Enamel is a highly mineralised tissue possessing a distinct feature as the hardest tissue in humans. This hardness can be sometimes mistaken as an impermeable barrier against external irritation [1,2]. One usually thinks that newly erupted enamel would be strongest before eruption or before it’s subjected to various oral challenges, but in reality, previous research suggests that they are more vulnerable to caries in the first 2-4 years posteruptively [3]. To understand the dynamics of the caries process, it’s essential to evaluate the diffusion rate of cariogenic substances, ions, and molecules through the enamel pores in an aqueous phase [4-7]. But in the case of defective enamel, either quantitative or qualitative, they can be more permeable, permitting the flow of acidic substances to enamel resulting in dissolution from the surface layer [8]. This process of dissolution of molecules and ions into the surface promotes caries development. Yet another critical factor in the caries process is the rate at which the ions and molecules diffuse [6]. Based on these factors, a strong correlation exists between enamel permeability and developmental defects of enamel in the carious process [2].
Until 1992, all developmental defects of enamel were considered as hypoplasia later when the FDI commission on oral health analysed the magnitude of the anomaly, research and epidemiology they classified them as two distinct enamel defects namely hypoplasia and hypomineralisation [9]. Molar Incisor Hypomineralisation (MIH) a clinical phenotype can be traced to even the medieval times, but its standalone description as a separate clinical entity has promoted enormous clinical research for the past few years [10-12]. The term MIH was coined and termed as a qualitative defect of enamel, affecting 1 to 4 first permanent molars and can also be associated with permanent incisors [12]. The clinical picture of MIH tooth exhibits more porous surface with soft enamel, with distinct demarcated opacities ranging from white to yellow sharing a distinct border with normal enamel. MIH affected enamel surface usually develops to its standard thickness, but the posteruptive breakdown due to masticatory stress predisposes the tooth to dental caries. This can be considered as one of the significant risk factor for dental caries even in a population with low caries prevalence [13,14].
Even though there is a debate in the air regarding whether the carious lesion contributes to this situation, but there has been a rapid progression rate of caries in MIH affected teeth [15]. The current challenge faced by a paediatric dentist is the management of MIH, caused due to the disturbances in the early mineralisation stage with deficient mineral content, rich albumin and normal residual amelogenin [16,17].
Progression of caries can be well accomplished, by evaluating the permeability in dental tissues. Various methodologies to estimate enamel permeability are in place from simple dye penetration to advanced confocal laser scanning microscopy [18-20]. Although there exist a possible correlation between caries susceptibility and fluid flow, the role of enamel permeability remains entirely unknown [21]. This is because most caries research focuses on the process of demineralisation and remineralisation of enamel [22].
Currently, in the literature, studies evaluating the permeability of enamel in MIH affected teeth are relatively sparse. So, in the present study an attempt was made to assess the enamel permeability in permanent teeth with and without MIH using a scanning electron microscope. The null hypothesis tested was that there exists no difference in enamel permeability between teeth with MIH and without MIH.
Materials and Methods
*Ex-Vivo Validation Study
Prior to the commencement of the In-Vivo study, an Ex-Vivo pilot study was conducted to validate the presence of enamel droplets in permanent teeth with and without MIH. A total of 4 extracted premolars were collected, of which 2 teeth were affected with MIH and 2 teeth without.
Selection of Teeth
Children who required therapeutic extraction of premolars for orthodontic treatment; teeth without any developmental defects or dental caries; teeth without post eruption enamel breakdown
MIH Scoring Criteria
MIH Scoring was done prior to extraction of the teeth using the 10-point scoring system based on the Ghanim et al., 2015 [23].
Storage of Teeth and SEM Evaluation
The extracted teeth were immediately washed and cleaned in saline and stored in formalin fixative. Later for the evaluation of enamel droplets, these samples were dried and to take a negative replica addition silicone material, a polyvinylsiloxane (VPS) (3M ESPE Express STD) was used. Only labial surface was analysed for enamel droplets and for this, the labial surface impression was taken for each sample separately. The labial surface of the negative replicas in both the groups were further divided into 3 segments-cervical, middle and incisal third and sub divided into left, middle and right segments. SEM evaluation for the presence of enamel droplets was performed at 2000 X magnification. After calibration two examiners who were blinded about the samples, scored each segments using the scoring criteria as mentioned below in the in-vivo study [24-27].
*In-Vivo Study
Approval and Informed Consent
This in-vivo study was conducted in full accordance with the Research ethics committee from Armed forces hospital southern region KSA with approval number AFHSRMREC/2018/DENTAL/307. Written Informed consent was obtained from the parents of each participant in the study. Informed assent was also obtained from each child giving their willingness to participate in this study.
Sample Size and Study Design
The patients were randomly selected from the daily outpatient department visiting paediatric dentistry clinic at King Fahad dental center, AFHSR from March to August 2018. A total of 16 children from the both sex between the age of 7 to 8 years were selected for this study and divided into two groups. Group 1 (n=8) had children with MIH defects involving two or more incisors. Group 2 (n=8) with no clinical enamel defects or dental caries were chosen as the control group. A total of 8 teeth from each group had a sample size of 16 teeth for assessment.
Inclusion and Exclusion Criteria
Fully erupted permanent upper anterior teeth were selected in children with MIH. Teeth with posteruptive enamel breakdown, dental caries, dental restorations, trauma, morphological and any other structural changes of the enamel and children with special health care needs were excluded. Teeth without MIH were recruited from the caries-free group with no developmental defects of enamel.
Assessment of Enamel Surface Replica
The enamel surface of the children received thorough oral prophylaxis, polishing with fluoride free prophylactic paste, rinsed and dried. VPS (3M ESPE Express STD) impression material consisting of putty and light body was used as per the manufacturer’s instruction to record the impression in a two-step procedure. The impressions were further degassed and subjected to gold sputtering after separating the labial portion from the impression. The surface morphology of enamel was assessed based on the negative replica technique of droplets [24,25]. Scanning electron microscope (SEM JEOL, JSM 5900LV, Tokyo, Japan) was used to inspect the surface droplets which appeared as a negative replica in the impression [25].
Evaluation under SEM
All SEM images of both MIH and non MIH teeth were blinded before the assessment by two independent investigators. Labial surface of each sample was further divided into 3 segments as the cervical, middle and incisal third which was further subdivided as left, middle and right. From the total of 9 segments, three areas of 20×20 μm were examined, and scoring was recorded. A total of 144 SEM images were obtained for comparison. Presence of droplets was evaluated using SEM at 2,000 X magnification. The highest value representative of the area was taken for scoring. Intergroup comparison was also made comparing the 9 segments from both the groups.
Scoring Criteria
Presence of droplets was evaluated using multipoint visual scale [26] which was a modification of Lucchese A et al., 2012 and Bertacci A et al., 2007 scoring criteria [2,27]. The scoring used in this study is as follows:
Intense- with more than 75% of the entire enamel surface covered with droplets;
High- with less than 75% but more than 50% of the entire enamel surface covered with droplets;
Moderate- with less than 50% but more than 25% of entire enamel surface covered with droplets; and
Low- with less than 25% of the entire enamel surface covered with droplets.
Validation of Scoring Criteria
Two independent investigators used this modified scoring criteria. Randomly selected 30 SEM images from the total of 144 images were used to measure the inter examiner variability. Proper validation was done, based on Cohen’s k statistical method interobserver agreement was found to be almost perfect with a kappa score of 0.83 which was a high percentage.
Statistical Analysis
All the samples were subjected to statistical analysis using SPSS software (version 13.0; Chicago, Ill., USA). Odd’s ratio was calculated by Logistic Regression Analysis at 95 % Confidence Interval and Pearson’s Chi-square test was performed to derive the p-value, with 0.05 level of significance.
Results
Ex-Vivo Study
The negative replicas of ex-vivo tooth enamel with and without MIH, examined by means of scanning electron microscopy revealed that fluid droplets were present generalised in all samples. On comparing the presence of droplets between the two groups, MIH group showed a higher presence of droplets as compared to non MIH [Table/Fig-1,2].
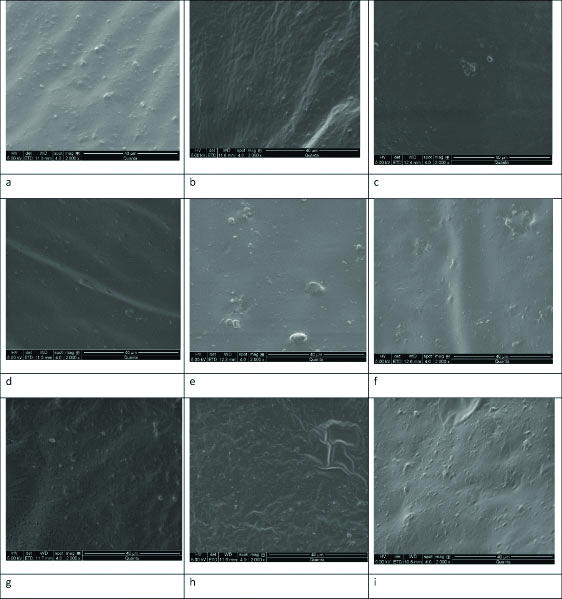
SEM micrographs of validation study showing the presence of fluid droplets depicting the enamel permeation at various segments in teeth without MIH a, b, c(cervical)d, e, f (incisal third)g, h, i (middle third).
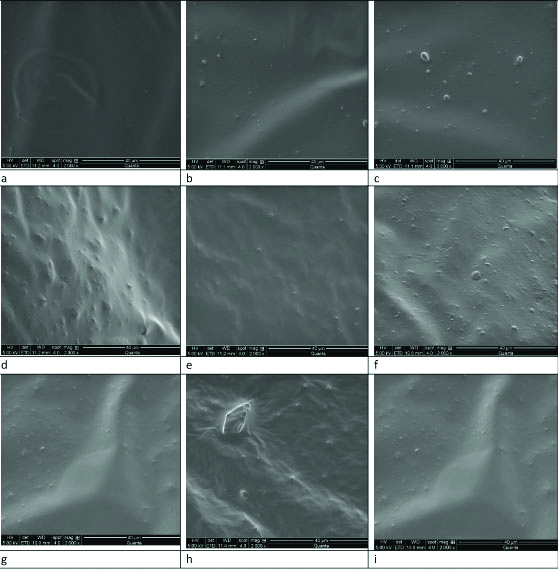
SEM micrographs of validation study showing the presence of fluid droplets depicting the enamel permeation at various segments in teeth with MIH a, b, c (cervical)d, e, f (incisal third)g, h, i (middle third).

Odds ratio was calculated by logistic regression analysis. Odd’s ratio=ad/bc=7×27/19×5=189/95=1.98 at 95% confidence Interval with lower limit 0.55 and upper limit 7.22. Odds ratio of 1.98 depicts that teeth with MIH will have 1.98 times more enamel permeability compared to teeth without MIH as shown in [Table/Fig-3].
Odds ratio comparison for ex-vivo study.
| Scores | MIH present | MIH absent | Total |
|---|
| 1 and 2 | 7 (a) | 5 (b) | 12 |
| 3 and 4 | 19 (c) | 27(d) | 46 |
The Odds ratio obtained suggests that teeth with MIH have 1.98 times more enamel droplets compared to teeth without MIH
In-Vivo Study
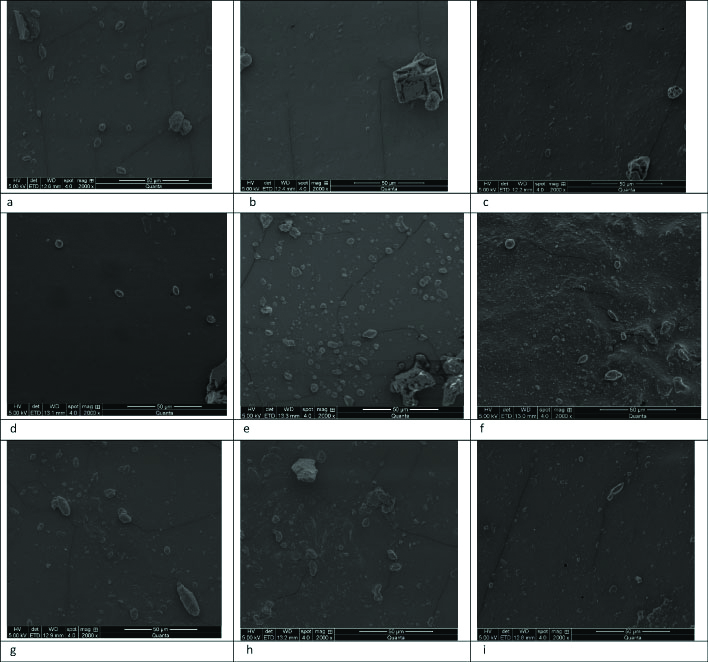
The negative replicas of In-Vivo tooth enamel with and without MIH, examined using scanning electron microscopy revealed that fluid droplets were seen in all the 9 segments of the teeth. The distribution of scores obtained under each segment in both the groups. In our study score1 (intense) was not observed in both the groups. The overall impression shows that in teeth without MIH (group 2), the score 4 (low) was predominant in all the 9 segments followed by score 3 (moderate) whereas score 2 (high) was found to be relatively low as in [Table/Fig-4] and [Table/Fig-5].
Distribution of scores in both the groups.
| Segment | Cervical left | Cervical middle | Cervical right | Middle left | Middle middle | Middle right | Incisal left | Incisal middle | Incisal right |
|---|
| Grading | LSc4 | MSc3 | HSc2 | LSc4 | MSc3 | HSc2 | LSc4 | MSc3 | HSc2 | LSc4 | MSc3 | HSc2 | LSc4 | MSc3 | HSc2 | LSc4 | MSc3 | HSc2 | LSc4 | MSc3 | HSc2 | LSc4 | MSc3 | HSc2 | LSc4 | MSc3 | HSc2 |
| Group I | 5 | 1 | 2 | 4 | 1 | 3 | 5 | 1 | 2 | 6 | 1 | 1 | 5 | 1 | 2 | 4 | 2 | 2 | 6 | 1 | 1 | 5 | 1 | 2 | 5 | 1 | 2 |
| Group II | 6 | 1 | 1 | 6 | 2 | 0 | 7 | 1 | 0 | 6 | 1 | 1 | 6 | 2 | 0 | 6 | 1 | 1 | 6 | 1 | 1 | 6 | 1 | 1 | 6 | 1 | 1 |
4 (Low), 3 (Moderate), 2 (High) and 1 (Intense) in Group 1 (teeth with MIH) and Group 2 (teeth without MIH)
SEM micrographs of validation study showing the presence of fluid droplets depicting the enamel permeation at various segments in teeth without MIH a, b, c (cervical)d, e, f (incisal third)g, h, i (middle third).
In teeth, with MIH (group 1) the score 4(low) was predominantly seen in all the segments evaluated. The next maximum observed score was score 2 (high) which was also present in all the segments, and it was more predominant in the cervical third followed by the middle and the incisal third. Score 3 (moderate) was found comparatively fewer to others in all the segments [Table/Fig-6]. There was a considerable difference in the presence of droplets between the two groups, with the MIH group showing more numbers than its counterpart. Odds ratio was calculated by Logistic Regression Analysis. Odd’s ratio was=ad/bc=17×66/55×6=1122/330=3.4 at 95% confidence Interval with lower limit 1.25 and upper limit 9.21. The p-value by Pearson’s Chi-square test is 0.0012, significant. Odds ratio of 3.4 shows that teeth with MIH will have 3.4 more times enamel permeability compared to teeth without MIH as in [Table/Fig-7].
Odds ratio comparison for In-vivo study.
| Scores | Teeth with MIH | Teeth without MIH | Total |
|---|
| 1 and 2 | 17 (a) | 6 (b) | 23 |
| 3 and 4 | 55 (c) | 66 (d) | 121 |
Pearson’s Chi-square test (p<0.0012) was found to be highly significant. The Odds ratio suggests that teeth with MIH will have 3.4 times more chance for developing dental caries compared to without MIH
SEM micrographs of validation study showing the presence of fluid droplets depicting the enamel permeation at various segments in teeth with MIH a, b, c (cervical)d, e, f (incisal third)g, h, i (middle third).
Discussion
The ex-vivo study conducted on extracted premolars showed a generalised distribution of enamel droplets in both the groups. The pattern of distribution was seen generalised with predominance in the MIH defective areas. This was done to validate the presence of enamel droplets before the start of the in-vivo study as no other reference literature was available at that time. The aim of this in-vivo study was to assess the differences in the enamel permeability of permanent teeth with and without MIH. The results derived from this study, reveals a generalised distribution of fluid droplets in both the groups examined, thus confirming enamel permeability. This is in accordance with the studies reported earlier in the literature [2,26,27] which demonstrated permeability of enamel in both primary and permanent teeth. On inter group comparison; teeth affected with MIH had more fluid droplets predominantly compared to the teeth without MIH with a statistical significance result. The data thus obtained rejects our null hypothesis, confirming the existence of difference in enamel permeability between teeth with and without MIH.
As there is no available data currently that evaluates the enamel permeability of teeth with and without MIH, this literature can open avenues for future research. The permeability of enamel is related to the pores, which might cause uptake and release of water droplets. Droplets thus formed on the enamel surface, are probably through a diffusion process. It was demonstrated that enamel permeability can best be appreciated while using VPS [2,27], a hydrophobic impression material. When a hydrophobic material like VPS is placed on hydrated enamel, through the above mentioned process of diffusion, water accumulates over these enamel pores, thus replicating in the impression material. The main advantages of using the VPS material for impression are ease of handling, non invasive, more comfortable to the children and can be used under any clinical conditions. Negative replica technique using VPS also reduces the complexity of procedure and errors while making a positive replica. We preferred VPS over other materials since it showed good stability without any damage to the impression while handling or even when subjected to direct observation under SEM [25,26].
The SEM image resolution obtained with VPS was also found to be superior for interpretation. These advantages of VPS make it an excellent diagnostic tool, in identifying children who are at high risk [27].
In our study, we used the scoring system proposed by Narrenthran JS et al., [26] adopted from the scoring criteria formulated by Luchesse A et al., and Bertacci A et al., [2,27]. This was preferred in our study to accommodate the broad moderate (Score2) with an appropriate representation of clinical significance. Thus the scoring grades used were low, moderate, high and intense. The ex-vivo study showed that MIH affected teeth showed,1.98 times more potential for enamel permeability, which gave a confirmatory signal that MIH teeth are more permeable compared to normal enamel. The in-vivo study further confirmed that MIH affected were 3.4 times more permeable than normal enamel, thus disproving our null hypothesis.
It has been reported that enamel surfaces of newly erupted permanent teeth showed more surface droplets than the mature one [27,28], probably due to the structures containing open protein forming diffusion pathways which get altered with the process of mineral deposition. This study could also establish similar findings with droplets on the enamel surface in all the teeth examined from both the groups, but with an increased presence in case of teeth with MIH.
In the case of hypoplastic and hypomineralised enamel, the porosity of enamel will be increased and in turn permeability of enamel also. These children fall under the category of high risk for caries development [24]. In this study too, MIH affected teeth demonstrated a high permeability of enamel with more droplets on the enamel surface.
It has been reported in the literature that enamel fluid flow has been related to the posteruptive maturation and caries susceptibility. As permanent teeth mature with age, permeability also reduces [27,29,30]. MIH lesions are caused due to the disturbances in the early mineralisation stage, which chronologicaliy affects enamel deficient in minerals, with regular content of residual amelogenin and rich albumin [16,17].
The microstructure of enamel looks preserved histologically indicating normal ameloblastic function during the secretory stage. But in areas affected with MIH, the crystals are disorganised with enlarged interprismatic spaces, suggesting post eruption problems in the early years. Hypomineralised enamel contains a high percentage of carbonate, indicating the persistence of high organic matter. The substitution or loss of carbonate increases the solubility in acidic media. But the persistence of carbonate could be expected to have the opposite effect [31].
Another possibility in MIH teeth is because of its greater porosity of enamel it enables adsorption of food and beverages, with the carbonate content in the lesion coming from the breakdown of organic compounds [32].
In, the newly erupted permanent teeth enamel is not matured, presenting with unique characteristics, more susceptible to demineralisation [29,33]. The enamel at this stage is more porous [34,35] with larger carbonated apattite concentration [36] and the composition has greater percent of impurities like sodium, magnesium, etc., [37] making it soluble in oral fluids.
With these structural defects in enamel and high content of enamel pore, teeth with MIH are at high risk for future caries development and posteruptive breakdown. Caries risk assessment should also include these defects for rendering preventive services.
Limitation(s)
SEM evaluation being very expensive and availability of large sample size with willingness of the children to participate in the study were some feasibility issues. So, only 16 children were included. Inclusion of all grades of MIH can be considered in the future studies with a larger sample size.
Conclusion(s)
Conclusions drawn from this study demonstrated a high presence of droplets in MIH teeth compared to teeth without MIH. This increase in enamel permeability gives speculation that it can contribute as one of the risk factors for the development of dental caries. Thus enamel permeability can serve as a tool for early detection and prevention of dental caries.