Evaluation of Hypomagnesemia in Acute Myocardial Infarction Patients
R Vedamanickam1, Anandan Palanychamy2, Giridharan Bupesh3
1 Associate Professor, Department of General Medicine, Sree Balaji Medical College and Hospital, Chennai, Tamil Nadu, India.
2 Assistant Professor, Department of General Medicine, Sree Balaji Medical College and Hospital, Chennai, Tamil Nadu, India.
3 Associate Director, Research and Development Wing, Sree Balaji Medical College and Hospital, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Palanichamy Anandan, Assistant Professor, Department of General Medicine, Sree Balaji Medical College and Hospital, Chennai, Tamil Nadu, India.
E-mail: anandanpdr.s@gmail.com
Introduction
Magnesium inhibits potassium efflux and calcium influx, the two events which are harmful to cardiac muscle survival during ischaemia. Magnesium prevents mitochondrial calcium overloading and maintains Adenosine Triphosphate (ATP) synthesis, which could result in smaller infarct size.
Aim
To compare the levels of serum magnesium in patients with Acute Myocardial Infarction (AMI) presenting within the first 24 hours.
Materials and Methods
This case-control study was conducted in Department of Medicine at a Tertiary Care Hospital, for 6 months from June 2018 to December 2018. A total of 60 participants were taken into the study and were divided into two groups. Group-1 was control subjects and Group-2 was patients with AMI. Serum magnesium level was assessed in both the groups and the results were compared. Student’s t-test was performed using SPSS version 21.0.
Results
A total of 73% of patients with AMI were more than 41 years, 53% of patients presented with anterior wall MI, 40% of patients presented with inferior wall Myocardial Infarction (MI) and 7% of patients with anterolateral MI. The mean serum magnesium level in AMI patients was found to be 1.23±0.98 mg/dL and was 2.12±0.68 mg/dL in control group, which was statistically significant.
Conclusion
Low serum magnesium was significantly found in AMI patients and their comorbidities. Therefore supplementation of Magnesium might improve the patients’ outcome.
Atherosclerosis, Comorbidities, Coronary heart diseases
Introduction
Magnesium is a mineral which plays a pivotal role in numerous biochemical reactions in the human body. It is an essential co-factor in all ATP-dependent enzymatic reactions. Magnesium protects the heart by decreasing contractility and ATP use [1]. Magnesium inhibits potassium efflux and calcium influx, the two events which are harmful to cardiac muscle survival during ischaemia [2]. A study suggests that deficiency in magnesium is a major risk factor in the development of atherosclerosis [3]. In a study done by Flink E et al., it is shown that there is a rise in levels of free fatty acids and decrease in levels of magnesium during the first 48 hours of AMI [4]. This occurs because of a sudden increase in catecholamine levels after AMI, which leads to lipolysis decreasing the magnesium level through increased uptake of magnesium into adipocytes and intracellular saponification by free fatty acids [5]. There is another factor which causes hypomagnesemia like diarrhoea, alcoholism, stress, overuse of diuretics [6].
Pharmacological effects of intravenous magnesium were considered as beneficial in arrhythmia. Magnesium with potassium therapy may reduce the aggregation of thrombosis. Magnesium also causes vasodilation and improves muscle contraction. Treating patients with ischaemic heart diseases with magnesium effectively decreases the risk of mortality due to AMI [7].
In the present study, the serum magnesium was investigated in patients of acute myocardial infarction and its associated comorbidities.
Materials and Methods
This case-control study was conducted in the Department of Medicine at a Tertiary Care Hospital from June 2018 to December 2018. Institutional Ethical Committee permission (IEHC/003/978/SBMCH-19) and informed consent from patients were obtained. A total of 60 participants were taken in the study and were divided into two groups. Group1- 30 patients were control and Group 2-30 patients with AMI comorbidities.
Inclusion Criteria
Patients diagnosed as having myocardial infarction and presenting within 24 hours with clinical features of ST elevation in ECG and abnormal echocardiography.
Exclusion Criteria
Patients with history of co-morbid conditions like liver or renal diseases. AMI patients with higher and normal magnesium levels were excluded.
Age-matched controls (patients attending for gastric problems) were used to compare the study cases.
The details including age, gender, history of previous myocardial infarction and cardiovascular risk factors (smoking, dyslipidaemia, hypertension and diabetes mellitus) and medications were obtained at the time of admission. Serum magnesium level was assessed using spectrophotometry by Methylthymol blue method using Biosystem kit and a range of 1.8 to 2.4 mg/dL was considered as normal [8].
Statistical Analysis
Student t-test was performed and compared with p-value of <0.001 using SPSS version 21.0.
Results
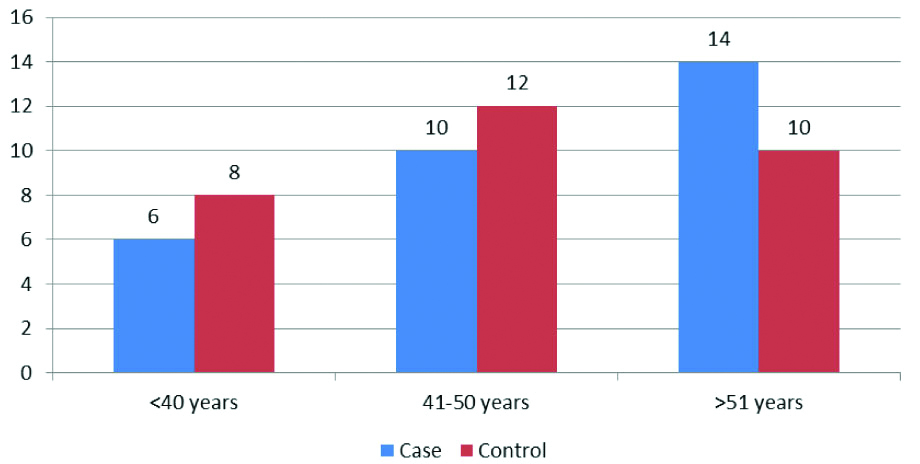
In this study, the age wise distribution of the control (Group 1) and case group (Group 2) are presented in the [Table/Fig-1]. Among the risk factors analysed, the hypertension and diabetes patients were found predominantly higher than the others [Table/Fig-2].
Age-wise distribution of case controls and AMI patients.
Risk factors analysis of Group 2 patients.
| Risk factor | % |
|---|
| Hypertension | 23 |
| Diabetes | 17 |
| Hyperlipidemia | 13 |
| Both Hypertension and Diabetes | 3 |
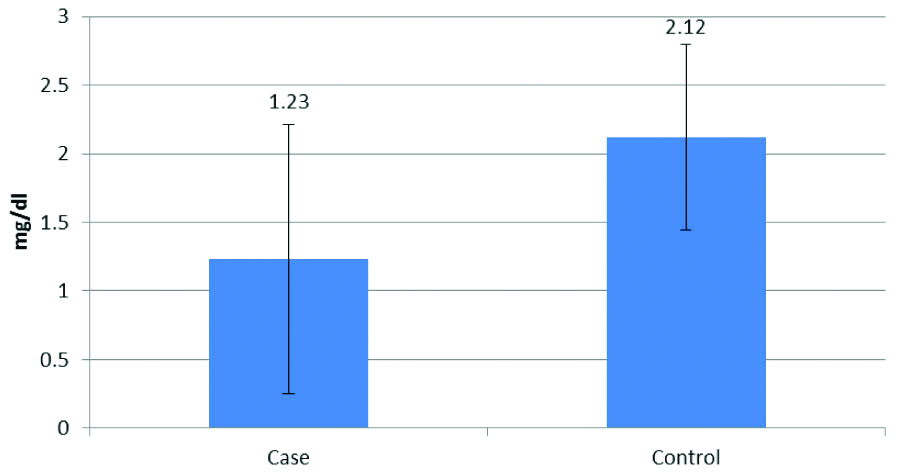
The mean serum magnesium level in AMI patients was 1.23±0.98 mg/dL and in control group 2.12±0.68 mg/dL, which was statistically significant (p-value of <0.001) [Table/Fig-3].
Comparison of Magnesium levels in Control and AMI cases.
Discussion
Hypomagnesemia associated with AMI may be transient, and serum magnesium concentrations may become normal during hospitalisation [8,9]. Moreover, experimental myocardial infarction brought about by coronary artery ligation will lead to an immediate efflux of magnesium from the ischemic area. In the present study, the correlation of magnesium level is determined in the AMI and patients with its comorbidities. The study further elucidates the correlation of Magnesium levels between the control group and AMI associated comorbidities. The results of the study found that mean serum magnesium level in AMI patients was lowered (1.23±0.98 mg/dL) than the control group (2.12±0.68 mg/dL), which was statistically significant (p-value of <0.001).
Recent studies suggest that Mg2+ insufficiency occurs in the incidence of CVD, serious cardiac arrhythmias and hypertension [9,10].
A decrease in post-infarction serum magnesium concentration was observed in patients with AMI but not in patients without AMI. According to Salaminia S et al., lowest serum magnesium concentrations were observed with the first 12 to 20 hours after hospitalisation [11].
Two to three-fold increase ventricular arrhythmia was seen in patients with hypomagnesemia than patients with normal serum magnesium [12,13]. Woods K et al., and Rosique-Esteban N et al., suggested that treating patients with IV magnesium decreases the incidence of ventricular arrhythmia [14,15].
Limitation(s)
The study is limited by the small sample size. Further studies should conducted with larger sample size and also AMI patients with higher and normal magnesium levels.
Conclusion(s)
In AMI patients, low serum magnesium levels were observed compared to the control group. However further studies are required to investigate the hypomagnesemia in reducing the mortality rate of coronary heart diseases and sudden cardiac death.
Author Declaration:
Financial or Other Competing Interests: No
Was Ethics Committee Approval obtained for this study? Yes
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. NA
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Aug 03, 2019
Manual Googling: Dec 16, 2019
iThenticate Software: Dec 29, 2019 (16%)
[1]. Taylor EJ, Hypomagnesemia at Dorland’s Medical Dictionary 2011 Philadelphia, PASaunders [Google Scholar]
[2]. Boon NA, Fox KAA, Bloomfield P, Brad Bury A, Cardiovascular disease in Davidson’s Principles and practice of Medicine 2002 19th EditionChurchill Living Stone:420 [Google Scholar]
[3]. Antman EM, Braunwald E, Acute Myocardial infarction in Heart Disease 2001 6th editionPhiladelphiaSaunders:1114-1137.:1171-1172. [Google Scholar]
[4]. Flink EB, Brick JE, Shane RS, Alterations of long-chain free fatty acid and magnesium concentrations in acute myocardial infarctionArch Int Med 1981 141(4):441-43.10.1001/archinte.1981.00340040037014 [Google Scholar] [CrossRef]
[5]. Altura BM, Zhang A, Altura BT, Magnesium hypertensive vascular disease, atherogenesis, subcellar compatmentation of Ca2+ and Mg2+ and vascular contractilityMiner Electrolyte Metab 1993 19(4-5):323-36. [Google Scholar]
[6]. Arsenian MA, Magnesium and cardiovascular diseaseProg Cardiovasc Dis 1993 35(4):271-310.10.1016/0033-0620(93)90008-2 [Google Scholar] [CrossRef]
[7]. Gyamlani G, Parikh C, Kulkarni AG, Benefits of magnesium in acute myocardial infarction: timing is crucialAm Heart J 2000 139(4):70310.1016/S0002-8703(00)90051-6 [Google Scholar] [CrossRef]
[8]. Mhaskar DM, Mahajan SK, Pawar KC, Significance of serum magnesium levels in reference to acute myocardial infarction and role of intravenous magnesium therapy in prevention of cardiac arrhythmias following myocardial infarctionInt J Med Public Health 2013 3(3):187-91.10.4103/2230-8598.118969 [Google Scholar] [CrossRef]
[9]. Kolte D, Vijayaraghavan K, Khera S, Sica DA, Frishman WH, Role of magnesium in cardiovascular diseasesCardiol Rev 2014 22(4):182-92.10.1097/CRD.000000000000000324896250 [Google Scholar] [CrossRef] [PubMed]
[10]. Li J, Zhang Q, Zhang M, Egger M, Intravenous magnesium for acute myocardial infarctionCochrane Database of Sys Rev 2007 (2):CD00275510.1002/14651858.CD002755.pub2 [Google Scholar] [CrossRef]
[11]. Salaminia S, Sayehmiri F, Angha P, Sayehmiri K, Motedayen M, Evaluating the effect of magnesium supplementation and cardiac arrhythmias after acute coronary syndrome: a systematic review and meta-analysisBMC Cardiovasc Disord 2018 18(1):129Published 2018 Jun 2810.1186/s12872-018-0857-629954320 [Google Scholar] [CrossRef] [PubMed]
[12]. Das B, Mishra TK, Prevention and management of arrhythmias in acute myocardial infarctionInternational Journal of Contemporary Medical Research 2016 3(5):1401-05. [Google Scholar]
[13]. Sherer Y, Shoenfeld Y, Shaish A, Levkovitz H, Bitzur R, Harats D, Suppression of atherogenesis in female low-density lipoprotein receptor knockout mice following magnesium fortification of drinking water: the importance of dietPathobiology 2000 68(2):93-98.10.1159/00002811910878506 [Google Scholar] [CrossRef] [PubMed]
[14]. Woods KL, Fletcher S, Roffe C, Haider Y, Intravenous magnesium sulfate in suspected acute myocardial infarction: Results of the second Leicester intravenous magnesium intervention trial (LIMIT-2)Lancet 1992 339(8809):1553-58.10.1016/0140-6736(92)91828-V [Google Scholar] [CrossRef]
[15]. Rosique-Esteban N, Guasch-Ferré M, Hernández-Alonso P, Salas-Salvadó J, Dietary magnesium and cardiovascular disease: A review with emphasis in epidemiological studiesNutrients 2018 10(2):E16810.3390/nu1002016829389872 [Google Scholar] [CrossRef] [PubMed]