Genital warts (condyloma acuminata) are benign, proliferative tumours which occur in the genital, anal, perineal and/or perianal areas. These warts are caused by Human Papilloma Virus (HPV). They are double-stranded DNA viruses which replicate in squamous epithelial cells. Many types of HPV has been recognised but 6 and 11 HPV types accounts almost 75-90% of genital warts cases. Many medical and ablative treatment modalities are available like topical podophyllin, imiquimod, cryotherapy, but recurrence is still a problem in many patients. Recently, a concept of combination treatment has been practiced and it was found to be better than monotherapy because of the synergistic effect of both the compounds. There are studies on the use of combination of cryotherapy with topical podophyllin and various other combinations but to achieve complete clearance of genital warts with no recurrence is still a challenge for the dermatologists. Thus, a combination treatment was needed to overcome this problem. So, a thought was given to use a combination of two modalities having different mechanism of action for treating genital warts. We hereby report a case of multiple giant genital warts in an immunocompetent female in whom complete clearance of lesions was achieved by a combination of Cryotherapy and 5% Imiquimod cream within six weeks of treatment.
Condyloma acuminata, Human papilloma virus, Topical immunomodulators, Topical therapy
Case Report
A 34-year-old married; female patient came to the dermatology outpatient section with the chief complaint of raised lesions over her external genitalia for the past four months which were associated with itching. The lesions initially were smaller in size and which gradually increased to the present size. She took a consultation with a private practitioner, details of which were not available, but some oral medications were prescribed. However she failed to adhere to the treatment protocol.
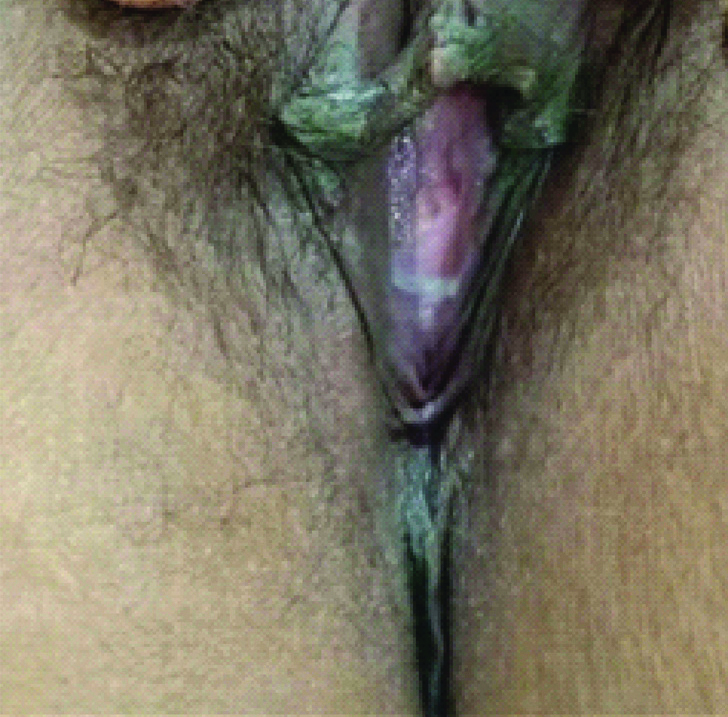
On examination at the time of consultation it was found that, she had large verrucous fleshy growth of approximate size of 2×5 centimeter on her left labia majora, 2 small similar lesions, 1 over the right labia minora and 1 lesion over its upper border [Table/Fig-1].
Lesions during 1st visit.

Differential diagnosis of Condyloma acuminata and Condyloma lata were considered. On cutaneous examination, no supportive evidence in th favour of Condyloma lata was present as its lesions are smooth, moist and flat whereas those of condyloma acuminata are cauliflower like, dry, and bulky white. The features of the lesions of this patient were in favour of condyloma acuminata so it was considered as a final diagnosis.
Her routine blood investigation included complete blood count and serum biochemistry (Sr. Creatinine, Urea, SGOT, SGPT and Bilirubin levels) which were within normal reference range. Her serology for hepatitis B, hepatitis C and retrovirus were negative. As the patient had discomfort due to the lesions, a fear of spread of the lesions to her partner and as she was a resident of far off town, she expressed her desire for quick relief from her complaint.
She was started on topical Imiquimod 5% cream, once a day application which was scheduled as three days on and four days off in a week for six weeks, in addition, cotton-tipped applicator based Liquid Nitrogen Cryotherapy (LN2) was given to lesions at two-week interval in total three sittings for six weeks till all lesions clear, which was achieved in three sessions. Each session consisted of three freeze-thaw cycles. In her second visit i.e., after two weeks, there was an almost 50% reduction [Table/Fig-2] of size of all the lesions, 75% reduction in size of all lesions at the third visit at four weeks [Table/Fig-3] and at the final visit after six weeks, she got complete (100%) reduction [Table/Fig-4]. Cryotherapy was not done on the day of Imiquimod cream application. The patient tolerated the treatment protocol well and without any significant adverse effects. Patient was under follow-up over a period of three months and there was no recurrence of the lesions and also, no late adverse side effects related to the treatment.
Approximately, about 50% Reduction i.e., 1×3 cm in the 2nd visit.

Approximately, about 75% reduction i.e., 0.5×2 cm in the 3rd visit.

Complete clearance of lesions seen during the 4th visit.
Discussion
Genital warts are caused due to infection by specific types of HPV [1] and it is one of the most common sexually transmitted viral infections in the world. They can be either raised (exophytic) or flat. Exophytic genital warts are commonly seen secondary to inoculation with non-oncogenic HPV types 6 and 11 into the basal epithelium, while flat warts are generally secondary to potentially oncogenic HPV types 16 and 31. Genital warts can seldom cause irritation and discomfort, predominantly during intercourse, while most cases are asymptomatic. It is the psychosocial effects of infection, such as a sense of embarrassment, depression, and apprehension, that represent the more substantial toll for maximum patients with genital warts. Various medical treatment modalities like topical podophyllin, podophyllotoxin, imiquimod 5% and 3.75% cream, sinectechins 15% ointment and 5-fluorouracil and some ablative modalities like trichloroacetic acid application, cryotherapy, electrosurgery, scissor excision, Co2 laser and systemic therapy like Interferon are available but complete clearance of lesions and recurrence is still a problem in many patients [1]. There are studies on the use of combination of cryotherapy with topical podophyllin, podophyllin 25% and post-ablation immuno-modulation with sinecatechins 15% ointment [2] and oral zinc sulfate with imiquimod, in the treatment of vulvar warts and various other combinations. In-spite of numerous options available, none is promising in achieving complete clearance and without recurrence and its treatment is still a challenge for the dermatologists. Genital warts are highly infectious and to arrest their transmission to partner, there is need of a treatment modality having early response and complete clearance. Recently, a concept of combination treatment has been practiced and found it always better than monotherapy because of the synergistic effect of both the compounds. A combination of two modalities having different mechanism of action can be a better option than the combination of two modalities having a similar mechanism of action.
Cryotherapy induces tissue damage in two mechanisms. First by causing damage to the blood vessels and capillaries in the target region which leads to ischaemic necrosis of the tissue. Second mechanism cause damage to the cells more complexly by generation of ice crystals and inducing osmotic cell injury and thus causing cellular membrane disruption. As the tissue cools, ice crystals form between cells and create an osmotic gradient speedily drawing water out of the cells. As cooling continues, crystals are produced inside the cell which causes the rupture of cell. Thawing process also damages the cells as it causes melting of the crystals outside the cells, that creates a gradient which speedily draws water back into the cell and causes them to swell and ultimately burst [2]. Imiquimod 5% cream produces an antitumour effect by boosting of both innate and cell-mediated immunity and thus is an immune response modifier. It is a topical agent that enhances local production of immune-stimulating cytokines like IFN-a, TNF-a, IL1, IL-1RA, IL-6, IL-8, IL-10, IL-12, p40, granulocyte colony-stimulating factor, granulocyte/macrophage colony-stimulating factor, macrophage inflammatory protein, and macrophage chemotactic protein-1. As a Toll Like Receptor (TLR)-7 and TLR-8 agonist, imiquimod was shown to induce these proinflammatory cytokines through activation of the central transcription factor, Nuclear Factor kappa-B (NF-κB) [3].
In literature, the previous studies carried out for treatment of genital warts with combination of two modalities are as follows: a) Treatment of anogenital HPV infection with combination of cryodestruction, podophyllin 25% and post-ablation immunomodulation with 15% sinecatechins ointment [3]. In which success and recurrence rates varying from 23% to 94% and from 4.1% to 77%, respectively have been found. Also, it has been noted that recurrence rate of sinecatechins ointment in recent years was very low i.e., 4.1-10.6%. After a total period of six months of follow-up, the initial clearance rate was 96.3% with a recurrence rate of 7.4% [4]; b) A study on treatment of vulvar warts with a combination therapy of oral zinc sulfate with imiquimod, podophyllin or cryotherapy was carried out where no significant difference was observed in the response to treatment. Relapse was significantly higher after six months in the patients treated with podophyllin, imiquimod and cryotherapy in comparison to patients receiving treatments in combination with oral zinc sulfate (p<0.05) [5].
Most common local inflammatory side effects encountered with 5% imiquimod cream are erythema, pruritus, burning, irritation, pain, tenderness, ulceration, and those of cryotherapy are local tissue destruction, which include painful blistering, infection, ulceration, possible permanent scarring, and depigmentation [6]. This patient did not encounter any of these side effects and responded well to this combination. We have treated our patient with a combination of imiquimod and cryotherapy and found excellent results in the form of early response and complete clearance of lesions. The time period for clearance of lesions with monotherapy of imiquimod as per literature is 16 weeks which in our considerate opinion is a bit unrealistic time frame [3]. During such a long duration of treatment period, patients can indulge in unprotected sexual intercourse and can transmit the infection to their partners. The limitation of our observation is that it has just been tried in one patient and that the follow-up observation period was short. It should ideally be longer, atleast up to six months.
Conclusion(s)
Combination treatment with two modalities like Cryotherapy and 5% Imiquimod cream having different mechanisms of action can give more promising result in treatment of genital warts. Randomised Control Trials should be carried out upon the use of combination of cryotherapy and imiquimod.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Sep 16, 2019
Manual Googling: Nov 27, 2019
iThenticate Software: Jan 09, 2020 (18%)
[1]. Cox JT, Petry KU, Rylander E, Roy M, Using imiquimod for genital warts in female patientsJ Women’s Health Larchmt 2004 13(3):265-71.10.1089/15409990432301642815130255 [Google Scholar] [CrossRef] [PubMed]
[2]. Prohaska J, Badri T, CryotherapyStatPearls [Internet] 2019 Stat Pearls Publishing:14 [Google Scholar]
[3]. Perry CM, Lamb HM, Topical imiquimodDrugs 1999 58(2):375-90.10.2165/00003495-199958020-0001710473026 [Google Scholar] [CrossRef] [PubMed]
[4]. Juhl ME, Seferovic V, Antonijevic S, Krunic A, Combined treatment of anogenital HPVinfection with cryodestruction, podophyllin 25% and post-ablation immunomodulation with sinecatechins 15% ointment- A retrospective analysisInt J STD & AIDS 2016 27(12):1071-78.10.1177/095646241560737526404110 [Google Scholar] [CrossRef] [PubMed]
[5]. Akhavan S, Mohammadi SR, Modarres Gillani M, Mousavi AS, Shirazi M, Efficacy of combination therapy of oral zinc sulfate with imiquimod, podophyllin or cryotherapy in the treatment of vulvar wartsJ Obstet Gynaecol Res 2014 40(10):2110-13.10.1111/jog.1245725132143 [Google Scholar] [CrossRef] [PubMed]
[6]. Yanofsky VR, Patel RV, Goldenberg G, Genital warts: A comprehensive reviewJ Clin Aesthet Dermatol 2012 5(6):25-36. [Google Scholar]