Birth asphyxia is a condition where gas exchange is impaired within the foetus. WHO defines it as “inability to initiate or maintain spontaneous breathing at birth” [1]. Neonatal mortality upto 23% is due to birth asphyxia as it is also the most common cause of neonatal deaths [2]. Impaired gaseous exchange due to asphyxia also causes foetal hypoxemia, hypercarbia and metabolic acidosis [3]. Roughly, 10% of births are associated with some degree of asphyxia and out of them 1% are severe and some further progresses to Hypoxic Ischemic Encephalopathy (HIE) which are a common cause of mortality and morbidity [4]. In India, institutional deliveries are only one-third and out of these, many asphyxiated newborns are being taken late to the centres, it is difficult to diagnose the same, if neonatal records are not available [5]. Hypoxic brain and systemic injury can be identified with biochemical biomarkers. Neonatal outcome can be predictable to some extent too. The asphyxia has adverse effect on every organ of body, however the common sequelae is HIE [6].
HIE injured cells release cellular enzymes, leads to elevation of some enzymes in blood which can be easily measured e.g., LDH. Neonatal asphyxia can lead to elevation of this and other enzymes also. The considerable rise in all of these after organ damage and asphyxia makes them possible predictors for assessing the severity of the hypoxic-ischemic injury [7]. Measurement of LDH in CB can be used as a biomarker for birth asphyxia.
In developing countries birth asphyxia is a major problem in newborns, biomarkers can be used for its timely diagnosis and also help in detecting prognosis. In Indian population, there is a paucity of literature regarding LDH level in birth asphyxia. Serum LDH level is an easily accessible tool in most of routine laboratories. Thus, through this study we had evaluated serum LDH as a biochemical marker of birth asphyxia in rural population.
Materials and Methods
This was a hospital based prospective analytical study (cohort study) done in NICU, Department of Paediatrics, Maharishi Markandeshwar Institute of Medical Sciences and Research (Deemed to be University), Ambala, Haryana, India in period of November 2017 to September 2019. The informed consent was taken in each case from parents and permission was granted by Institutional Ethical Committee (IEC) vide letter number IEC-1091. Total 100 newborns enrolled in study out of which 50 were asphyxiated cases and 50 were controls normal newborns. The asphyxiated newborns were classified into mild, moderate and severe HIE [8].
Inclusion Criteria
The newborns have been identified to have experienced birth asphyxia when the Apgar score was less than 7, at one minute of life.
Exclusion Criteria
Neonates with gross congenital malformations. Haemolytic disease of the newborn (Birth trauma) [9].
Maternal drug addiction or mother received magnesium sulphate within four hours prior to delivery or opioids.
Unwilling parents and haemolysed samples.
The sample size collected for this study (for α level of significance at 5% (0.005) and power of study assumed 80%) was 50 cases and 50 controls, based on literature [9].
Controls
All term neonates (50) who were born with Apgar score >7 at 1 minute of life. Detailed maternal history, assessment of intrauterine foetal well being and other relevant information were recorded as per the Performa. Apgar score of newborns was evaluated at 1, 5 and 10 minutes. They were managed at NICU as per the managing consultant.
At birth 2 mL of blood was collected from cases and controls and was sent for serum LDH level and at 24 hours, 2 mL blood sample was collected only in cases and sent for LDH measurement. The sample were analysed in biochemistry department by kit method i.e., reagent kit used of Relkon Diagnostics Pvt., Ltd.
Statistical Analysis
Descriptive statistical analysis was carried out and the student’s t-test was used to compare the quantitative data and qualitative data were analysed by using Chi-square/Fisher-Exact test to find the significance of study parameters. The α level of significance at 5% (0.005) and power of study assumed at 80%. The software used to analyse and compute data was SPSS version 20.
Results
Total 100 neonates were enrolled in the present study. Distribution of asphyxiated group and control group according to mode of delivery, gestational age, parity of mother, sex, meconium stained liquor are shown in [Table/Fig-1].
Distribution of case and control group.
| | Group | Total | Chi-square value | p-value |
|---|
| | Cases | Controls |
|---|
| Parity | Multigravida | 21 | 42% | 30 | 60% | 51 | 3.922 | 0.141 |
| Primigravida | 29 | 58% | 20 | 40% | 49 |
| Gestation* | SGA | 16 | 32% | 3 | 6% | 19 | 10.981 | 0.002 |
| AGA | 34 | 68% | 47 | 94% | 81 |
| Sex | Female | 24 | 48% | 22 | 44% | 46 | 0.161 | 0.688 |
| Male | 26 | 52% | 28 | 56% | 54 |
| Mode of delivery* | Vaginal | 29 | 58% | 42 | 84% | 71 | 8.208 | 0.008 |
| LSCS | 21 | 42% | 8 | 16% | 29 |
| Meconium stained liqour | No | 44 | 88% | 49 | 98% | 93 | 3.840 | 0.112 |
| Yes | 6 | 12% | 1 | 2% | 7 |
Asterisk denotes significant p-value
AGA: Appropriate-for-gestational-age; SGA: Small-for-gestational-age; LSCS: Lower segment caesarian section
The mean birth weights in cases and controls were 2.58 kg±0.45 SD and 2.81 kg±0.31 SD respectively with significant p-value <0.005. Mild birth asphyxia was recorded in 3(6%), moderate birth asphyxia in 32 (64%) and 15 (30%) had severe birth asphyxia. The frequency of HIE were: stage 1 in 16%, stage 2 in 4%, stage 3 in 16% and 64% cases had no HIE. The p-value is highly significant in moderate and severe birth asphyxia (<0.005).
Comparative values of LDH in CB and at 24 hours are shown in [Table/Fig-2]. The sensitivity, specificity and predictive value of LDH are shown in [Table/Fig-3]. Comparison of LDH of CB at birth of cases and controls, the p-value (<0.001) was highly significant. The cut-off level of LDH taken as 580U/L. The number of neonates with LDH levels >580 U/L was significantly more in cases when compared to controls with p<0.001. The LDH level at 24 hours of birth in cases was: 2 (4%) had LDH level <580 U/L and 48% (96%) had >580 U/L.
Comparison of LDH (CB) and LDH (24 hours) in cases and LDH (CB) in controls.
| Cases | Controls | T | p-value | Difference |
|---|
| Mean | SD | Mean | SD | Mean | SD |
|---|
| LDH (CB) U/L | 999.04 | 521.73 | 299.90 | 205.46 | 8.816 | 0.001 | 699.140 | 79.299 |
| LDH (24 hours) U/L | 1574.72 | 916.34 | | | | | | |
CB: Cord blood; LDH at 24 hours were assessed only in cases and compared with cord blood LDH
Shows sensitivity, specificity and predictive values of LDH.
| LDH (CB) |
|---|
| Statistic | Percentage | 95% CI |
|---|
| Specificity | 90.00% | 78.19% to 96.67% |
| Sensitivity | 94.00% | 83.45% to 98.75% |
| Negative likelihood ratio | 0.07 | - |
| Positive likelihood ratio | 9.4 | 4.08 to 21.65 |
| Disease prevalence | 50.00% | 39.83% to 60.17% |
| Negative Predictive Value (NPV) | 93.75% | 83.30% to 97.83% |
| Positive Predictive Value (PPV) | 90.38% | 80.32% to 95.59% |
| Accuracy | 92.00% | 84.84% to 96.48% |
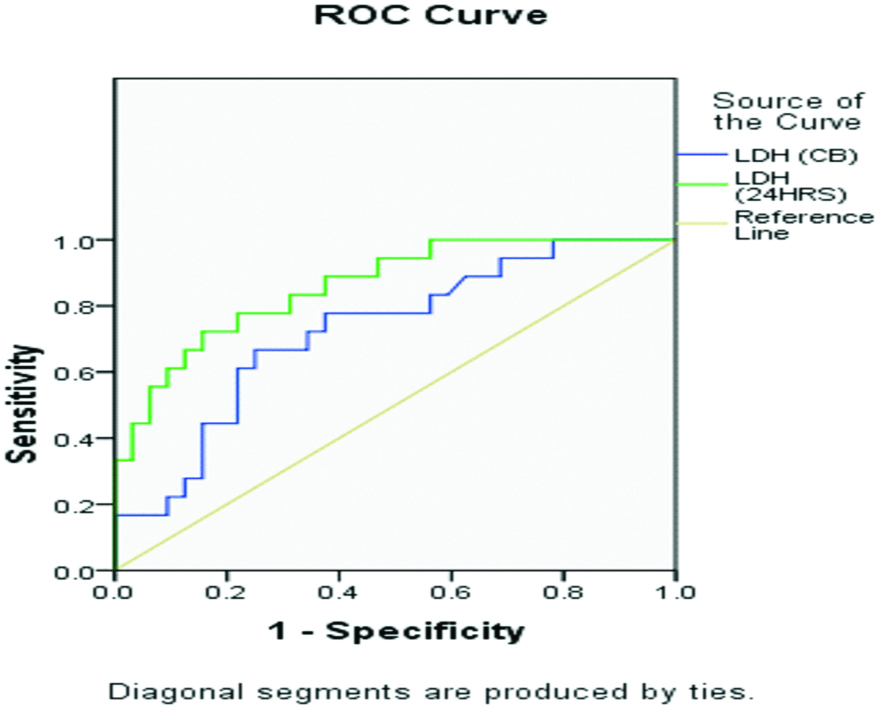
The LDH (CB) value of mild, moderate and severe were 585.33±424.78 U/L, 694.91±444.22 U/L, 1369±672.59 U/L, respectively with highly significant p-value. The LDH (24 hours) values in mild, moderate, severe newborns were 772.33±108.61 U/L, 1103.69±605.25 U/L, 2457±1019.81 U/L, respectively with highly significant p-value. LDH value of CB and at 24 hours increased significantly with the severity of birth asphyxia, with p-value <0.001. Out of 50 cases of birth asphyxia, 11 required mechanical ventilation. Those newborns which received mechanical ventilation had significantly increased level of LDH level in CB and at 24 hours. The LDH level was highly raised in non-survivors both in CB and at 24 hours of life (1479.67U/L & 3145.33U/L, respectively). Receiver Operator Characteristics (ROC) was generated for LDH at birth CB and at 24 hours [Table/Fig-4].
Receiver operator curve of LDH at birth Cord Blood (CB) and at 24 hours.
Discussion
Perinatal asphyxia is one of the main factors responsible for mortality and morbidity in neonate [10]. The main finding in this study was significantly raised level of LDH in CB at birth in asphyxiated newborns and at 24 hours of post-natal life in cases. It shows that LDH is a good predictor of organ damage in term neonates with birth asphyxia. There is an increased LDH level as a result of ischemia induced leakage of enzymes therefore marked elevation may be a sensitive indicator of ischemic damage.
Distribution according to gender in this study was similar to other studies [5,11]. No considerable association was found between birth asphyxia and parity of mothers (p> 0.05) which was similar to the study by Reddy S et al., [5]. In the current study, more cases were delivered by vaginal then caesarean section. The values are contrary to Reddy S et al., and Khreisat WH et al., in which the frequency of birth asphyxia were more in cases born by LSCS in comparison to controls born by LSCS [5,12]. The cut-off level of LDH was taken as 580U/L. All the cases, that is term neonates with birth asphyxia, had significantly higher concentration of LDH levels. In comparison to Sanjay KM et al., this study had more cases with LDH level >580 U/L [9]; similar to the study by Shylaja CG et al., [13] and less than Reddy S et al., [5]. The comparison among the studies is shown in [Table/Fig-5]. The sensitivity of LDH in this study was more than Sanjay KM et al., [9] and lower than Reddy S et al., Karlsson M et al., Shylaja CG et al., [5,7,13]. The specificity and PPV of LDH was almost similar to Reddy S et al., Sanjay KM et al., Shylaja CG et al., [5,9,13].
Comparison of different study on basis cut-off level of LDH 580 U/L [5,9,13].
| Cases | Controls | p-value |
|---|
| <580 U/L | >580 U/L | <580 U/L | >580 U/L |
|---|
| Present study | 6% | 94% | 90% | 10% | <0.001 |
| Sanjay KM et al., [9] | 40.82% | 59.18% | 92% | 8% | <0.001 |
| Shylaja CG et al., [13] | 6% | 94% | 94% | 6% | <0.001 |
| Reddy S et al., [5] | 0% | 100% | 90% | 10% | <0.001 |
The area under the ROC curve for LDH at 24 hours was 0.861 as compared to LDH (CB) ROC is 0.725 in relation to HIE which is comparable to other study. The incidence of HIE in the present study compared with other studies mentioned in [Table/Fig-6]. The incidence of HIE in this study was lower as compared to Rajakumar PS et al., and slightly higher in comparison to Karunatilaka DH et al., [14,15].
Comparison of different studies on basis of sensitivity, specificity, Positive Predictive Value (PPV), Negative Predictive Value (NPV), Area Under Curve (AUC) [5,7,9,13].
| Sensitivity | Specificity | PPV | NPV | AUROC |
|---|
| Present study | 94% | 90% | 90.38% | 93.75% | 0.861 |
| Reddy S et al., [5] | 100% | 89% | 92% | 100% | 0.998 |
| Karlsson M et al., [7] | 100% | 97% | 92% | 100% | - |
| Sanjay KM et al., [9] | 59.18% | 92% | 87.88% | 69.70% | 0.954 |
| Shylaja C et al., [13] | 100% | 88% | 89.29% | 100% | 0.939 |
PPV: Postive predictive value; NPV: Negative predictive value; AUROC: Area under curve; ROC: Receiver operating characteristic curve
Limitation(s)
LDH level at 24 hours was not estimated in controls.
Conclusion(s)
Good correlation was found between LDH levels in cases with severity of birth asphyxia. LDH at 24 hours is a more accurate method to differentiate newborn with birth asphyxia and without birth asphyxia. By estimation of LDH level of CB and at 24 hours can help in differentiation of term newborn with asphyxia and without asphyxia, with reasonable degree of accuracy. The LDH at 24 hours have more accuracy than CB LDH. LDH can be used as a biomarker for diagnosis of birth asphyxia in sick newborns which are referred from peripheral hospitals without past records.
Asterisk denotes significant p-value
AGA: Appropriate-for-gestational-age; SGA: Small-for-gestational-age; LSCS: Lower segment caesarian section
CB: Cord blood; LDH at 24 hours were assessed only in cases and compared with cord blood LDH
PPV: Postive predictive value; NPV: Negative predictive value; AUROC: Area under curve; ROC: Receiver operating characteristic curve