Despite significant advances in endodontics, pain experienced after therapy is an undesired, yet often occurring sensation of important concern for both patients and endodontists [1].
Sources of post endodontic pain are multivarious-preoperative pain, procedural errors, extrusion of materials like-debris, intracanal medicaments, irrigants, obturating materials, irrigation techniques [2].
Sealer extrusion is common during obturation procedures which have been shown to have cytotoxic effects on periapical tissues elucidating an inflammatory response, activating sensory neurons, and thus increased postoperative discomfort and persistent pain [3].
The choice of sealer affects the prognosis of the treatment. However, to date there has been no documented in-vivo study that correlates the effect of these commonly used endodontic sealers- zinc-oxide eugenol based, calcium hydroxide based and epoxy-resin based on incidence of postoperative pain after root canal treatment. Therefore, this study aims to evaluate and compare the postoperative pain experienced after root canal treatment using three different root canal sealers, viz., Tubli-Seal EWT, Apexit Plus, and AH Plus.
Materials and Methods
This was a single center, single blind, parallel, in-vivo study which was carried out in the Department of Conservative Dentistry and Endodontics, KLE VK Institute of Dental Sciences, KLE Academy of Higher Education and Research, Belagavi, Karnataka, India, from February 2016 to July 2017. Ethical approval for the study was obtained from Research and Ethics Committee KLE VK Institute of Dental Sciences, Belagavi, Sl No: 1035.
Sample Size Determination
A pilot study was conducted in which the pain scores were recorded from three groups by 3 convenient samples in each group
Considering 5% α-error, 80% power of test and a drop-out rate of 10%, the required sample size was determined to be 33 patients in all the three groups totaling to 99 patients in the study.
Inclusion Criteria
Permanent molars diagnosed with chronic irreversible pulpitis in patients within the age group of 18-50 years who had a non-contributory medical history were included in the study.
Exclusion Criteria
Patients who refused to given consent for the procedure, those with any systemic diseases, pregnancy and immunocompromised conditions, history of maxillary sinusitis, allergic to lignocaine with 1:80,000 adrenaline and allergic to Non-Steroidal Anti-Inflammatory Drugs (NSAIDS) were excluded from the study.
Also, the patients who were already on analgesia within 24 hours before the treatment and those requiring root canal treatment of two or more teeth ipsilaterally (since the pain caused by any of these teeth can result in false positive reading) were excluded.
It was ensured that teeth with calcified canals, severe canal curvatures, immature apex, resorption (internal and external) and periodontal diseases were excluded.
Methodology
A total of 99 patients requiring endodontic treatment for permanent molar in accordance with the inclusion and exclusion criteria were selected for the study. The treatment and study design was explained to the patients in their own comprehendible language and a written informed consent was obtained from the voluntary patients who participated in the study [Table/Fig-1].
Flowchart of Methodology.
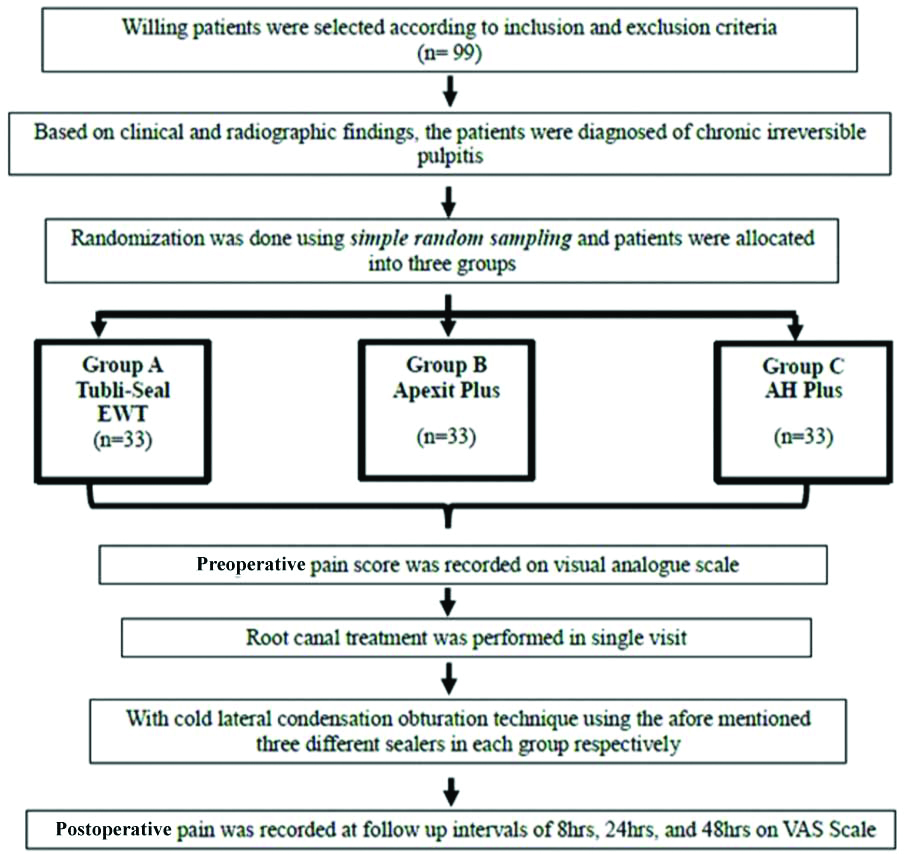
A cold test and electric pulp-test was used to assess pulp vitality. Based on clinical and radiographic findings, the patients were diagnosed of chronic irreversible pulpitis.
Allocation
The patients were allocated to three different groups as follows:
Group A-Tubli-Seal EWT (SybronEndo, Glendora, CA, USA) (n=33)
Group B-Apexit Plus (Ivoclar Vivadent, Schaan, Liechtenstein) (n=33)
Group C-AH Plus (Dentsply, DeTrey, Germany) (n=33)
Endodontic Protocol
A single clinician had evaluated all patients, using radiographic and clinical findings, and the same clinician was assigned for treatment of all cases. Before the start of treatment, the details of each patient with regard to tooth number, intensity of pain, gender, and age were recorded.
The severity of pain was measured using VAS. According to this scale, level of pain was documented in the range of 0-10 numerically and verbally as no pain (0), mild pain (1-3), moderate pain (4-6) and severe pain (7-10).
The patient received topical anaesthesia before local anaesthesia. Later local anaesthesia was administered (2% lignocaine with 1:80,000 adrenaline). Anaesthetic effect was verified by both subjective (tingling and numbness) and objective symptoms. It was also confirmed by lack of response to electric pulp sensibility and cold tests.
Later the tooth was isolated using rubber dam. Access cavity was prepared using sterile carbide burs under magnification. The canal patency was checked by #10 K-file (MANI, Inc. Japan) and a glide path was established using #15 K-file (MANI, Inc. Japan).
The working length was determined with K files and by the use of an apex locator (Dentaport ZX, J Morita corp). It was confirmed using periapical radiographs (Kodak).
All the canals were prepared using ProTaper Universal (Dentsply Maillefer) rotary files up to the working length to size dependent on apical gauging following manufacturer’s suggested sequence using endomotor (X-Smart Dentsply). Apical patency was maintained throughout the shaping procedure by recapitulating with #10 file between each instrument.
Irrigation Protocol
Endodontic syringe with closed-ended side-vented needle was used. All the canals were irrigated with 3% NaOCl (Vishal Dentocare Pvt., Ltd, India) and normal saline (Amanta, Kheda India). Finally the canals were flushed with 17% EDTA solution (Canalarge, Ammdent, India) for 1 min.
Obturation Protocol
All the canals were dried with sterile paper points (DiaDent Group Intl. Inc., Canada). According to each group, the specific sealer was applied into the dried canals using the master gutta-percha cone coating technique. All canals were obturated with gutta-percha cones (ProTaper, Dentsply Maillefer) using cold lateral condensation technique in the same visit. Later intermediate restorative material was given.
Postoperative and Follow-Up Instructions
The patients were advised to call the investigator by phone if they felt very uncomfortable at any point of the follow-up time and they were advised not to take medications without the knowledge of the investigator
The patients were instructed to take mild analgesics (200 mg of Ibuprofen), only if they experienced intolerable pain
The absence of pain, or the appropriate degree of its presence was recorded as none, mild, moderate, or severe, by using a VAS.
The Pain Score Reading
No pain (0): The treated tooth felt normal. Patients don’t have any pain
Mild pain (1-3): Recognisable, but not discomforting pain, which required no analgesics
Moderate pain (4-6): Discomforting, but bearable, pain (analgesics, if used, were effective in relieving the pain)
Severe pain (7-10): Difficult to bear (analgesics had little or no effect in relieving the pain)
The patient was contacted through phone call after treatment to note their pain readings at postoperative periods of 8, 24, and 48 hours. The amount of analgesic (if taken) was recorded at that particular time interval.
Statistical Analysis
It was performed using SPSS software (version 20.0). The intergroup comparisons were done using Kruskal Wallis ANOVA, Mann-Whitney U test, and intragroup comparisons were done using Wilcoxon matched pairs test. Chi-square test was used for comparing demographic data of the participants. The level of statistical significance considered was p<0.05.
Results
The preoperative pain scores of all patients in all three groups, fell in the range of mild (VAS score 1-3) and moderate (VAS score 4-6) categories.
Comparison of Three Study Groups (A, B, C) with Respect to VAS Scores at Preoperative, 8 hours, 24 hours, 48 hours by Kruskal-Wallis ANOVA
In all three groups, the pain scores postoperatively when compared to preoperative score, were statistically significant at the end of 8 hrs (p=0.0030) and 48 hrs (p=0.0320). However, the scores at end of 24 hours when compared to those at preoperative though not statistically significant (p=0.1550) were clinically significant [Table/Fig-2].
Comparison of three study groups (A, B, C) with respect to VAS scores at preoperative, 8 hours, 24 hours, 48 hours by Kruskal Wallis ANOVA.
| Time points | Pain score | Group A | Group B | Group C | H-value | p-value |
|---|
| Pre-op | Mean | 4.7 | 4.4 | 4.3 | 4.2870 | 0.1170 |
| SD | 0.8 | 0.9 | 0.7 |
| Median | 5.0 | 4.0 | 4.0 |
| Mean rank | 57.7 | 47.4 | 44.9 |
| After 8 hrs | Mean | 3.0 | 2.8 | 3.1 | 2.0610 | 0.3570 |
| SD | 0.9 | 0.9 | 0.7 |
| Median | 3.0 | 3.0 | 3.0 |
| Mean rank | 50.7 | 44.9 | 54.4 |
| After 24 hrs | Mean | 1.7 | 1.5 | 1.6 | 1.8710 | 0.3920 |
| SD | 0.7 | 0.8 | 0.7 |
| Median | 2.0 | 1.0 | 2.0 |
| Mean rank | 54.6 | 45.8 | 49.6 |
| After 48 hrs | Mean | 0.5 | 0.5 | 0.6 | 2.1190 | 0.3470 |
| SD | 0.6 | 0.5 | 0.5 |
| Median | 1.0 | 0.0 | 1.0 |
| Mean rank | 49.6 | 45.8 | 54.7 |
| Compare pre-op to 8 hrs | Mean | 1.7 | 1.6 | 1.2 | 11.5180 | 0.0030* |
| SD | 0.9 | 0.5 | 0.8 |
| Median | 2.0 | 2.0 | 1.0 |
| Mean rank | 59.1 | 52.6 | 38.3 |
| Compare pre-op to 24 hrs | Mean | 3.0 | 2.9 | 2.7 | 3.7230 | 0.1550 |
| SD | 0.8 | 0.6 | 0.6 |
| Median | 3.0 | 3.0 | 3.0 |
| Mean rank | 55.4 | 50.8 | 43.8 |
| Compare pre-op to 48 hrs | Mean | 4.2 | 3.9 | 3.7 | 6.8610 | 0.0320* |
| SD | 0.7 | 0.9 | 0.8 |
| Median | 4.0 | 4.0 | 4.0 |
| Mean rank | 58.1 | 50.7 | 41.3 |
*p<0.05
Pair Wise Comparison of Three Study Groups (A,B,C) with Respect to VAS Scores at Preoperative, 8 hours, 24 hours, 48 hours by Mann-Whitney U test
When compared to the scores at pre-operative, there was a statistically significant difference at the end of 8 hours between group A and C (p=0.0043), and between group B and C (p=0.0372) [Table/Fig-3].
Pair wise comparison of three study groups (A, B, C) with respect to VAS scores at preoperative, 8 hours, 24 hours, 48 hours by Mann-Whitney U test.
| Time points | Groups | Mean | SD | Median | Mean rank | U-value | Z-value | p-value |
|---|
| Pre-op | Group A | 4.7 | 0.8 | 5.0 | 36.82 | 435.00 | -1.4043 | 0.1602 |
| Group B | 4.4 | 0.9 | 4.0 | 30.18 |
| Group A | 4.7 | 0.8 | 5.0 | 37.92 | 398.50 | -1.8724 | 0.0612 |
| Group C | 4.3 | 0.7 | 4.0 | 29.08 |
| Group B | 4.4 | 0.9 | 4.0 | 34.23 | 520.50 | -0.3078 | 0.7582 |
| Group C | 4.3 | 0.7 | 4.0 | 32.77 |
| After 8 hrs | Group A | 3.0 | 0.9 | 3.0 | 35.39 | 482.00 | -0.8015 | 0.4228 |
| Group B | 2.8 | 0.9 | 3.0 | 31.61 |
| Group A | 3.0 | 0.9 | 3.0 | 32.32 | 505.50 | -0.5002 | 0.6170 |
| Group C | 3.1 | 0.7 | 3.0 | 34.68 |
| Group B | 2.8 | 0.9 | 3.0 | 30.33 | 440.00 | -1.3402 | 0.1802 |
| Group C | 3.1 | 0.7 | 3.0 | 36.67 |
| After 24 hrs | Group A | 1.7 | 0.7 | 2.0 | 36.39 | 449.00 | -1.2247 | 0.2207 |
| Group B | 1.5 | 0.8 | 1.0 | 30.61 |
| Group A | 1.7 | 0.7 | 2.0 | 35.18 | 489.00 | -0.7118 | 0.4766 |
| Group C | 1.6 | 0.7 | 2.0 | 31.82 |
| Group B | 1.5 | 0.8 | 1.0 | 32.18 | 501.00 | -0.5579 | 0.5769 |
| Group C | 1.6 | 0.7 | 2.0 | 34.82 |
| After 48 hrs | Group A | 0.5 | 0.6 | 1.0 | 34.73 | 504.00 | -0.5194 | 0.6035 |
| Group B | 0.5 | 0.5 | 0.0 | 32.27 |
| Group A | 0.5 | 0.6 | 1.0 | 31.82 | 489.00 | -0.7118 | 0.4766 |
| Group C | 0.6 | 0.5 | 1.0 | 35.18 |
| Group B | 0.5 | 0.5 | 0.0 | 30.50 | 445.50 | -1.2696 | 0.2042 |
| Group C | 0.6 | 0.5 | 1.0 | 36.50 |
| Compare pre-op to 8 hrs | Group A | 1.7 | 0.9 | 2.0 | 35.86 | 466.50 | -1.0003 | 0.3172 |
| Group B | 1.6 | 0.5 | 2.0 | 31.14 |
| Group A | 1.7 | 0.9 | 2.0 | 40.24 | 322.00 | -2.8534 | 0.0043* |
| Group C | 1.2 | 0.8 | 1.0 | 26.76 |
| Group B | 1.6 | 0.5 | 2.0 | 38.42 | 382.00 | -2.0840 | 0.0372* |
| Group C | 1.2 | 0.8 | 1.0 | 28.58 |
| Compare pre-op to 24 hrs | Group A | 3.0 | 0.8 | 3.0 | 35.09 | 492.00 | -0.6733 | 0.5008 |
| Group B | 2.9 | 0.6 | 3.0 | 31.91 |
| Group A | 3.0 | 0.8 | 3.0 | 37.35 | 417.50 | -1.6287 | 0.1034 |
| Group C | 2.7 | 0.6 | 3.0 | 29.65 |
| Group B | 2.9 | 0.6 | 3.0 | 35.88 | 466.00 | -1.0067 | 0.3141 |
| Group C | 2.7 | 0.6 | 3.0 | 31.12 |
| Compare pre-op to 48 hrs | Group A | 4.2 | 0.7 | 4.0 | 35.85 | 467.00 | -0.9939 | 0.3203 |
| Group B | 3.9 | 0.9 | 4.0 | 31.15 |
| Group A | 4.2 | 0.7 | 4.0 | 39.20 | 356.50 | -2.4110 | 0.0159* |
| Group C | 3.7 | 0.8 | 4.0 | 27.80 |
| Group B | 3.9 | 0.9 | 4.0 | 36.53 | 444.50 | -1.2824 | 0.1997 |
| Group C | 3.7 | 0.8 | 4.0 | 30.47 |
*p<0.05
Also, there was a statistically significant difference at the end of 48 hours between group A and C (p=0.0159) with lower scores in Group C than the other two groups [Table/Fig-3].
Intragroup Comparison of Preoperative, 8 hours, 24 hours, 48 hours with Respect to VAS Scores in Three Study Groups (A, B, C) by Wilcoxon Matched Pairs Test
When the scores at the three time periods were compared among each other, within each group, there was a statistically significant difference in all three groups A, B, C (p=0.0001) [Table/Fig-4].
Comparison of pre-op, 8 hours, 24 hours, 48 hours with respect to VAS scores in three study groups (A, B, C) by Wilcoxon matched pairs test.
| Groups | Time points | Mean | SD | Mean diff. | SD diff. | % of change | Z-value | p-value |
|---|
| Group A | Pre-op | 4.7 | 0.8 | | | | | |
| After 8 hrs | 4.4 | 0.9 | 1.70 | 0.99 | 36.22 | 4.1443 | 0.0001* |
| Pre-op | 4.7 | 0.8 | | | | | |
| After 24 hrs | 4.3 | 0.7 | 2.96 | 0.90 | 62.99 | 4.4573 | 0.0001* |
| Pre-op | 4.4 | 0.9 | | | | | |
| After 48 hrs | 4.3 | 0.7 | 4.19 | 0.74 | 88.98 | 4.5407 | 0.0001* |
| Group B | Pre-op | 4.36 | 0.93 | | | | | |
| After 8 hrs | 2.79 | 0.93 | 1.58 | 0.50 | 36.11 | 5.0119 | 0.0001* |
| Pre-op | 4.36 | 0.93 | | | | | |
| After 24 hrs | 1.48 | 0.76 | 2.88 | 0.65 | 65.97 | 5.0219 | 0.0001* |
| Pre-op | 4.36 | 0.93 | | | | | |
| After 48 hrs | 0.45 | 0.51 | 3.91 | 0.95 | 89.58 | 5.0319 | 0.0001* |
| Group C | Pre-op | 4.36 | 0.93 | | | | | |
| After 8 hrs | 2.79 | 0.93 | 1.58 | 0.50 | 36.11 | 4.4316 | 0.0001* |
| Pre-op | 4.36 | 0.93 | | | | | |
| After 24 hrs | 1.48 | 0.76 | 2.88 | 0.65 | 65.97 | 5.0119 | 0.0001* |
| Pre-op | 4.36 | 0.93 | | | | | |
| After 48 hrs | 0.45 | 0.51 | 3.91 | 0.95 | 89.58 | 5.0319 | 0.0001* |
*p<0.05
Age Distribution among Groups
The mean age in group A was 31.24±11.08 years, in group B was 29.18±9.49 years, while in group C was 31.67±6.36 years [Table/Fig-5].
Distribution of patients in three study groups by age groups (A, B, C).
| Age groups | Group A | % | Group B | % | Group C | % | Total | % |
|---|
| ≤20 yrs | 6 | 18.18 | 8 | 24.24 | 2 | 6.06 | 16 | 16.16 |
| 21-30 yrs | 10 | 30.30 | 10 | 30.30 | 7 | 21.21 | 27 | 27.27 |
| 31-40 ys | 9 | 27.27 | 9 | 27.27 | 21 | 63.64 | 39 | 39.39 |
| ≥41 yrs | 8 | 24.24 | 6 | 18.18 | 3 | 9.09 | 17 | 17.17 |
| Chi-square=13.7876 p=0.0321* |
| Total | 33 | 100.00 | 33 | 100.00 | 33 | 100.00 | 99 | 100.00 |
| Mean age | 31.24 | 29.18 | 31.67 | 30.70 |
| SD age | 11.08 | 9.49 | 6.36 | 9.16 |
*p<0.05
Gender Distribution among Groups
In group A, 48.48% of the samples were males while 51.52% of the samples were females; group B, 48.48% males and 51.52% females; group C, 39.39% males and 60.61% females [Table/Fig-6].
Distribution of male and female patients in three study groups (A, B, C).
| Sex | Group A | % | Group B | % | Group C | % | Total | % |
|---|
| Male | 16 | 48.48 | 16 | 48.48 | 13 | 39.39 | 45 | 45.45 |
| Female | 17 | 51.52 | 17 | 51.52 | 20 | 60.61 | 54 | 54.55 |
| Total | 33 | 100.00 | 33 | 100.00 | 33 | 100.00 | 99 | 100.00 |
| Chi-square=0.7332 p=0.6931 |
Discussion
In literature, reported frequencies of post-endodontic pain range from 1.5 to 53% [4,5]. The success and failure of endodontic treatment is determined by long-term results and not the presence or absence of short-term postoperative pain [4]. Yet postoperative pain is an important issue for both dentists and patients when considering patient’s confidence in their dentists, and their attitude towards future dental treatment.
The evolution of sealers has been from the conventional ZOE based preparations which have a history of use in root canal obturation for over a century which are highly acclaimed for their antimicrobial property [6]. These were followed by Calcium hydroxide based sealers that had an additional osteogenic-cementogenic potential. The rationale for the addition of calcium hydroxide to root canal sealers was their antibacterial and tissue regenerating ability, exerted via the leaching of calcium and hydroxyl ions to surrounding tissues [6]. Then came the era of contemporary ones, the resin based sealers like epoxy-resin based sealers having properties of adhesion. [6]. So this study, evaluated and compared the effect of these three commonly used class of endodontic sealers: zinc-oxide eugenol based, calcium hydroxide based and epoxy-resin based on incidence of postoperative pain after root canal treatment.
Abdel Wahab MHA and Kennedy JG, reported, the high sensitivity and specificity of cold and electric pulp tests to localise pulpal pain [7]. Therefore, in this study the findings of these tests were correlated with radiographic and clinical findings to diagnose irreversible pulpitis.
In most of similar clinical studies, usually single-rooted teeth were selected for evaluating postoperative pain which was done to minimise the risk of iatrogenic errors due to missed canals or complicated root canal anatomy with multirooted teeth [8].
However, on the other hand, in day-to-day clinical scenario, it is more likely that the molar teeth are the most common reason for a patient to visit a dental office rather than the single rooted teeth. Thus, justifying the selection of multirooted molar teeth in this study.
In order to avoid afore-mentioned complications, greater care was taken not to miss any canals with the aid of magnification and meticulous aseptic protocol was followed to avoid the risk of residual microorganism exacerbation or to introduce the bacteria into the periradicular tissues.
Patients requiring root canal treatment of two or more teeth ipsilaterally were avoided as the pain caused by any of these teeth could have led to exaggerated response from patient and interfere with interpretation from the pain scale.
Patients with apical periodontitis, periapical pathology, sinus tract stomas and retreatment cases, were excluded from the study as it has been proved that microbial cause is the important causative factor of pain and periapical pain may become a confounding factor in the study [9].
Root canal therapy in a single visit has many favourable aspects like no risk of inter-appointment leaky temporary restorations, lesser number of operative procedures, thereby shortened chair-side time making it more economically viable both for patient and the dentist [10]. Also, several reports suggest that single visit therapy ensues less postoperative discomfort than multi-visit therapy which justifies the same in this study [11].
An aseptic endodontic protocol was followed where both radiologic and electronic root canal measurements of working length were combined which greatly helps to confine instrumentation within the root canal system, thereby preventing the over-instrumentation, being one of the reasons for postoperative discomfort [12].
The ProTaper Universal system which is one of the most commonly preferred rotary NiTi systems by dental practitioners had been used in this study [13]. Its modified triangular cross section with three-point contact between this progressively tapering file and canal has shown encouraging results in crown-down technique over the years in terms of its shaping ability [14].
It has been well documented that the use of closed-ended and side-vented needles prevented the apical extrusion and possible periradicular discomfort by irrigants [15]. Thus, it justifies their use in the present study, with the standard irrigation protocol including 3% sodium hypochlorite, 17% EDTA solution and sterile normal saline (0.9% w/v). The sealer application by master cone coating and pumping technique has shown to better seal the voids between the obturating material and dentinal walls [16]. Obturation with cold lateral condensation was completed in the same appointment as it has been affirmed by researcher Schwendicke F and Göstemeyer G, that the root canal is most clean with least microbial load immediately after chemo-mechanical preparation [10].
It is well known that pain perception is a highly subjective and variable experience as its measurement is very difficult due to high probability of errors mediated by various physical and psychological factors. The use of VAS to evaluate the intensity of pain is well documented for its validity and reliability [17]. Hence in this study, a 10 cm VAS scale ranging from 0 to 10 was used to measure the postoperative pain intensity, which was explained, and familiarised to all patients.
It is important for a clinician to evaluate the benefits and risk of prescribing analgesics after root canal treatment.
In this study, among the NSAIDS, the prototype medication for postoperative pain relief after root canal treatment, Ibuprofen 200 mg a safe and cost-effective analgesic was prescribed as over the counter drug to patients only if they developed pain during the follow-up period [18]. This was done to avoid the intake of analgesics immediately after the treatment due to psychological fear of pain, which in turn may affect the pain intensity due to treatment protocol.
All the pain intensity scores and number of pills taken at each follow-up period were recorded through phone calls instead of questionnaires to improve patient cooperation, marking the pain intensity at proper follow-up time, and to avoid the possible loss of follow-up from the study.
In general, all the patients in this investigation had preoperative pain of mild to moderate nature as defined by the VAS scores. Studies show that incidence of postoperative pain associated with symptomatic teeth was comparatively more than the asymptomatic teeth [19]. Therefore, preoperative pain is considered one of the predictable indicators for postoperative pain as in this study.
Within each group, when the scores at the three time periods were compared among each other there was a statistically significant difference in all three groups A, B, C (p=0.0001) [Table/Fig-4].
However, in an intergroup comparison, at specific time points (8 hrs, 24 hrs and 48 hrs) the mean value of pain scores among three groups were not statistically significant [Table/Fig-2]. This indicates that the pace of pain reduction among all three sealers may be similar.
But, when the mean pain score at specific time point was compared with that of the pre-op score: in all groups, there was a statistically significant difference at the end of 8 hours (p=0.0030) and the end of 48 hrs (p=0.0320) when compared to the scores at pre-op [Table/Fig-2].
This decrease in pain by increasing time is both logical and expected because this is a natural course of disease process after debridement. None of the patients reported increase in pain intensity when compared with their respective baseline pain intensity (except two patients, which may be attributed to the subjective component of pain).
These results are in agreement with previous studies by Scelza MZ et al., and Ehsani M et al., who asserted that the irritant effect induced by sealers gradually reduced with passage of time [20,21].
At the end of 8 hours, the mean pain scores in group A (Tubli-Seal EWT), group B (Apexit Plus) and group C (AH Plus) were 1.7, 1.6 and 1.2 respectively which indicated a statistically significant difference in the reduction of pain between group A and C (p=0.0043), and between group B and C (p=0.0372) [Table/Fig-3]. Also at the end of 48 hours, the mean pain scores in group A and C were 4.2 and 3.7, respectively which had a statistically significant difference (p=0.0159) [Table/Fig-3].
The reason for this relatively higher mean pain score in group A (Tubli-Seal EWT) and lower pain score in group C (AH Plus) can be attributed to the fact that the eugenol based sealers have a relatively higher cytotoxicity than the resin counter parts [22].
These findings are also in agreement with those of Tanomaru FM et al., who asserted that inflammatory infiltrate present in the periapical tissues due to irritation potential of the root canal filling material was predominantly of higher severity (92.9%) in Zinc oxide eugenol based sealer group than Calcium hydroxide based sealer group (57.9%) and AH Plus was shown to have better biocompatibility than other sealers [23].
The reasons may also be due to the high solubility of eugenol based sealer and higher chance of apical extrusion (though not radiographically apparent in this study) than the resin ones [24]. In addition, these assertions may also be the reason for consumption of analgesic by one patient in group A and two patients in group C after 8 hours of treatment.
The distribution of age in all the groups was uniform except in Group C where 21 patients out of 33 (63.64%) fell in the age range between 31-40 years thus giving a statistically significant finding, p=0.03. This could be attributed to the random allocation of patients. It is not clinically significant as there are no reports of evidence documented on influence of age on pain perception. There are many studies, which inferred that females are more sensitive to pain perception compared to males [25,26] whereas no such finding was noted in this study.
Limitation(s)
The present study compared only three types of sealers, the biological effect of various other available class of root canal sealers like Methacrylate resin-based, Glass-ionomer based, Bioceramic-based sealers etc., on postoperative pain was not evaluated. This could possibly be a limitation of this study. Also, the present study had a short follow-up time. Further studies are needed to compare postoperative pain after root canal treatment with a longer follow-up time.
Conclusion(s)
The present study shows that in permanent molars with irreversible pulpitis when treated with different sealers, the pain after endodontic treatment gradually reduced with passage of time. Nonetheless, when AH plus was used as root canal sealer, the pain post-therapy, was relatively lesser compared to pre-treatment status. Thus, inferring that the choice of root canal sealer used has an influence of post-treatment discomfort.