Hydatid Cyst of the Thyroid Gland: A Case Report
Reema Abdul Rahman Al Gunaid1, Wael Abdu Thabet2
1 Assistant Professor, Department of Pathology, University of Science and Technology, Sana’a, Yemen.
2 Phd Student, Department of Pathology, Faculty of Medicine, Cairo University, Egypt.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Reema Abdul Rahman Al Gunaid, 60 Street, Sana’a, Yemen.
E-mail: r.algoneed@ust.edu
Hydatid disease is a zoonotic infestation caused by the genus Echinococcus. It is still widespread in agricultural communities. It is common in temperate and sheep raising countries of the world where it causes a significant public health problem. It is a chronic disease and cyst can be presented in different organs. In humans, hydatid cyst develops most often in the liver (65%) and lungs (25%). Other organs affected occasionally include the brain, muscle, kidney, heart, pancreas, adrenal, and thyroid gland. Involvement of the thyroid gland by hydatid cyst is rare. It is most often asymptomatic or present with anterior neck swelling or rarely dysphagia or dyspnoea. This case report explains our experience with a patient suffering from hydatid cyst in the thyroid.
Echinococcosis, Neck swelling, Thyroid nodule
Case Report
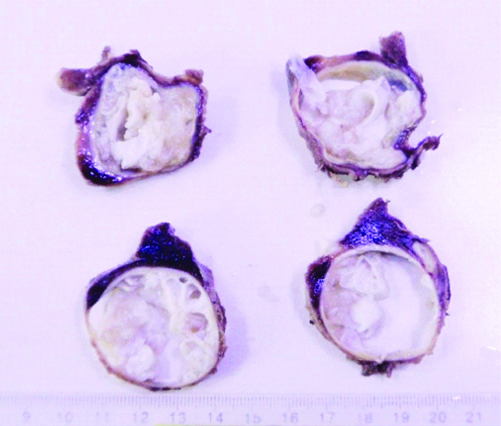
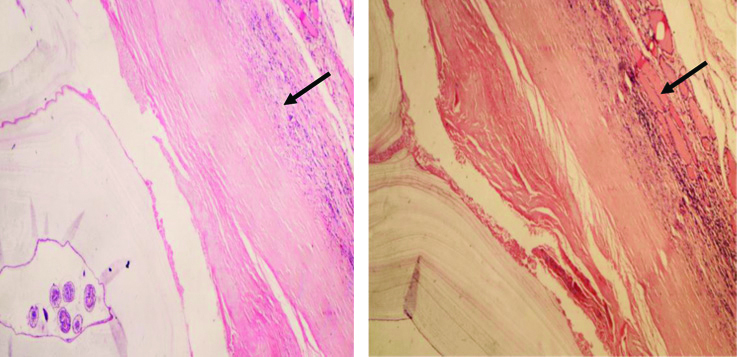
A 60-year-old female patient presented to our clinic with swelling in front midline of the neck since two years. The swelling had been there since 2017, but it had increased in size recently and was associated with hoarseness and sore throat. She lived in a rural area of Yemen and had a history of animal contact. On physical examination, a well-circumscribed, approximately 4×4 cm mass was observed in the left lobe of the thyroid. The mass was non-tender on palpation. Other systemic examinations were normal and no other physical abnormalities or features, suggestive of thyroid over activity were noted. Ultrasonography (USG) of the gland revealed a large lobulated cystic nodule in the left thyroid lobe of size 5×4×3 cm. The function of thyroid gland was normal and Fine Needle Aspiration Biopsy (FNAB) result reported a hypocellular smear showing few follicular cells with round regular nuclei and mild inflammatory cells. The provisional diagnosis was colloid cyst. A total lobectomy of left lobe of thyroid was carried out and specimen was sent for pathologic examination. Gross examination of the thyroid lobe showed that it was a cystic lesion, measuring 6×4×3 cm [Table/Fig-1,2]. Histopathological examination showed cystic lesion formed of three layers: the outermost layer formed of compressed thyroid parenchyma, with dense chronic inflammation and interstitial fibrosis, the middle laminated, cellular membrane and the inner germinal layer contained scolices and daughter cysts [Table/Fig-3,4,5 and 6]. Postoperative computed tomography scans of the head, throrax and abdomen showed no hydatid cysts in other organs. The patient continued to receive 400 mg/day albendazole treatment for two months postoperatively. The patient is being followed-up by repeated examination at 24 months without any recurrence of hydatid disease.
Total left thyroid lobectomy.

Cut section showing cystic lesion, measuring 6×4×3 cm.
Hydatid cyst fibrous wall containing chronic inflammation and surrounded by thyroid compressed follicles (H&E, 100X).
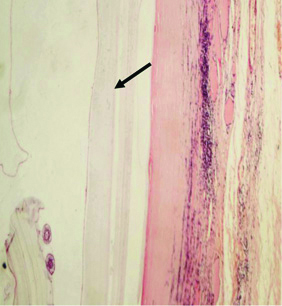
Hydatid cyst showing innermost germinal layer (H&E, 100X).
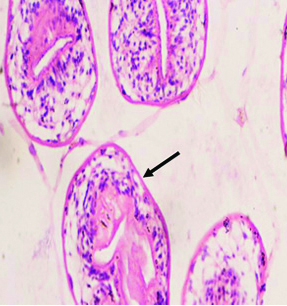
Photograph showing daughter cysts (H&E, 400X).
Discussion
Hydatidosis or cystic hydatid disease is an endemic parasitic disease seen in some parts of the world such as the Mediterranean countries, South America, Middle East, India, Australia, Iceland, New Zealand, and South Africa. It is caused by larvae of tape worm called Echinococcus [1]. Hydatid disease can occur in any part of the body but the most frequently affected sites are the liver, which is considered the first line of defense and the most common organ involved by the disease (75%), followed by lungs (15%). Other affected sites include heart, muscles, brain and kidneys. Head and neck hydatid disease is uncommon, even in countries where echinococcosis is endemic [2]. In this case report, the primary focus was thyroid tissue and there was no evidence of any other organs of hydatid cyst disease.
Hydatid cyst disease (cystic echinococcosis) is one of the major public health problems present in many regions of the world and the ovine and bovine animals are the primary source of infection [3]. The intermediate host is human. The eggs of a parasite that enters the body is hatched in small intestine then transported to the liver through the portal vein or lymphatic system, forming cystic lesions [4]. Other organs of the body such as heart, brain, kidneys, bones, muscles, and pancreas can be affected following a haematogenous spread [5]. High circulatory flow rate of the thyroid gland may play a role in the development of the thyroid hydatid cyst. However, the small diameter of the thyroid vessels together with their position at a right angle to the carotids explains the low incidence of the disease [6].
Mostly, hydatid cysts are asymptomatic and grow slowly. However, symptoms may appear depending on the location and size of the cyst. The cyst can be attached to the oesophagus producing dysphagia, or to the trachea producing dyspnoea [1]. Some common and serious complications of the disease are cyst rupture and consequent anaphylaxis, infection and abscess formation, organ damage and secondary cyst formation [2].
The diagnosis of hydatid cyst disease depends mainly on the patient clinical history, radiological features and serologic tests. On clinical examination the differential diagnosis include benign conditions like branchial cyst and sebaceous cyst in neck. Radiographic tests most commonly used are USG, Computed Tomography (CT), and Magnetic Resonance Imaging (MRI). Although homogeneous appearance of cystic echinococcosis makes radiological diagnosis more difficult, the definitive diagnosis for many cases of hydatid cyst is still possible using radiological methods mentioned above [7].
USG is very useful in showing the daughter vesicles, which is crucial to a preoperative diagnosis of hydatid disease. CT and MRI are effective in advanced diagnosis when the relationship between cystic lesions and the surrounding structures cannot be clearly shown by USG [8]. Serologic examinations have limited use in diagnosis of hydatid disease because of low diagnostic sensitivity and specificity [7]. FNA has a risk of spreading cyst fluid or releasing an anaphylactic shock so it is not recommended in hydatid disease, although there is only one report in the literature mentioning allergic reaction after FNA [9]. The main treatment for hydatid cyst is surgery [10]. Medical treatment is not effective without surgery. Surgical procedure is intended to completely remove the cyst and prevent spread of its content. Medical treatment with albendazole and mebendazole can be used in rare cases if surgery may not be possible because of the debilitated condition of the patient or the location of the cyst, although many adverse reactions of the surgery have been reported and the unpredictable outcome has often been reported [2]. The patient must be followed-up for years because anti-parasite drugs eliminate live parasites and prevent contamination by contents of the cyst during surgery, rather than a cure [1].
Conclusion(s)
Thyroid gland hydatid cyst is rare; however, it should be involved in the differential diagnosis of every cystic lesion, especially where hydatidosis is endemic. Imaging methods as USG, CT, MRI are most commonly used for evaluation of thyroid nodules and the surgeon must take in account the possibility of hydatid disease. Histopathological examination of surgical specimen is mandatory in all cases for accurate diagnosis.
Author Declaration:
Financial or Other Competing Interests: No
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Oct 07, 2019
Manual Googling: Dec 11, 2019
iThenticate Software: Dec 09, 2019 (9%)
[1]. Eshraghi M, Shahmoradi L, Ghoddoosi M, Sadati SJA, Diagnosis of primary hydatid cyst of thyroid gland: A case reportBiomol Concepts 2019 10:106-10.10.1515/bmc-2019-001331199755 [Google Scholar] [CrossRef] [PubMed]
[2]. Sultana N, Shah W, Ullah S, Ali M, Basharat S, Primary hydatid cyst of the thyroid gland: A case reportAnn Clin Pathol 2016 4(3):1070 [Google Scholar]
[3]. Akbulut S, Demircan F, Sogutcu N, Hydatid cyst disease of the thyroid gland: Report of two casesInt Surg 2015 100(4):643-47.10.9738/INTSURG-D-14-00124.125598424 [Google Scholar] [CrossRef] [PubMed]
[4]. Bartin MK, Yilmaz EM, Arslan H, Tekeli AE, Karatas S, A case of primary hydatid cyst in the thyroid glandUlus Cerrahi Derg 2015 31(2):94-95.10.5152/UCD.2014.266826170748 [Google Scholar] [CrossRef] [PubMed]
[5]. Azendour I, Boulaich M, Ayoubi A, Oujilal A, Essakalli L, Kzadri M, Primary hydatid cyst of the thyroid glandInt J Otolaryngol 2011 2011(10):71308910.1155/2011/71308923008718 [Google Scholar] [CrossRef] [PubMed]
[6]. TieminI J, QiangI G, Bo R, Ruiqing Z, Tuerganaili A, Yingmei S, Hydatid cyst of the thyroid gland with tracheal fistula: A case report and review of the literatureExp Ther Med 2019 18:573-79. [Google Scholar]
[7]. Ismet O, Cigdem O, Sukru O, Mustafa Y, Primary echinococcus cyst of the thyroid: A case reportActa Med Iran 2011 49(4):262-64. [Google Scholar]
[8]. Bouomrani S, Souissi O, Regaieg N, BenHamed M, Primary hydatid cyst of the thyroid gland revealed by primary hypothyroidismJ Inf Dis Trav Med 2018 2(3):000121 [Google Scholar]
[9]. Dey AK, Mandal PK, Dutta A, Pramanik S, Maji S, Chakraborti N, A case of hydatid cyst of thyroid glandAsian J Med Sci 2014 5:143-45.10.3126/ajms.v5i2.8830 [Google Scholar] [CrossRef]
[10]. Oksuz S, Pektas E, Yavuz M, Aksungur N, Cayir Y, Akcay MN, An unusual cause of hoarseness: Hydatid cyst of the thyroidTrop Biomed 2013 30(4):642-44. [Google Scholar]