Regeneration Potential of Pulp: A Case Report
Rohith Shinde1, Pranitha Shinde2, Sanganand Gavle3, Madhuri Reddy4, T Sai Pravallika5
1 Endodontist, Department of Conservative Dentistry and Endodontics, Family Dental Care, Bodhan Rural Nizamabad, Telangana, India.
2 Postgraduate, Department of Periodontics, HKE’s S Dental College, Kalaburagi, Karnataka, India.
3 Endodontist, Department of Conservative Dentistry and Endodontics, Elite Dental Care, Athapur, Hyderabad, India.
4 Postgraduate, Department of Periodontics, MNR Dental College, Sangareddy, Telangana, India.
5 Clinician, Department of Public Health Dentistry, Family Dental Care, Kukatpally, Hyderabad, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Rohith Shinde, Department of Conservative Dentistry and Endodontics, Family Dental Care, Beside SBI Bank, Main Road, 1st Floor, Bodhan Rural Nizamabad, Telangana, India.
E-mail: intellects19@yahoo.com
Regenerative endodontics is a boon to dentistry as it restores the non-vital tooth with a less invasive procedure. Revascularization helps in restoration of teeth with medicaments having antimicrobial properties. There is a substantial literature supporting revascularization using this technique. Hence the present case report was documented with the objective of presenting the regeneration potential of pulp. A 15-year-old male patient presented with complaints of pain in upper right back tooth region since last one month. The pain aggravated on biting and during night. The patient had a history of previous visit to satellite clinic followed by emergency access opening. The tooth was tender on percussion. Pulp vitality tests gave a negative response. The tooth was diagnosed as apical periodontitis with immature apex. Under strict aseptic environment after administration of Local anaesthesia (LA), access cavity was opened. The canal was then dried and temporarily restored with Triple Antibiotic Paste (TAP) and sealed with 4 mm of Intermediate Restorative Material (IRM). It was found that there was narrowing of the apical area after 3 months follow-up and after 5 months follow-up, there was complete apical closure. Hence, tooth with immature apex with viable radicular pulp should not be treated with aggressive procedures, as root canal treatment. So, in such cases application of TAP (Triple Antibiotic Paste) followed by revascularization should be done and follow-up of the case must be done till the apex has been completely closed.
Apical periodontitis, Pulp necrosis, Triple antibiotic paste
Case Report
A 15-year-old male patient presented to the department of conservative dentistry and endodontics, MNR dental college and hospital with the complaints of pain in upper right back tooth region, since the last one month. The patient complained of dull, localised pain which was aggravated on biting and on lying down at night. The patient previously visited satellite clinic where emergency access opening was done. The tooth was tender on percussion. Pulp vitality tests like cold test with endo ice spray and an electric pulp testing done gave a negative response irt 15.
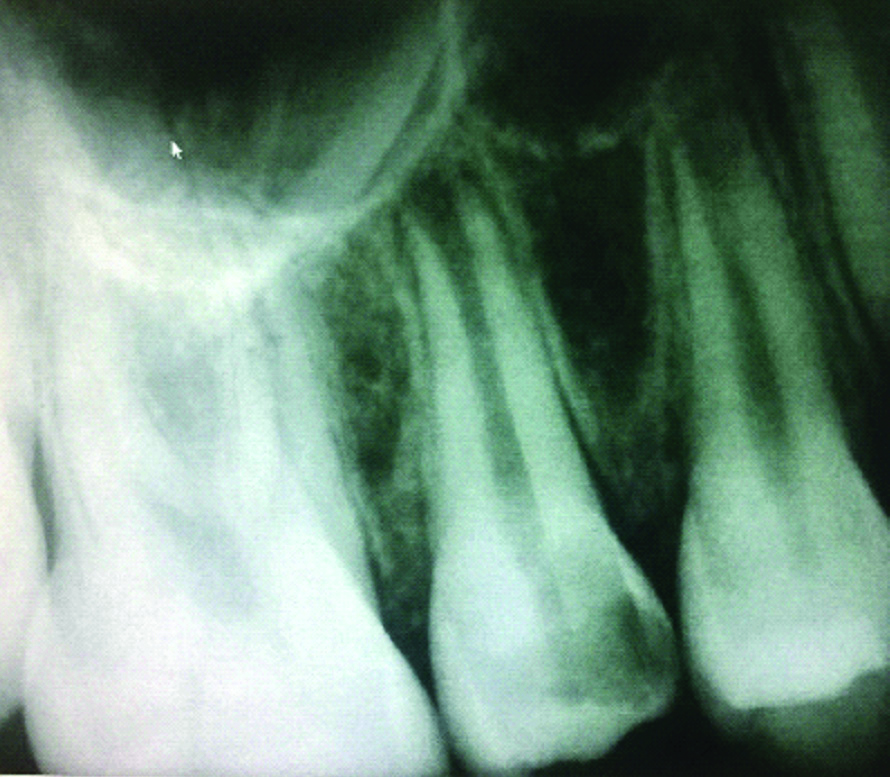
No soft tissue anomalies were seen during intraoral examination. Periodontal probing depths were found to be within the normal limits. Incomplete root formation with a wide-open apex was seen in intraoral periapical radiograph. The diagnosis of apical periodontitis with immature apex was made [Table/Fig-1].
Figure showing preoperative intraoral periapical radiograph.
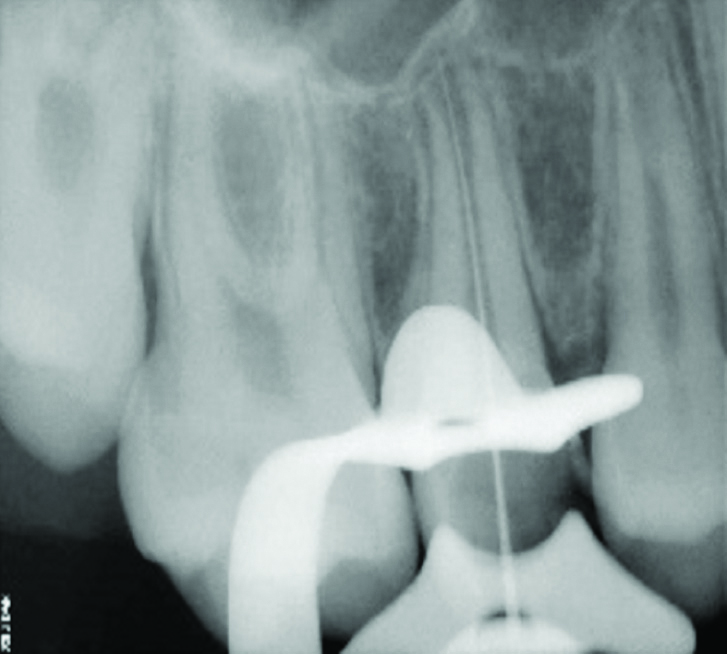
A conventional revascularization procedure was planned. LA was administered using 2% lidocaine with 1:100 000 epinephrine. The tooth was isolated using a rubber dam. Access cavity was modified using an Endo Access bur in a high-speed air turbine handpiece with copious irrigation. Temporary restoration was removed and working length of the tooth was determined by placing a size 15 K-file [Table/Fig-2]. It was noted that the remnants of radicular pulp were still present followed by bleeding in the canal. Gentle irrigation of the canal was performed using 10 mL of saline in order to preserve the viable pulp tissue which helps in development of open apex root. Further the canal was dried using sterile absorbent paper points. Triple antibiotic paste was formed by grounding and mixing an equal proportion of ciprofloxacin, metronidazole and minocycline. This mixture was mixed with distilled water to form the required paste. This antibiotic paste was then introduced with the blunt end of sterile paper points until the resistance was felt. The access cavity was then sealed with 4 mm of IRM.
Radiograph showing the working length irt 15.
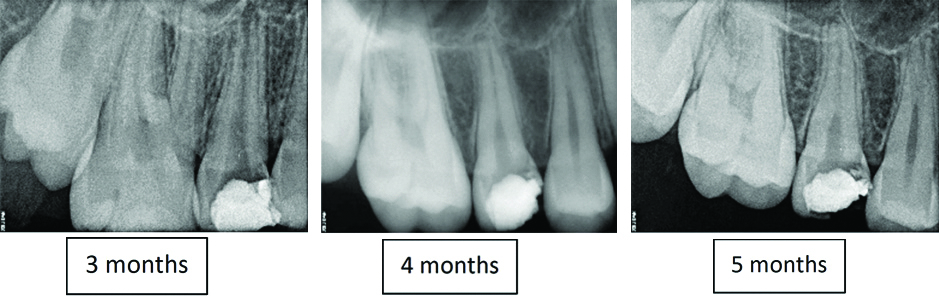
The patient was recalled after 3 weeks. The tooth was asymptomatic to percussion and palpation tests. Rubber dam isolation was obtained and LA was administered using 2% lidocaine with 1:100 000 epinephrine. The antibiotic paste was flushed out of the canals using sterile saline solution after re-opening the access cavity. The canal was dried with paper points followed by induction of bleeding using 15 no. k file and temporization with temporary restoration. Patient was recalled every two weeks for check-up but the patient did not respond. Patient visited after three months and it was found that there was narrowing of the apical area. After 5 months follow-up, it has been found that there was complete apical closure [Table/Fig-3]. Then 3-mm-thick layer of MTA (Mineral Trioxide Aggregate) was placed coronally. A moist cotton pellet was placed over the MTA, and tooth was temporised using IRM. The patient was recalled after 3 days to remove the cotton pellet, and the tooth was restored using IRM. The patient was called for follow-up visits at 1 month, 3 month, 4 month and 5 month, respectively. Radiographs taken during the follow-up visits revealed continuous thickening of dentinal walls, regression of periapical lesion followed by apical closure and root lengthening [Table/Fig-3,4].
Radiography showing the follow-up at 3 months, 4 months and 5 months respectively.
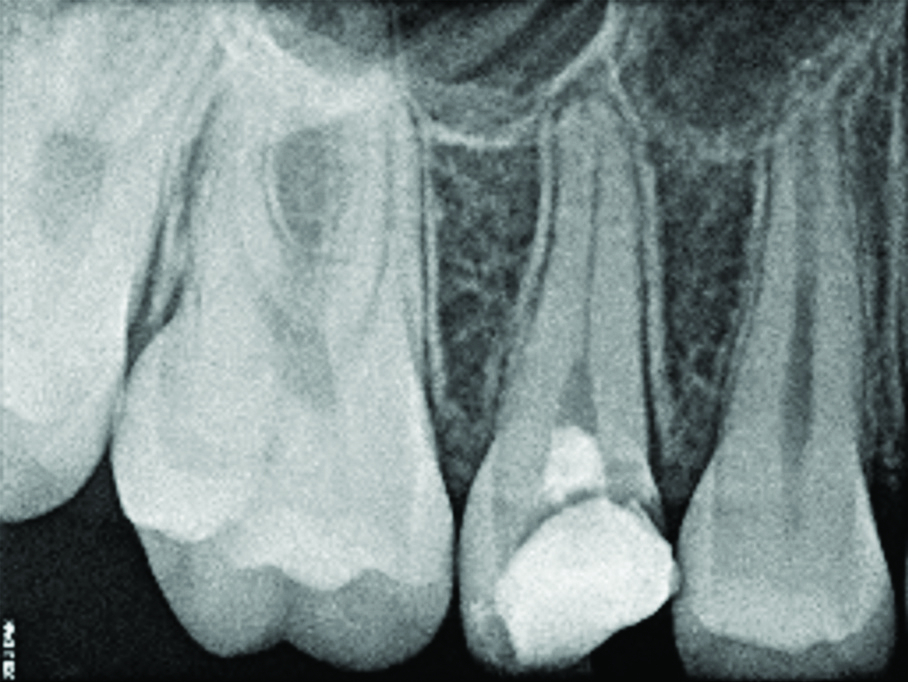
Radiograph showing MTA plug and restoration with IRM.
Discussion
Regenerative endodontics is a treatment revolution in dentistry in which a nonvital tooth is restored back to life through Root canal treatment [1]. Time taken by for the root completion post-eruption is 2-3 years, one of the crucial periods where any caries or injury to the tooth can cause cessation of development of the root. Traditional endodontic methods of treating necrotic immature permanent teeth are limited by the tooth’s incomplete root anatomy. Revascularization can broadly defined as the restoration of vascularity to a tissue or organ [2,3]. Revascularization technique makes the use of intracanal irrigants, chlorhexidine with placement of antibiotics which is a mixture of ciprofloxacin, metronidazole, and minocycline paste for several weeks. In a case report of Murugesan G et al., shows a promising effect of MTA and calcium hydroxide in regressing the periapical lesion and apical closure [4]. There is substantial evidence in case reports and case series in the current literature to support successful revascularization using antimicrobial therapy [5-7]. Therefore, the purpose of this report was to present a case on regeneration potential of the pulp.
The resulting closure of the root apex and thickening of the root walls demonstrated successful revascularization and maturogenesis after applying triple antibiotic therapy and MTA. Vitality testing would not be viable since the coronal plug does not allow access to the dentinal tubules where new pulp tissue has been regenerated below the CEJ level [1]. Necrosis of the Pulp in permanent teeth leads to delay in apical closure. Hence, revascularization helps in revitalising the tooth.
This technique makes the use of chlorhexidine with placement of antibiotics i.e., a mixture of ciprofloxacin, metronidazole, and minocycline paste for two weeks. This combination of medicines particularly Triple antibiotic therapy and MTA is cost effective, simple to use with least available equipments and effectively helps in disinfecting the root canal as well as to increase the revascularisation. The only disadvantage of this medicament is discoloration due to Minocycline. A number of previous researches have suggested replacing the medicament with Custom fitted Gutta-percha cones but since the apical portion of the root is wider than coronal portion proper closure at the apex becomes difficult. Further widening of the apical portion renders the tooth weak exposing to the risk of fracture [8-11]. Hence, revascularization is more conservative procedure in such cases rather than apexification.
In a review published in 2018 states that, instead of performing the routine treatment protocol and apexification, two types of antibiotics (metronidazole and ciprofloxacin) were applied to the canal which was left empty after the application. The initiation of apical closure 5 months after the antimicrobial procedure was observed in the radiographic finding. Thickening of the root dentine and complete apical closure, was confirmed 30 months after the treatment. Within 6 and 12 months, the success rate of TAP and Vitapex were 100% and 96%, respectively. In a study ornidazole was replaced with metronidazole in TAP, and better results were obtained at 3, 6, and 12 months after treatment of infected teeth. They added that ornidazole had better efficacy, longer duration of action and slower metabolism compared to metronidazole [12]. In a systemic review article it was observed that there was unanimity of the clinically satisfactory results in pulp revascularization procedures employing triple antibiotic paste as an intracanal medication. In most studies, all teeth were clinically asymptomatic in the different follow-up periods: after 1 month; after 12 months; and after 18 months. Studies have shown that the patients were asymptomatic, had no sensitivity to percussion and palpation, and had a complete resolution of swelling and the sinus [Table/Fig-5] [4,6,7,14,15].
Review of article with other medicaments [4,6,7,14,15].
| Studies | Medicaments used | Outcome |
|---|
| Murugesan G et al., [4] | MTA and Calcium Hydroxide | Apical closure within 3 months |
| Shin SY et al., [6] and Frank AL [7] | 6% NaOCl and 2% chlorhexidine coronal irrigation and using antimicrobial therapy | Restores root vitality, pulp regeneration and root maturation. |
| Shivashankar VY et al., [14] and Vijayaraghavan R et al., [15] | Triple Antibiotic paste | Revitalization of necrotic infected immature teeth within 1 year. |
| Present study | Triple Antibiotic paste | Complete apical closure was seen after 5 months of follow-up |
Conclusion(s)
Several technologies have been developed for delivering regeneration of pulp-dentin complex. Tooth with immature apex with viable radicular pulp should not be treated with aggressive procedures e.g., root canal treatment, so in such cases application of TAP followed by revascularization has to be done and to follow-up the case till the apex has been completely closed. So in these types of cases, apexification with calcium hydroxide and MTA can be avoided because Ca(OH)2 makes the radicular part brittle and may tend to fracture. Apexification with MTA has good results but inferior to the revascularization technique, as revascularization undergo Apexogenesis/Maturogenesis and can close the immature open apex.
Author Declaration:
Financial or Other Competing Interests: No
Was Ethics Committee Approval obtained for this study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Oct 24, 2019
Manual Googling: Dec 02, 2019
iThenticate Software: Dec 23, 2019 (15%)
[1]. Nygaard-Ostby B, The role of the blood clot in endodontic therapy: An experimental histologie studyActa Odontol Scand 1961 19:324-53.10.3109/00016356109043395 [Google Scholar] [CrossRef]
[2]. Huang GTJ, Gronthos S, Shi S, Mesenchymal stem cells derived from dental tissues vs those derived from other sources: their biology and role in regenerative medicineJ Dent Res 2009 9:792-806.10.1177/002203450934086719767575 [Google Scholar] [CrossRef] [PubMed]
[3]. Sigurdsson A, Trope M, Civian N, The role of endodontics after dental traumatic injuries. In: Hargreaves KM, Cohen SPathways of the Pulp 2011 10 edSt Louis, MoMosby Elsevier:620-49.10.1016/B978-0-323-06489-7.00017-5 [Google Scholar] [CrossRef]
[4]. Murugesan G, Selvaraj V, Veerabadhran M, Rangasamy V, Ramachandran K, Apexification with calcium hydroxide and mineral trioxide aggregate: Report of two casesJ Pharm Bioallied Sci 2013 5(Suppl 2):S131-34.10.4103/0975-7406.11430523956590 [Google Scholar] [CrossRef] [PubMed]
[5]. Thibodeau B, Case report: Pulp revascularization of a necrotic, infected, immature, permanent toothPediatr Dent 2009 31:145-48. [Google Scholar]
[6]. Shin SY, Albert JS, Mortman RE, One step pulp revascularization treatment of an immature permanent tooth with chronic apical abscess: A case reportInt Endod J 2009 42:1118-26.10.1111/j.1365-2591.2009.01633.x19912384 [Google Scholar] [CrossRef] [PubMed]
[7]. Frank AL, Therapy for the divergent pulpless tooth by continued apical formationJ Am Dent Assoc 1966 72:87-93.10.14219/jada.archive.1966.00175215726 [Google Scholar] [CrossRef] [PubMed]
[8]. Rule DC, Winter GB, Root growth and apical repair subsequent to pulpal necrosis in childrenBr Dent J 1966 120:586-90. [Google Scholar]
[9]. Sunitha Raja V, Munirathnam Naidu E, Platelet-rich fibrin: Evolution of a second-generation platelet concentrateIndian J Dent Res 2008 19:42-46.0.4103/0970-9290.3893118245923 [Google Scholar] [CrossRef] [PubMed]
[10]. Safi L, Ravanshad S, Continued root formation of pulp less permanent incisor following root canal treatment: A case reportInt Endod J 2005 38:489-93.10.1111/j.1365-2591.2005.00966.x15946271 [Google Scholar] [CrossRef] [PubMed]
[11]. Cvek M, Cleaton-Jones P, Austin J, Lownie J, Kling M, Fatti P, Effect of topical application of doxycycline on pulp revascularization and periodontal healing in reimplanted monkey incisorsEndod Dent Traumatol 1990 6:170-76.10.1111/j.1600-9657.1990.tb00413.x1723382 [Google Scholar] [CrossRef] [PubMed]
[12]. Mohammadi Z, Jafarzadehb H, Shalavi S, Yaripour S, Sharifi F, Kinoshita JI, A Review on triple antibiotic paste as a suitable material used in regenerative endodonticsIranian Endodontic Journal 2018 13(1):01-06.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5800433/ [Google Scholar]
[13]. Aline M, Marcela CE, Anamaria PP, Carolina CM, Maria CF, Lucas GA, A systematic review of pulp revascularization using a triple antibiotic pastePediatric Dentistry 2019 41(5)https://www.aapd.org/globalassets/media/publications/open-access/341-53.pdf [Google Scholar]
[14]. Shivashankar VY, Johns DA, Vidyanath S, Kumar MR, Platelet Rich Fibrin in the revitalization of tooth with necrotic pulp and open apexJ Conserv Dent 2012 15:395-98.10.4103/0972-0707.10192623112492 [Google Scholar] [CrossRef] [PubMed]
[15]. Vijayaraghavan R, Mathian VM, Sundaram AM, Karunakaran R, Vinodh S, (Triple antibiotic paste in root canal therapyJ. Pharm. Bioallied Sci 2012 4:S230-33.10.4103/0975-7406.10021423066258 [Google Scholar] [CrossRef] [PubMed]