)
[1]. Northrup H, Krueger DA, International Tuberous Sclerosis Complex Consensus GroupTuberous sclerosis complex diagnostic criteria update: Recommendations of the 2012 International Tuberous Sclerosis Complex Consensus ConferencePediatr Neurol 2013 49(4):243-54.10.1016/j.pediatrneurol.2013.08.00124053982 [Google Scholar] [CrossRef] [PubMed]
[2]. Kaur S, Garg R, Aggarwal S, Chawla SPS, Pal R, Adult onset seizures: Clinical, etiological, and radiological profileJ Family Med Prim Care 2018 7(1):191-97.10.4103/jfmpc.jfmpc_322_1629915758 [Google Scholar] [CrossRef] [PubMed]
[3]. Osborne JP, Jones AC, Burley MW, Jeganathan D, Young J, O’Callaghan F, Non-penetrance in tuberous sclerosisLancet 2000 355(9216):169810.1016/S0140-6736(00)02247-9 [Google Scholar] [CrossRef]
[4]. Hake S, Cutaneous manifestations of tuberous sclerosisOchsner J 2010 10(3):200-04. [Google Scholar]
[5]. Wataya-Kaneda M, Tanaka M, Hamasaki T, Katayama I, Trends in the prevalence of tuberous sclerosis complex manifestations: An epidemiological study of 166 Japanese patientsPloS One 2013 8(5):e6391010.1371/journal.pone.006391023691114 [Google Scholar] [CrossRef] [PubMed]
[6]. Rosset C, Netto CBO, Ashton-Prolla P, TSC1 and TSC2 gene mutations and their implications for treatment in Tuberous Sclerosis Complex: A reviewGenet Mol Biol 2017 40(1):69-79.10.1590/1678-4685-gmb-2015-032128222202 [Google Scholar] [CrossRef] [PubMed]
[7]. Zaroff CM, Devinsky O, Miles D, Barr WB, Cognitive and behavioral correlates of tuberous sclerosis complexJ Child Neurol 2004 19(11):847-52.Available from: https://journals.sagepub.com/doi/abs/10.1177/0883073804019011010110.1177/0883073804019011010115658788 [Google Scholar] [CrossRef] [PubMed]
[8]. Nabbout R, Belousova E, Benedik MP, Carter T, Cottin V, Curatolo P, Epilepsy in tuberous sclerosis complex: Findings from the TOSCA StudyEpilepsia Open 2018 4(1):73-84.10.1002/epi4.1228630868117 [Google Scholar] [CrossRef] [PubMed]
[9]. Chandrakala Patil S, Guruprasad KY, A case report of tuberous sclerosis in two generationsThe Journal of the Association of Physicians of India 2014 62(12):60-64. [Google Scholar]
[10]. Mühler EG, Turniski-Harder V, Engelhardt W, Von Bernuth G, Cardiac involvement in tuberous sclerosisBr Heart J 1994 72(6):584-90.10.1136/hrt.72.6.584785774 [Google Scholar] [CrossRef] [PubMed]
[11]. Kingswood JC, Belousova E, Benedik MP, Carter T, Cottin V, Curatolo P, Renal angiomyolipoma in patients with tuberous sclerosis complex: Findings from the TuberOus SClerosis registry to increase disease AwarenessNephrol Dial Transplant 2019 34(3):502-08.10.1093/ndt/gfy06329697822 [Google Scholar] [CrossRef] [PubMed]
[12]. Li M, Zhou Y, Chen C, Yang T, Zhou S, Chen S, Efficacy and safety of mTOR inhibitors (rapamycin and its analogues) for tuberous sclerosis complex: A meta-analysisOrphanet J Rare Dis 2019 14(1):39Published 2019 Feb 1310.1186/s13023-019-1012-x30760308 [Google Scholar] [CrossRef] [PubMed]
[13]. Sarkar S, Khaitan T, Sinha R, Kabiraj A, Tuberous sclerosis complex: A case reportContem Clin Dent 2016 7(2):236-39.10.4103/0976-237X.18307127307675 [Google Scholar] [CrossRef] [PubMed]