Ovarian Cancer (OC) is commonly described as the “silent killer” is the fifth commonest cause of deaths due to cancer in females. It forms 30% of all gynaecological cancers. Serous Epithelial Ovarian Cancer (SEOC) is considered one of the most fatal cancer and accounts for about 90% of the malignant tumours which arise from the ovary [1].
Although carcinoma of the ovary is about ten times less prevalent than cancer breast but it is accompanied with late stage and extra pelvic spread detected in 70-75% of patients. Relapse after operations and chemotherapy and the number of deaths are considered high during the course of the disease [2].
In OC, the rate of survival of patients after 5 years is 25-30%. The mortality rate is still high despite the progress in management of this cancer. Most of the patients with OC have distant spread even during the diagnosis without specific symptoms. The major reasons of failure of the treatment are presence of invasion to the surrounding structures and distant metastasis. Understanding exact molecular basic processes which include proliferation of the tumour, cohesion between cells and spread is important to insure the effective therapeutic treatments of ovarian cancer [3].
Early diagnosis and new therapeutic methods are ineffective due to absence of early stages diagnostic aids for screening and definitive aetiological factors. Histological structure, degree of tumour differentiation and International Federation of Gynaecology and Obstetrics (FIGO) stage are the main criteria for detection of OC prognosis. Such criteria do not always represent the real biological characteristics of tumours, especially their invasive and metastatic features. So, there is urgent need for searching an innovative method to detect the prognosis of OC [4].
Ovarian Serous Carcinoma (OSC) is associated with changes in proliferation, angiogenesis and cell adhesion molecules expression like CD44 that is very important in mechanisms of tumour spread and metastasis. Epithelial-to-Mesenchymal Transition (EMT) is a main patho-physiological method which helps epithelial malignant cells to infiltrate the surrounding structures. Loss of cohesion between cells causes spread of individual malignant cells then invading blood stream and lymphatic [5].
Theory of Cancer Stem Cells (CSCs) believes that CSCs forms 0.1% of the all amount of malignant cells that have the capacity of renewing themselves and carcinogenicity, and have an important function in distant metastasis of the tumour, resistance to chemotherapy and recurrence following therapy in multiple human malignancies like breast and ovarian carcinomas [6].
One of the hot topics recently is targeting CSCs to prevent recurrence and increasing the survival rates of cancer patients. Targeting CSC specific markers is very easy and important way to identify putative CSCs. One of these markers raised up to identify ovarian CSCs is Cluster of Differentiation 44 (CD44) [7].
CD44, was firstly known as adhesion molecule that is present on cell membrane. Mechanisms of adhesion are considered very important in the whole steps of the metastatic cascades, and presence of CD44 expression in invading side of the tumour was used as prognostic indication of lymph node and distant metastases [8,9].
CD44 is a cell membrane protein located on chromosome 11 in human, which mediates cell-cell interactions between cells, in addition cell adhesion and migration. CD44 has a role in numerous processes like tumour metastasis, haematopoiesis, and stimulation of lymphocyte, recycling and homing. CD44 is considered as hyaluronic acid receptor and reacts with other reagents like, matrix metalloproteinases, collagens and osteopontin. Recently CD44 is applied as a biomarker to recognise CSCs and important factor for prognosis of many malignant tumours. The CSC supposition explains how a sub-population of cells inside the tumour of the patient becomes resistant to treatment, leading to recurrent chemoresistant disease [10].
Cell proliferation has a main function in the behaviour and aggressiveness of OC and also the sensitivity to chemotherapy. Determination of proliferative activity has a diagnostic and prognostic importance and multiple ways are applied to count the proliferation index [11]. Ki-67 antigen is detected in the nucleus and related to proliferation of the cells; it is a simple method for counting the Proliferative Index (PI) of malignant tumours. It is detected through all dynamic steps of the cell division but not in quiescent cells [12].
The objective of this study was to evaluate the immunohistochemical expression of CD44 (stem cell marker) and Ki67 in serous ovarian cancer and their relation to clinical and pathological parameters in an attempt to determine the predictor for their biological behaviour.
Materials and Methods
Patients and Clinical Data
This was a prospective cohort study conducted in Pathology, Gynaecology and Obstetrics and Clinical Oncology departments, Faculty of Medicine, Zagazig University, Egypt. The studied cases were collected from Pathology Department archive in the period from April 2011 to December 2013. The study included 45 Formalin-Fixed and Paraffin-Embedded (FFPE) female ovarian serous cancer tissues including 8 borderline tumours, 13 low grade serous carcinomas and 24 high grade serous carcinomas. This study excluded females with benign or other ovarian cancer and cases with insufficient tissue for staining. Histopathological typing and grading were done using the World Health Organisation classification (WHO) 2014 [13] and clinically staged according to FIGO classification, 2015 [14].
The patients were examined in clinical oncology Zagazig University hospitals where they were offered their treatment in the form of carboplatin - paclitaxel, carboplatin- gemcitabine and ifosfamide-mesna-etoposide as chemotherapy protocols were used. All patients underwent proper history, clinical and radiological examinations. Surgical interventions included optimal and non-optimal surgical resection, complete, incomplete debulking and biopsy through exploration. Follow-up was up to the end of December 2018. We obtained the clinical, pathological and radiological information from the relevant patients’ sheets.
The institutional Review Board of Faculty of Medicine Zagazig University approved this study (No.5604) with informed consent from the patients.
Immunohistochemical Procedures
The sections were de-waxed using xylene and rehydration in alcohol was performed, and then exposed to 0.01 M citrate buffer (pH 6.0) for 30 minutes to retrieve antigens before another treatment. Next a rapid wash in Phosphate Buffered Saline (PBS), the sections were incubated in 0.3% H2O2 for 30 minutes to stop endogenous peroxidase activity (Dako ko411 kit) before blocking the non-specific immunoreactions with 5% horse serum for 2 hours.
Using the manufacturer’s instructions, overnight incubation of the sections with two primary antibodies in a humid atmosphere: mouse monoclonal anti-CD44std (1: 100, clone: 156-3c11. 0.09% sodium azide from Thermo Scientific/Lab Vision Corporation, Fermont, USA) and MIB-1 antibody/monoclonal antibody (Novocastra, code no Ki-67-MM1-R7-C Newcastle. United Kingdom) Novostain. The sections were treated with biotinylated secondary antibodies for 30 minutes, and then followed by avidin-biotin peroxidase complex for another 30 minutes, according to (Universal Detection Kit, Dako, Denmark). At the end, the immune reaction was seen using 3, 3-diaminobenzidine tetra hydrochloride (DAB, Dako K0114 Kit) for 5 minutes. Mayer’s haematoxylin was used as a counterstain for one minute.
All the steps were done at room temperature. Negative control for both markers in which the primary antibody was removed and changed by phosphate buffered saline. In addition, reactive lymph node sections were used as positive control for both markers and were processed in the same staining procedure to precise and standardise the IHC results of both CD44 and Ki67.
Evaluation of Immunohistochemical Staining
The immunostaining was semiquanitatively evaluated by 2 pathologists (TI&SA). CD44 membranous immunostaining was only accepted as positive. The intensity of the stain was calculated as follows: 0, absence of staining: 1) minimal immunoreactivity; 2) intermediate immunostaining; 3) marked staining. The distribution was counted by the percent of positive stained tumoural cells in a scale from 0 to 4, as follows: score 0-≤5% positive stained tumour cells; 1, 6-25% positive stained tumour cells; 2, 26-50% positive tumour cells; 3, 51-75% positive tumour cells; 4, >75% positive tumour cells [15]. The final score was obtained by multiplying the intensity score with the distribution score that detected the level of expression: less than 2, none; 3 up to 5, mild positive; 6 up to 8, moderately positive; 9 up to 12, strongly positive [15].
For Ki67, it showed positive nuclear staining. Simple method was used for assessment of the Ki-67 Labeling Index (LI), it could be considered as high LI (if >50% tumour cells are positive) and low LI (if <50%tumour cells are positive) because there is no standard cut-off point of the level of expression. The staining patterns were focal, heterogeneous and homogeneous [11].
Statistical Analysis
All data were tested using SPSS 22.0 for windows (SPSS Inc., Chicago, IL, USA). For numerical variables, we used mean±SD and median (range), but the qualitative variables were presented as a number or percentage. Pearson’s Chi-square test or Fisher’s-exact test were used to examine the relation between variables. Kaplan-Meier test was used for analysis of OS and DFS, and compared using two-sided exact log-rank test. OS was calculated from the time of diagnosis till the time of death and DFS was calculated from the time of surgery till the time of occurrence of local or distal relapse or the end of the follow-up. Stratification of OS and DFS was applied according to the markers. All tests were two tailed. A p-value <0.05 was accepted significant, p<0.001 means highly significant, while p>0.05 means non-significant.
Results
Patients’ Characteristics
This study was done on 45 cases of epithelial OSC. Mean age of cases was 54.73±8.69 (ranging between 35 and 72 years). In regard to tumour size, it was ranging from 3.8 and 15 cm. Borderline serous carcinoma cases were unilateral in 75% (6/8 cases) while high grade carcinoma cases were bilateral in 58.3% (14/24 cases).
In the present study, 37 serous ovarian carcinoma cases, 13 cases (35.1%) were low grade and 24 cases (64.9%) were high grade were studied. According to FIGO staging system, there were eight tumours stage I (21.6%), 10 tumours were stage II (27%), eight tumours were stage III (21.6%) and 11 tumours (29.7%) were stage IV. Lymph node metastasis was positive in 51.4% (19 cases) while distant metsatasis was present in 29.7% (11 cases).
Results of Immunohistochemical Expression of CD44
Only membranous CD44 immunostaining was considered positive in serous epithelial ovarian cancer cells. CD44 immuno-reactivity was detected in 22 out of 45 tissue sections (48.8%), but not detected in borderline serous carcinoma [Table/Fig-1a-c].
Representative samples of immunohistochemical expression of CD44 and Ki67: a) Borderline serous ovarian tumour showed lack of membranous staining for CD44 (X200); b) A case of low grade serous ovarian carcinoma showed membranous staining for CD44(X400); c) High grade serous ovarian carcinoma, with marked membranous staining for CD44 (X400); d) Borderline serous ovarian tumour showed focal nuclear staining for Ki67 (X200).); e) A case of low grade serous ovarian carcinoma showed heterogeneous nuclear staining for Ki67 (X400; f) High grade serous cancer ovary, with strong diffuse nuclear immunereaction for Ki67 (X200).
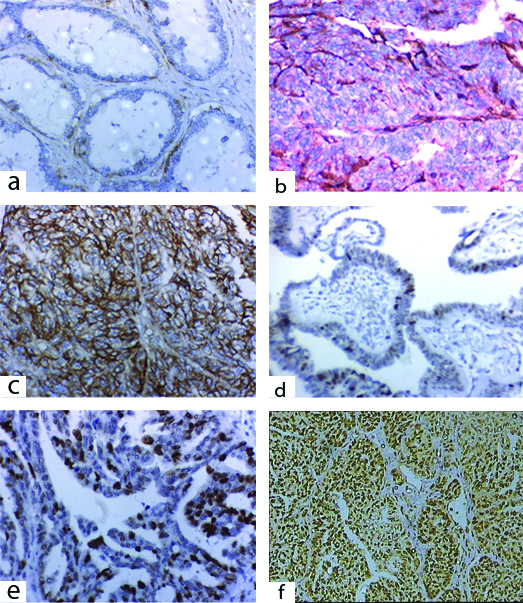
In the studied malignant serous carcinoma, CD44 immunostaining was detected in 59.5% (22/37), it was detected in 23.1% (3/13) in low grade ovarian carcinoma while it was detected in 79.2% (19/24) in high grade ovarian carcinoma. As regard staining pattern, it was weak in 5.4% (2 cases), moderate in 27% (10 cases) and strong in 27% (10 cases). CD44 was expressed in one case of studied stage I (1/8), four cases of studied stage II cases (4/10), six cases of stage III cases (6/8) and 11 cases of stage IV (11/11) this correspond to 12.5% of stage I, 40% of stage II, 75% of stage III and 100% of stage IV.
As regard relationship between clinicopathological features and immunohistochemical staining for CD44 in serous ovarian carcinoma, there was a lack of significant association between patient age and CD44 immunostaining (p=0.118) while the relationship was near the significant level (p=0.052) as regard tumour size.
In ovarian serous cystadenocarcinoma, CD44 was more expressed in patients with high grade and advanced stage with highly statistically significant difference (p=0.001 and p<0.001, respectively). CD44 expression in bilateral cancer with presence of lymph node and distant spread was more than in unilateral tumour not involving lymph node and distant spread (p=0.013, p<0.001 and p=0.001, respectively) [Table/Fig-2,3].
Relation between clinicopathological features and immunohistochemical staining for CD44 & Ki67 in studied ovarian tumours patients (N=45).
| Parameters | Borderline (N=8) | Low grade Cystadenocarcinoma (N=13) | High grade Cystadenocarcinoma (N=24) | p-value |
|---|
| No. | % | No. | % | No. | % |
|---|
| Age (years) |
| Mean±SD | 42.50 | ±6.27 | 46.77 | ±5.86 | 59.04 | ±6.72 | <0.001• |
| Median (Range) | 43 | (33-53) | 46 | (35-56) | 57 | (49-72) | |
| <50 years | 8 | 100% | 6 | 46.2% | 3 | 12.5% | <0.001‡ |
| ≥50 years | 0 | 0% | 7 | 53.8% | 21 | 87.5% | |
| Size (cm) |
| Mean±SD | 5.18 | ±1.53 | 6.03 | ±2.07 | 10.83 | ±2.04 | <0.001• |
| Median (Range) | 5 | (3.50-7.50) | 6 | (3.80-12) | 10 | (7.50-15) | |
| <10 cm | 8 | 100% | 12 | 92.3% | 8 | 33.3% | <0.001‡ |
| ≥10 cm | 0 | 0% | 1 | 7.7% | 16 | 66.7% |
| Laterality |
| Unilateral | 6 | 75% | 8 | 61.5% | 10 | 41.7% | 0.205‡ |
| Bilateral | 2 | 25% | 5 | 38.5% | 14 | 58.3% |
| Lymph node |
| Node negative | 8 | 100% | 13 | 100% | 5 | 20.8% | <0.001‡ |
| Node positive | 0 | 0% | 0 | 0% | 19 | 79.2% |
| CD44 expression |
| Negative | 8 | 100% | 10 | 76.9% | 5 | 20.8% | <0.001‡ |
| Positive | 0 | 0% | 3 | 23.1% | 19 | 79.2% |
| Negative | 8 | 100% | 10 | 76.9% | 5 | 20.8% | <0.001‡ |
| Weak | 0 | 0% | 2 | 15.4% | 0 | 0% | |
| Moderate | 0 | 0% | 1 | 7.7% | 9 | 37.5% | |
| Strong | 0 | 0% | 0 | 0% | 10 | 41.7% | |
| Ki67 expression |
| Negative | 6 | 75% | 8 | 61.5% | 2 | 8.3% | <0.001‡ |
| Positive | 2 | 25% | 5 | 38.5% | 22 | 91.7% | |
| Negative | 6 | 75% | 8 | 61.5% | 2 | 8.3% | 0.001‡ |
| Low | 2 | 25% | 3 | 23.1% | 7 | 29.7% | |
| High | 0 | 0% | 2 | 15.4% | 15 | 62.5% | |
| Ki67 pattern |
| No | 6 | 75% | 8 | 61.5% | 2 | 8.3% | <0.001‡ |
| Focal | 2 | 25% | 2 | 15.4% | 1 | 4.2% | |
| Heterogenous | 0 | 0% | 3 | 23.1% | 8 | 33.3% | |
| Diffuse | 0 | 0% | 0 | 0% | 13 | 54.2% | |
Categorical variables were expressed as number (percentage); Continuous variables were expressed as mean±SD & median (range); •Kruskal Wallis H test; ‡Chi-square test; p<0.05 is significant
Relationship between clinicopathological features and immunohistochemical staining for CD44 & Ki67 in ovarian cystadenocarcinoma patients (N=37).
| Characteristics | All | CD44 expression | p-value | Ki67 expression | p-value |
|---|
| (N=37) | Negative (N=15) | Positive (N=22) | Negative (N=10) | Positive (N=27) |
|---|
| No. | % | No. | % | No. | % | No. | % | No. | % |
|---|
| Age |
| <50 years | 9 | 24.3% | 6 | 66.7% | 3 | 33.3% | 0.118‡ | 5 | 55.6% | 4 | 44.4% | 0.041‡ |
| ≥50 years | 28 | 75.6% | 9 | 32.1% | 19 | 67.9% | | 5 | 17.9% | 23 | 82.1% | |
| Size (cm) |
| <10 cm | 20 | 54.1% | 11 | 55% | 9 | 45% | 0.052‡ | 7 | 35% | 13 | 65% | 0.288‡ |
| ≥10 cm | 17 | 45.9% | 4 | 23.5% | 13 | 76.5% | | 3 | 17.6% | 14 | 82.4% | |
| Pathological type |
| Low grade | 13 | 35.1% | 10 | 76.9% | 3 | 23.1% | 0.001‡ | 8 | 61.5% | 5 | 38.5% | 0.001‡ |
| High grade | 24 | 64.9% | 5 | 20.8% | 19 | 79.2% | | 2 | 8.3% | 22 | 91.7% | |
| Laterality |
| Unilateral | 18 | 48.6% | 11 | 61.1% | 7 | 38.9% | 0.013‡ | 8 | 44.4% | 10 | 55.6% | 0.029‡ |
| Bilateral | 19 | 51.4% | 4 | 21.1% | 15 | 78.9% | | 2 | 10.5% | 17 | 89.5% | |
| Lymph node |
| Node negative | 18 | 48.6% | 13 | 72.2% | 5 | 27.8% | <0.001‡ | 9 | 50% | 9 | 50% | 0.003‡ |
| Node positive | 19 | 51.4% | 2 | 10.5% | 17 | 89.5% | | 1 | 5.3% | 18 | 94.7% | |
| Distant met. |
| Absent | 26 | 70.3% | 15 | 57.7% | 11 | 42.3% | 0.001‡ | 10 | 38.5% | 16 | 61.5% | 0.018‡ |
| Present | 11 | 29.7% | 0 | 0% | 11 | 100% | | 0 | 0% | 11 | 100% | |
| FIGO stage |
| Stage I | 8 | 21.6% | 7 | 87.5% | 1 | 12.5% | <0.001§ | 6 | 75% | 2 | 25% | <0.001§ |
| Stage II | 10 | 27% | 6 | 60% | 4 | 40% | | 3 | 30% | 7 | 70% | |
| Stage III | 8 | 21.6% | 2 | 25% | 6 | 75% | | 1 | 12.5% | 7 | 87.5% | |
| Stage IV | 11 | 29.7% | 0 | 0% | 11 | 100% | | 0 | 0% | 11 | 100% | |
| CD44 expression |
| Negative | 15 | 40.5% | | | | | | 8 | 53.3% | 7 | 46.7% | 0.006‡ |
| Positive | 22 | 59.5% | | | | | | 2 | 9.1% | 20 | 90.9% | |
| Ki67 expression |
| Negative | 10 | 27% | 8 | 80% | 2 | 20% | 0.006‡ | | | | | |
| Positive | 27 | 73% | 7 | 25.9% | 20 | 74.1% | | | | | | |
Categorical variables were expressed as number (percentage); Continuous variables were expressed as mean±SD & median (range); ‡ Chi-square test; §Chi-square test for trend; p<0.05 is significant
Results of Immunohistochemical Expression of Ki67
Ki67 immunostaining was detected in the nuclei of the epithelial cancer cells of the ovary. Ki67 positive stained sections were observed in 27 cases (60%) of the studied serous ovarian tumours, with high Ki67 Labeling Index (LI) in 37.8% (17/45) and low Ki67 LI in 22.2% (10/45) of cases. It was expressed in 25% (2/8) of borderline serous ovarian tumours, 38.5% (5/13) of low-grade serous tumours and 91.7% (22/24) of high grade serous tumour [Table/Fig-1d-f].
According to FIGO stages, the Ki67 positivity has been detected in 25% of stage I, 70% of stage II, 87.5% stage III, 100% stage IV.
In this study, diffuse pattern was found in high grade serous carcinoma in 54.2% of cases while it was heterogenous in low grade serous carcinoma in 23.1% of cases and focal pattern (isolated stained cells) in borderline tumour in 25% of cases.
Significant association was found between patient age and Ki67 immunostaining (p=0.04) while the relationship was insignificant (p=0.288) as regard tumour size.
Ki67 immunostaining was noted with increased grade and late stage which was statistically significant (p=0.001 and p<0.001, respectively), also significant relationship was found between Ki67 expression and bilateral cancer with positive lymph node and distant spread (p=0.029, p=0.003, p=0.018, respectively) [Table/Fig-2,3].
Associations between CD44 Expression and Ki67 in the Examined Carcinoma
A positive association was found between CD44 and Ki67 expression, where Ki67 positivity was observed in 90.9% (20 cases out of 22 cases) of CD44 positive tumours and 46.7% (7 cases out of 15 cases) of CD44 negative tumours. Whereas, 53.3% of Ki67 negative tumours were CD44 negative (p-value=0.006) [Table/Fig-3].
Associations between CD44 Expression and Ki67 and Outcome in the Ovarian Cystadenocarcinoma Cases (N=37)
DFS and OS were used to analyse survival in the present study. The patient group with CD44 and Ki67 positive expression level in OSC had a significantly shorter DFS than the patient group with negative expression of CD44 and Ki67 (p=0.020 and p=0.002, respectively) [Table/Fig-4,5].
Relationship between immunohistochemical staining for CD44 & Ki67 and outcome in ovarian cystadenocarcinoma patients (N=37).
| Outcome | All | CD44 expression | p-value | Ki67 expression | p-value |
|---|
| (N=37) | Negative (N=15) | Positive (N=22) | Negative (N=10) | Positive (N=27) |
|---|
| No. | % | No. | % | No. | % | No. | % | No. | % |
|---|
| Response |
| CR | 17 | 45.9% | 13 | 86.7% | 4 | 18.2% | 0.001‡ | 9 | 90% | 8 | 29.6% | 0.001‡ |
| PR | 4 | 10.8% | 1 | 6.7% | 3 | 13.6% | | 0 | 0% | 4 | 14.8% | |
| SD | 1 | 2.7% | 0 | 0% | 1 | 4.5% | | 1 | 10% | 0 | 0% | |
| PD | 15 | 40.5% | 1 | 6.7% | 14 | 63.6% | | 0 | 0% | 15 | 55.6% | |
| Relapse | (N=17) | (N=13) | (N=4) | | (N=9) | (N=8) | |
| Absent | 9 | 52.9% | 9 | 69.2% | 0 | 0% | 0.029‡ | 8 | 88.9% | 1 | 12.5% | 0.003‡ |
| Present | 8 | 47.1% | 4 | 3.8% | 4 | 100% | | 1 | 11.1% | 7 | 87.5% | |
| DFS |
| Mean (months) (95%CI) | 32.82 months (30.73-34.91) | 33.54 months (31.01-36.06) | 30.50 months (28.03-32.97) | 0.020† | 35.33 months (34.10-36.57) | 30 months (26.75-33.25) | 0.002‡ |
| 1-year DFS | 100% | 100% | 100% | | 100% | 100% | |
| 2-year DFS | 94.1% | 92.3% | 100% | | 100% | 87.5% | |
| 3-year DFS | 52.9% | 69.2% | 0% | | 88.9% | 12.5% | |
| Mortality | (N=37) | (N=15) | (N=22) | | (N=10) | (N=27) | |
| Absent | 12 | 32.4% | 11 | 73.3% | 1 | 4.5% | <0.001‡ | 8 | 80% | 4 | 14.8% | <0.001‡ |
| Present | 25 | 67.6% | 4 | 26.7% | 21 | 95.5% | | 2 | 20% | 23 | 85.2% | |
| OS |
| Mean (months) (95%CI) | 24.22 months (20.58-27.85) | 33.20 months (29.84-36.56) | 18.09 months (14.09-22.09) | <0.001‡ | 33.50 months (29.61-37.39) | 20.78 months (16.71-24.84) | 0.001‡ |
| 1-year OS | 70.3% | 93.3% | 54.5% | | 100% | 59.3% | |
| 2-year OS | 51.4% | 86.7% | 27.3% | | 90% | 37% | |
| 3-year OS | 32.4% | 73.3% | 4.5% | | 80% | 14.8% | |
Continuous variables were expressed as mean (95% CI); categorical variables were expressed as number (percentage); ‡Chi-square test; †Log rank test; p<0.05 is significant
Kaplan Meier plot, Left panel: Disease Free Survival, Right panel: Overall Survival; (a and d) All studied patients, (b and e) Stratified by CD44 expression and (c and f) Stratified by Ki67 expression.
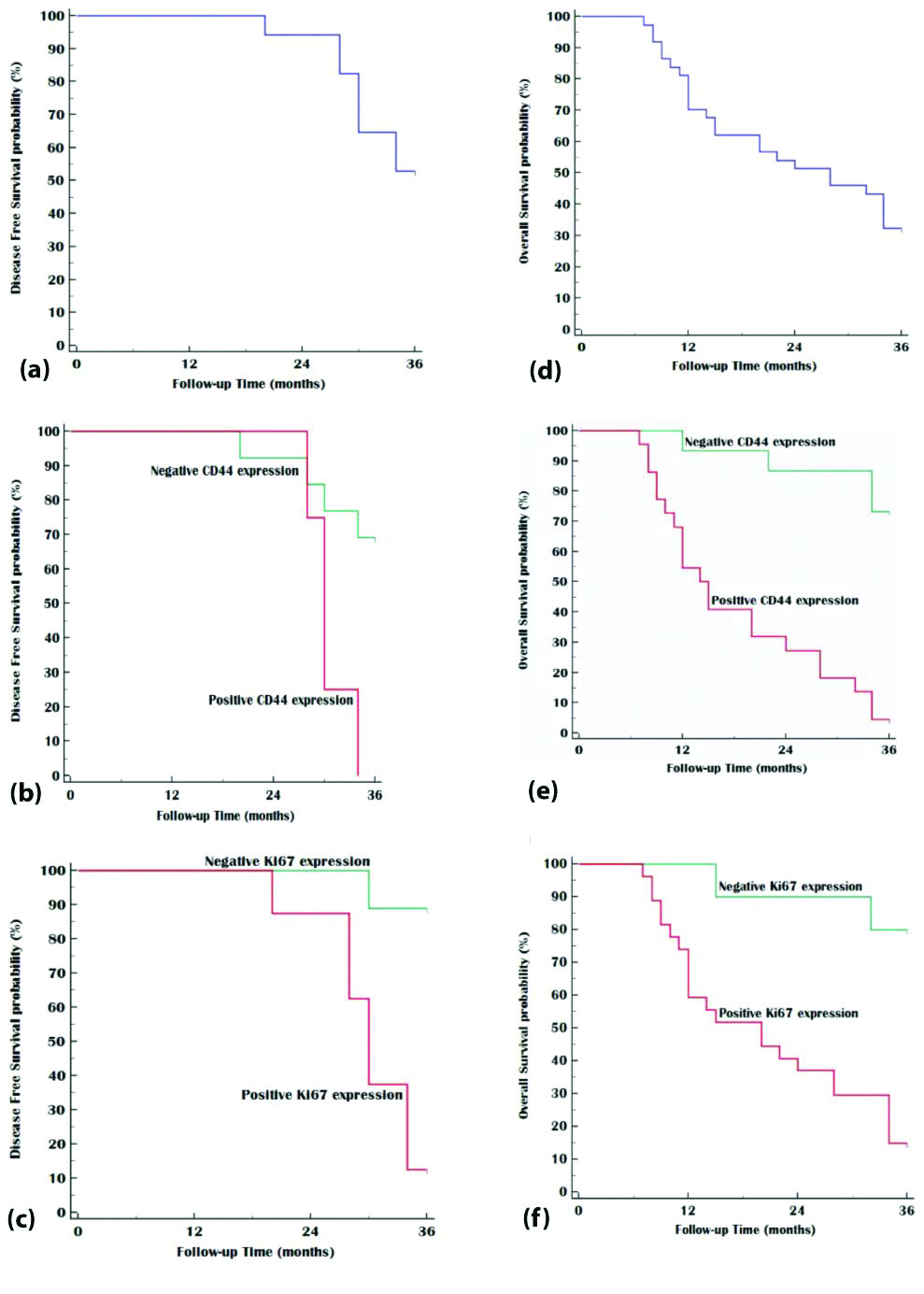
Patients with positive CD44 and Ki67 expression were associated with significant progressive disease (p=0.001). Three year DFS was worse in patients with positive CD44 expression and high Ki67 expression (p=0.020, p=0.002, respectively). Also, 3 year OS was worse in patients with positive CD44 expression and high Ki67 expression (p<0.001, p=0.001, respectively).
Discussion
Although ovarian carcinoma is considered one of the extremely sensitive solid tumours to chemotherapy, it has high lethal rate worldwide. There is a minimal group of cells, named as CSCs that do not respond to therapy, then survives and initiates new tumours leading to recurrence, so searching new CSCs markers is mandatory to identify these cells to prevent relapse and improve survival. CD44, one of the cell-surface adhesion molecules involved in multiple pathological and physiological processes. Studies have suggested that CD44 overexpression promotes cells migration and metastasis for human solid tumours, including ovarian carcinoma. Recently, it has been known as a marker of CSCs [15,16].
Ki67 has been identified as a prognostic marker in many tumours because it can detect the proliferative activity of tumour cells. Its expression is linked to poor prognostic variables and metastasis [11].
The present study examined the prognostic significance of immunostaining of CD44 (stem cell marker) and Ki67 in borderline and malignant serous ovarian tumours in relation to clinicopathological variables and patients survival.
This work was performed on 45 patients diagnosed as serous ovarian tumours, 8 borderline tumours, 13 low grade ovarian carcinoma and 24 high grade ovarian carcinomas. The age range of the examined cases was 35-72 years and mean age was 54.73±8.69 years, the mean age was more in high grade carcinoma than low grade and borderline tumours p<0.001. The range of tumour diameter was 5 cm in borderline, 6 cm in low grade and 10 cm in high grade tumours. These findings were similar to that of Popa M et al., [17].
This study noticed that the frequency of bilateral tumours in borderline, low grade and high-grade ovarian carcinoma cases was 25%, 38.5% and 58.5%, respectively. These results near the findings of Popa M et al., they revealed that high grade serous carcinoma was bilateral in 50% of cases [18].
In the studied malignant serous carcinoma CD44 immunostaining was detected in 59.5%; it was detected in 23.1% of low grade ovarian carcinoma while it was detected in 79.2% of high grade ovarian carcinoma, but not detected in borderline serous carcinoma, so CD44 expression is linked to the pathogenesis of malignant serous carcinoma. These findings were in line with that of Zheng J et al., who revealed that the level of CD44 expression was closely related to epithelial ovarian cancer as it was detected in 64% of cases of ovarian cancers and not detected in normal ovarian epithelial tissue [15]. Another study reported that CD44 immunostaining was positive in 50% of high-grade carcinoma cases [18]. Zhanga J et al., reported that CD44 expression was detected in 38% of the cancer ovary cases [19].
When analysing the relationship between CD44 expression and clinicopathological data, high immunostaining of CD44 in serous carcinoma of the ovary was significantly associated with high grade, advanced stage with lymph node and distant metastasis, p=0.001, these results showed that CD44 expression could be involved in disease progression. These findings were similar to the results of Zheng J et al., and Zhanga J et al., [15,19], but in contrary to those of Popa M et al., who found that CD44 expression was not associated with bilateral tumour or with late stage malignancy [18]. Ryabtseva OD et al., had found the increased adhesive characters of serous ovarian malignant cells that may be important for determination of prognosis of ovarian cancer and presence of metastasis [8]. Vos MC et al., found that in late stage serous carcinoma patients, CD44 was accompanied with vimentin immunostaining and consequently EMT-like alterations [20].
Shi Y and Jiang H conduced meta-analysis to examine the correlation between CD44 and multiple clinico-pathological variables of ovarian cancer, whose results demonstrated that CD44 expression is not significantly correlated with the grade of the tumour, patients age, residual tumour mass or chemotherapy response but CD44 expression is significantly correlated with lymph node metastasis and tumour TNM staging [21]. Also, Lin J and Ding D found that CD44v6 immunostaining in cancer ovary was correlated significantly with advanced TMN stage. They did not found correlation between CD44 positivity and grade of the tumour, lymphatic invasion, patients’ age, remaining masses or chemotherapy response and concluded that CD44 immunostaining can be applied in routine histopathological examination of ovarian cancer to detect the future outcome [22].
This study found, Ki67 positive immunostaining in 60% of the studied serous ovarian tumours. It was detected in 25% of borderline serous ovarian tumours, 38.5% of low-grade serous tumours and 91.7% of high-grade serous tumour. These findings near that of Giurgea LN et al., who reported in their study that Ki67 expression was detected in 61.53% of investigated malignancies, especially in advanced stages but borderline and benign tumours showed decreased expression in 13.3% and 9.09%, respectively [12].
In the current study, we noticed the diffused pattern of Ki67 expression in high grade serous carcinoma in 54.2% of cases while it was heterogenous in low grade serous carcinoma in 23.1% and focal pattern (isolated stained cells) in borderline tumour in 25% of cases, in accordance with Giurgea LN et al., and other studies, who reported that in low-grade serous carcinoma, there was moderate heterogeneous expression but in high grade carcinomas, they found marked diffuse expression. While borderline tumours revealed heterogeneous expression in lower than 10% of tumour [11,12,23].
In this work, we found high Ki67 LI in 42.5% and low Ki67 LI in 25% of cases, in high grade serous carcinoma we found high Ki67 LI in 62.5% of cases, this was similar to previous study which reported that SEOC showed high Ki-67 LI than benign and borderline tumours [24]. Popa M et al., had shown Ki67 index >80% was detected in 30% of tumours of high-grade ovarian carcinoma [18]. Chen M et al., found that median Ki67 expression level was 40% in cases of High Grade Serous Carcinoma [25].
In the current study, Ki67 immunostaining was detected in high grade and late stage ovarian carcinomas which was statistically significant (p=0.001 and p<0.001, respectively), also the relationship between Ki67 expression and bilateral cancer with positive lymph node and distant metastasis was significant (p=0.029, p=0.003, p=0.018, respectively) this is similar to the another studies, who supposed that Ki67 might be implicated in the progress of epithelial cancer ovary and the prognosis of the patients [11,23,26-29]. While Chen M et al., found that Ki67 expression was not correlated with advanced disease in HGSC, because they did not found correlation between Ki67 immunostaining and tumour stage or lymph node spread [25].
In this study, a direct relation between CD44 and Ki67 expression was found, where Ki67 positivity was observed in 90.9% of CD44 positive tumours (p-value =0. 006). The same findings were declared by Parte CS et al., who reported that CD44 immunostained cells showed positive expression of Ki67 marker [30].
DFS and OS were used to analyse survival in present study. The patient group with CD44 and Ki67 positive expression level in ovarian serous carcinoma had a significantly shorter 3-year DFS than the patient group with negative staining of CD44 and Ki67 (p=0.020 and p=0.002, respectively). Shi Y and Jiang H reported that CD44 positivity was significantly correlated with low OS for ovarian cancer cases [21]. Lin J and Ding D found that cancer ovary cases that showed CD44 expression has poor outcome than cases with absence of CD44 immunostaining [22].
Elzarkaa AA et al., reported in their study that CD44 expression participates in the occurrence of resistance to carboplatin in late SEOC, and leading to poor outcome for patients, but it is not predicting survival or recurrence [31].
This result was in contrary to Zhanga J et al., who found in their study that CD44 positivity was not correlated with OS (p=0.529) or DFS (p=0.218). They proposed that CD44 expression cannot be applied as biomarker of cancer ovary outcome and concluded that CD44 positive reactivity cannot predict the prognosis but related to increased grade and late stage cancer ovary [19]. Multiple studies have proposed that the OC patients with CD44 positive expression have shorter progression-free survival than patients that did not show CD44 expression, but some studies have revealed that marked CD44 expression is linked to good OC outcome. In contrast, other studies did not find any relation between CD44 expression and prognosis of OC [32].
Mahadevappa A et al., and others reported that the PI can be used to predict patients’ outcome in epithelial ovarian cancer. Patients with intense Ki-67 expression are associated with low median survival than patients with low Ki-67 expression [11,23,28,29]. In contrast, Chen M et al., found that in HGSC, significant correlation was obtained between low Ki67 expression (<40%) and platinum resistance and decreased survival [25]. Darb-Esfahani S et al., reported that the Ki67 LI was high but the relation was not significant (p=0.910) in control cases and patients who survive for long time (median=39.8 versus 38.0%) [33].
Discrepancy between studies may be due to variable number of patients, choosing different cut-off points and scoring system for reagents staining evaluation, using variable antibodies and detection or technical processes.
Limitation(s)
There were some limitations as small numbers of cases, financial problems and difficulties in follow-up of patients in this study, so further studies on a wide scale of patients are recommended.
Conclusion(s)
CD44 and Ki67 expression were related to increased grade and late stage serous ovarian carcinoma significantly, and their high expressions were associated with poor prognosis. CD44 may be more specific CSCs marker of HGSC ovarian cancer. In addition, because of CD44 was specifically located in cancer cells rather than borderline serous tumour, it can be an appropriate target therapy marker focused on CSCs of HGSC.