Restoring patients smile with congenitally missing maxillary lateral incisor often needs a challenging interdisciplinary treatment, which can be done either by canine substitution, single implants, or tooth-supported restorations. This case report describes the orthodontic treatment of an Angle Class I malocclusion, slightly convex lower third profile, absence of right maxillary lateral incisor, microdontia of the left lateral incisor, and prolonged retention of the right deciduous canine. The treatment was completed with good dental and functional occlusion with a third premolar implant-borne crown. After one-year of follow-up there was maintenance of good aesthetics, with gingival and periodontal health with stability.
Case Report
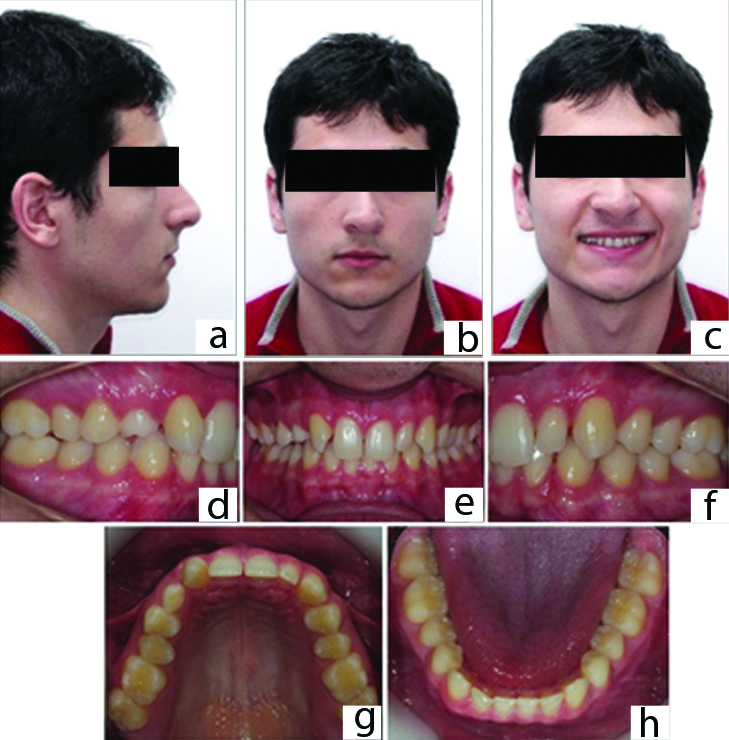
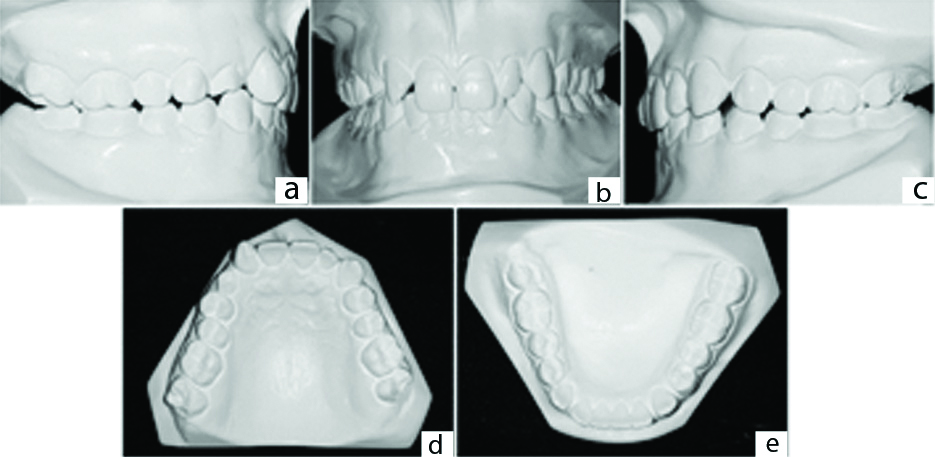
A 19.5-year-old boy reported for the orthodontic consultation in a private practice office with a primary complaint of “irregularly shaped tooth,” pointing towards the maxillary right canine in place of the lateral incisor. His medical and dental history were non-contributory. Intraorally, he presented an Angle Class I malocclusion, small size of the left lateral incisor [Table/Fig-1a-h]. Extraoral examination showed a slightly convex lower third profile. On the analysis of dental casts, the maxillary and mandibular arch showed a mild misalignment and spacing on the mesial and the distal sides of the maxillary left lateral incisor, Angle Class I molar relationship, 6,0 mm overbite, and normal overjet [Table/Fig-2a-e].
Pretreatment facial and intraoral photographs: a) right side profile view; b) frontal view; c) frontal smile view; d) right lateral intraoral image; e) frontal image f) left lateral intraoral image g) maxillary occlusal view; h) Mandibular occlusal view. Diastema on the mesial and the distal sides of the maxillary left lateral incisor, 6,0 mm overbite, and normal overjet.
Pretreatment dental casts: a) right lateral intraoral image; b) frontal image c) left lateral intraoral image; d) maxillary occlusal view showed a mild misalignment and leveling; e) Mandibular occlusal.
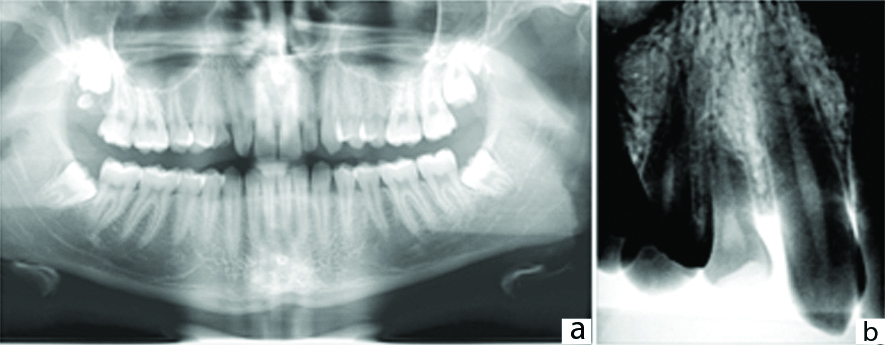
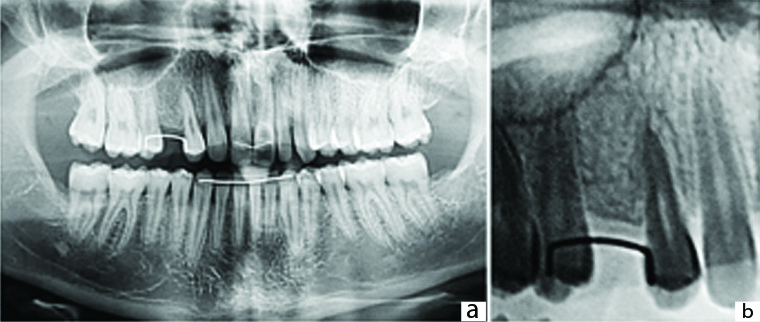
Panoramic and periapical radiographs revealed the absence of a maxillary right lateral incisor and retained maxillary right deciduous canine [Table/Fig-3a-b].
Pretreatment radiographs: a) Panoramic radiograph showing the presence of deciduous maxillary right canine; b) periapical radiograph showing the absence of a maxillary right lateral incisor and retained maxillary right deciduous canine.
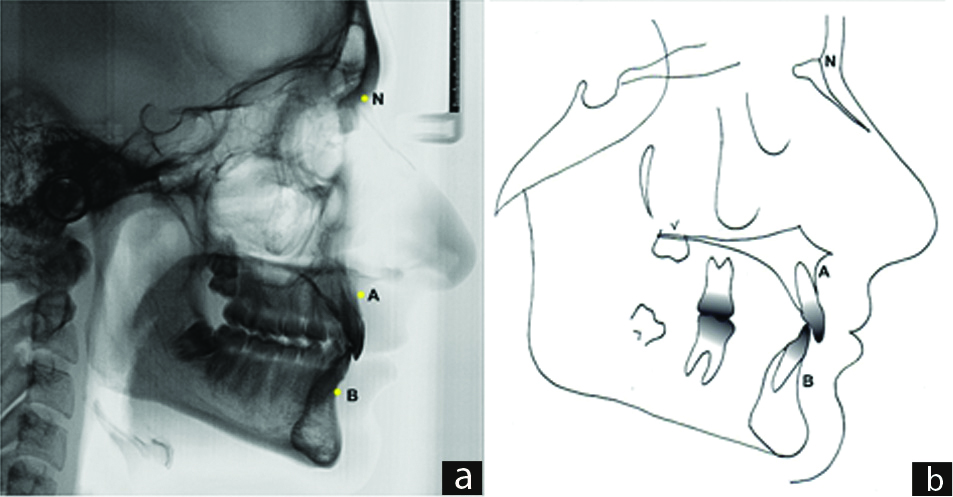
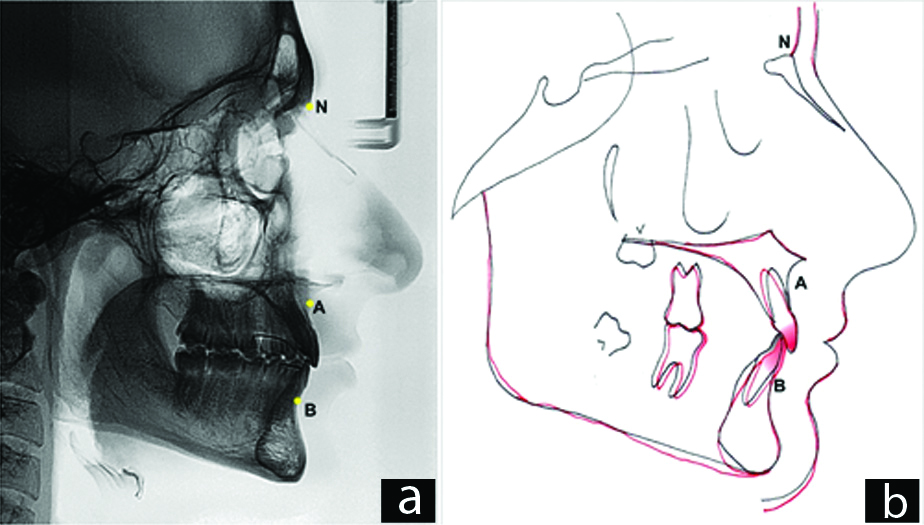
The cephalometric analysis showed a skeletal Class I pattern (ANB=3°), maxillary incisor in a good position (1-NA=23°), mandibular incisor slightly upright (1-NB=22°), soft tissue measurement showed a slightly convex profile (Z-Angle=78°) [Table/Fig-4a-b].
Pretreatment cephalometric radiograph and tracing.
Treatment Objectives
The orthodontic treatment aimed to maintain the good facial profile, align, level, and restore the missing maxillary right lateral incisor.
Treatment Alternatives
Extracting the maxillary right deciduous canine and all three treatment alternatives were explained to the patient. First: to open space between maxillary central incisor and canine for a prosthetic replacement mostly with an implant-borne crown; second: to close the space completely by moving the posterior teeth with the canine substitution in place of missing lateral incisor; third: to open space between the maxillary first and second right premolars.
Treatment Progress
Before orthodontic treatment, the patient was referred to the general practitioner for routine clinical procedures. All treatment alternatives were explained, and the patient decided for opening the space between the maxillary first and second right premolars, to position the prosthesis far from the aesthetic zone.
The associated risks, the need for cooperation in the hygiene and in the use of accessories such as the intermaxillary elastics and the time of treatment were oriented, informed, and explained.
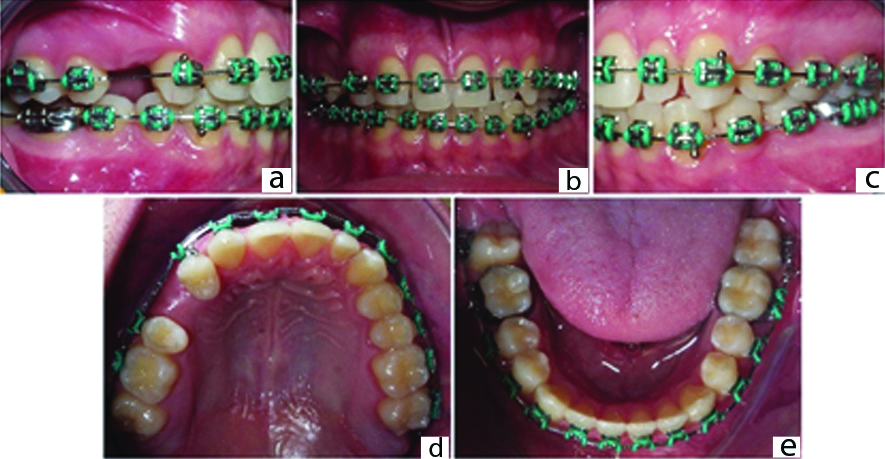
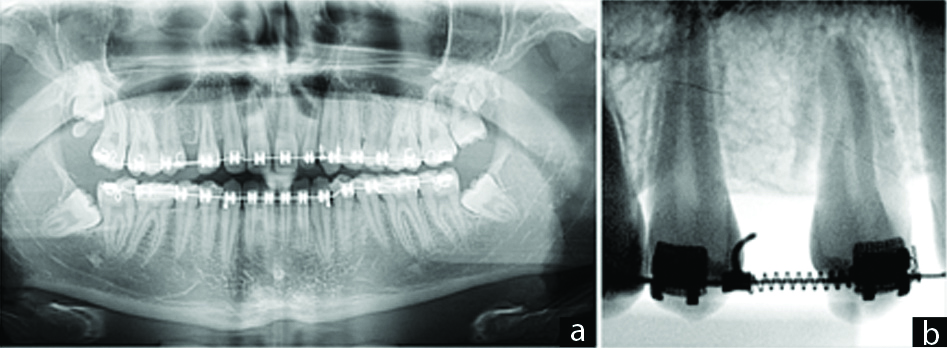
A 0.022″×0.28″ edgewise standard brackets were bonded in all teeth, except in the mandibular first molars, which were banded. The 0.016″×0.016″ NiTi Thermal was the first archwire for alignment and leveling, followed by 0.016″×0.022″ NiTi Thermal; 0.017″×0.025″ SS; and finishing with a 0.019″×0.25″ SS. Coil spring and elastic chain were used to open space between both maxillary right premolars [Table/Fig-5a-e,6a-b].
Progress. Space opening between both right maxillary premolars: a) right lateral intraoral image; b) frontal image; c) left lateral intraoral image; d) maxillary occlusal view; e) Mandibular occlusal.
Progress. Panoramic and periapical radiographs.
Treatment Results
After 30 months the desired results were achieved, and the appliance was removed. The treatment time was longer than expected because the patient had to stop regular consultation for eight months for family reasons. A maxillary wrap around removable retainer was placed with bonded braided dead-wire between maxillary central incisors, and a mandibular lingual 0.028-in round stainless-steel wire retainer was bonded from canine to canine [Table/Fig-7].
Post treatment facial and intraoral photographs: a) right profile view; b) frontal view; c) frontal smile view; d) right lateral intraoral image; e) frontal image; f) left lateral intraoral image; g) maxillary occlusal view with space opened between the right maxillary premolars for placement of the implant; h) Mandibular occlusal.
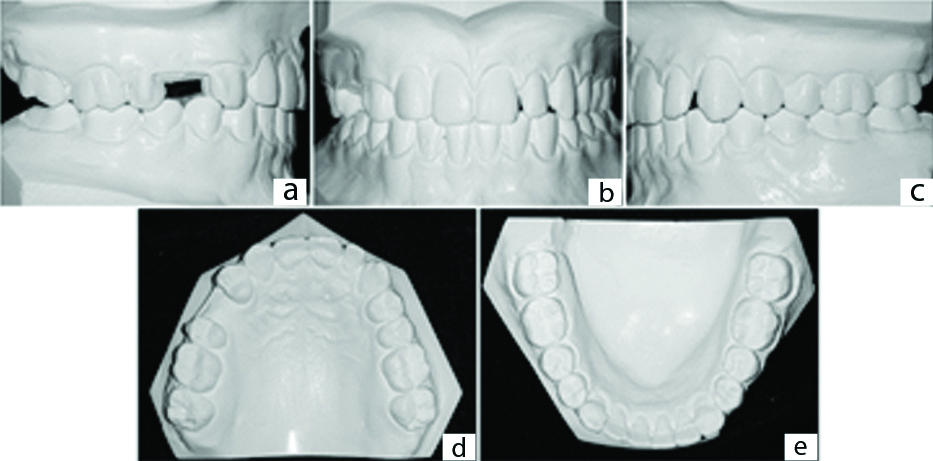
Post treatment intraoral records show that a space was opened between the right maxillary premolars for placement of the implant. The distal angulation and the space were maintained mesial and distal to the maxillary left lateral incisor for build-up [Table/Fig-8a-e]. Good intercuspation with Class I molars and canines with aesthetics, function, and gingival and periodontal health was obtained [Table/Fig-7a-h].
Post treatment plaster casts. a) right lateral intraoral image; b) frontal image; c) left lateral intraoral image; d) maxillary occlusal view; e) Mandibular occlusal.
Post treatment panoramic and periapical radiographs. a) Panoramic radiograph; b) periapical radiograph.
The radiographic evaluation shows good root parallelism between both maxillary right premolars, but when the first premolar analysed individually, was slightly distally tilted. Also, it was ensured that adequate bone was available for placing the implant. The maintenance of radicular and alveolar health was observed during treatment [Table/Fig 9a-b]. The total cephalometric superimposition showed that the maxillary and mandibular incisors were well positioned and the facial profile was also well maintained [Table/Fig-10a,b;11].
a) Post treatment cephalometric radiograph; b) superimposition of the cephalometric tracings. Prettreatment, black; Posttreatment, red.
Cephalometric measurements.
| Measurements | Norm | Pre treatment | Post treatment |
|---|
| SNA angle (°) | ° | 79 | 80 |
| SNB angle (°) | 80° | 76 | 77 |
| ANB angle (°) | 2° | 3 | 3 |
| Ao-Bo (mm) | ♀0±2 mm ♂1±2 mm | 0 | -2 |
| Facial angle (°) | 87° | 88 | 89 |
| Convexity (°) | 0° | 3 | -3 |
| FMA(°) | 25° | 19 | 19 |
| GoGn-SN) (°) | 32° | 28 | 27 |
| Y-Axis (°) | 59° | 56 | 61 |
| 1-NA (mm) | 4 mm | 4 | 4 |
| 1-NA (°) | 22° | 23 | 15 |
| 1-NB (mm) | 4 mm | 4 | 4 |
| 1-NB (°) | 25° | 22 | 23 |
| IMPA (°) | 90° | 99 | 100 |
| Interincisal angle (°) | 132° | 138 | 141 |
| Z-angle (°) | 75° | 78 | 77 |
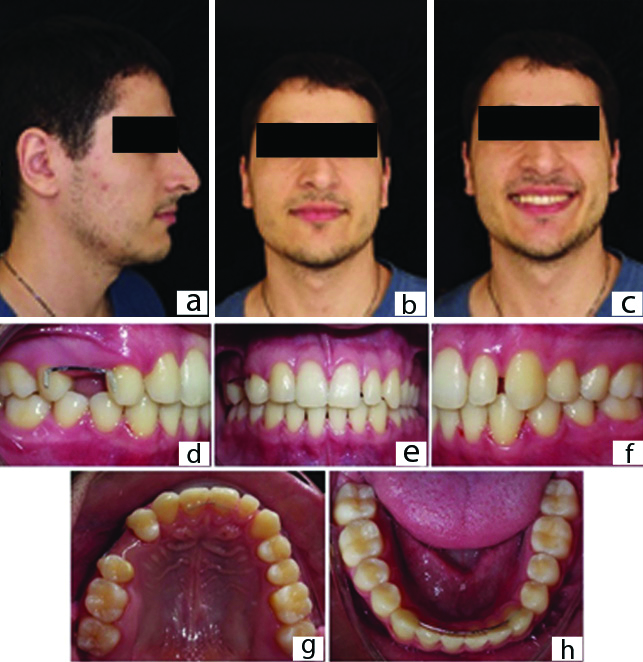
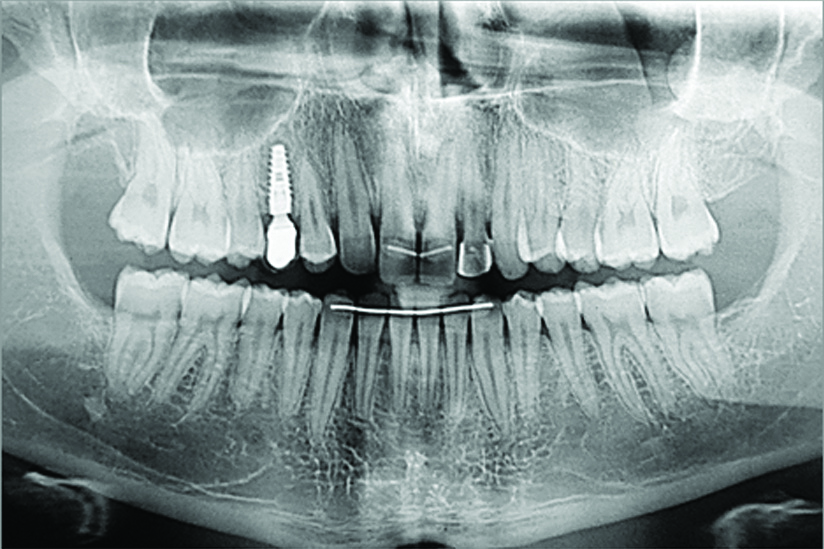
Two months after removal of the appliance, the implant was placed (Drive CM Neodent® 3.5 mm × 11.5 mm) between both premolars. The left maxillary lateral incisor was adequately reshaped in its width. Twelve months after implant and prosthesis with good occlusal intercuspation and appropriate occlusion guidance has been shown in [Table/Fig-12a-h], and the panoramic radiograph revealed a stable implant-borne crown [Table/Fig-13].
One-year follow-up intraoral photographs: a) right lateral intraoral image; b) frontal image; c) left lateral intraoral image; d) maxillary occlusal view with the prosthesis on the implant placed between the right maxillary premolars; e) Mandibular occlusal; f) canine guidance on right g) Wraparound-type maxillary retention; h) canine guidance on left.

One-year follow-up panoramic radiograph.
Discussion
In the case of a missing maxillary lateral incisor there are three treatment options that exist for replacing missing lateral incisors. They are canine substitution, a tooth-supported restoration, or a single-tooth implant. In the present clinical case the patient decided for opening the space between the maxillary first and second right premolars to position the prosthesis far from the aesthetic zone.
Besides closing all spaces to open the space for a prosthetic replacement mostly with an implant-borne crown the patient could decide to close the space completely by moving the posterior teeth with the canine substitution in place of missing lateral incisor. Another alternative was to open between both premolars in the maxillary arch [1]. In a similar case report with both missing maxillary lateral incisors, Bizetto MS et al., performed implant-prosthesis rehabilitation in place of canines, the treatment plan was facilitated because the patient chose to keep the canines in place of the missing maxillary lateral incisors [1]. The patient of the present case did not accept that option and decided for a more posterior region for implant placement, despite taking a longer time.
In the present case, the treatment time was longer than expected because the patient had to stop regular consultation for eight months for medical reasons in the family. Usually, open space requires less treatment time than closing all spaces by movement of posterior teeth mesially.
If we chose to open space in the anterior space, special care has to be taken because tooth-supported dental prostheses for maxillary lateral incisor agenesis have worse scores in the periodontal indexes than orthodontic space closure treatment [2].
The advantage of space closure is that the entire treatment is finished with the orthodontic treatment [3]. In order to replicate the replaced tooth and match it with its contralateral tooth, the mesiodistal and inciso-gingival dimensions of the canine would be reduced, also with some alterations on the labial and lingual surfaces [3].
Although the aesthetic outcomes of implant-borne crowns replacing missing maxillary lateral incisors are far more appealing than they were 10 years ago, aesthetic perceptions and preferences for this treatment modality can vary between dental professionals and laypersons [3], present case just transferred the implant/crown far from the aesthetic zone.
The dimensions of the premolar must be increased mesiodistally and incisogingivally, and the lingual cusp will need to be reduced [4], but in the present case the lingual cusp of the maxillary right premolar was not reduced because there was no interference.
On the grounds of function and dysfunction, the importance of canine-protected occlusion on lateral movement has been emphasised [5]. It is necessary to understand that fixed biomechanics can be used to control tooth movement, but it seems that safe movement does not exist, and torque is probably one of the most detrimental factors [6]. In the present case, minor torque movement was performed into the maxillary right canine and the first premolar with minor grinding of the palatal cusp.
The opening of space far from the aesthetic zone was applied in the present case report, as presented by Rosa M and Zachrisson BU, with a difference because they have opened space in between the second premolar and first molar in the case of missing maxillary lateral incisors [7].
The presence of good alveolar bone for implant rehabilitation and the absence of loss of the canine guidance [8] led to a good result in this clinical case. In addition, the patient’s cooperation, the practitioner’s skill and experience, aesthetics, and function were all important factors that affected the treatment results. These factors must always be considered in an interdisciplinary treatment approach that is beneficial for obtaining the most predictable outcomes in the case of a missing maxillary lateral incisor.
Conclusion(s)
The restoration of the prosthesis on the implant with a third premolar implant-borne crown was carried out with good dental and functional occlusion, maintenance of good aesthetics, and, mainly, gingival and healthy periodontal tissues. This clinical case can significantly contribute in similar cases with a multidisciplinary approach.
[1]. Bizetto MS, Tessarollo FR, Jimenez EE, Guariza-Filho O, Camargo ES, Tanaka OM, Implant rehabilitation of canines in case of bilaterally missing maxillary lateral incisorsAm J Orthod Dentofacial Orthop 2013 144:110-18.10.1016/j.ajodo.2012.06.02023810052 [Google Scholar] [CrossRef] [PubMed]
[2]. Tanaka OM, Pithon MM, Meira TM, Kaizer LR, Souza PHC, An atypical outcome in a case with agenesis of both mandibular central incisorsJournal of Clinical and Diagnostic Research 2019 13:01-03.10.7860/JCDR/2019/40795.12828 [Google Scholar] [CrossRef]
[3]. Silveira GS, de Almeida NV, Pereira DM, Mattos CT, Mucha JN, Prosthetic replacement vs space closure for maxillary lateral incisor agenesis: A systematic reviewAm J Orthod Dentofacial Orthop 2016 150:228-37.10.1016/j.ajodo.2016.01.01827476355 [Google Scholar] [CrossRef] [PubMed]
[4]. Schneider U, Moser L, Fornasetti M, Piattella M, Siciliani G, Esthetic evaluation of implants vs canine substitution in patients with congenitally missing maxillary lateral incisors: Are there any new insights?Am J Orthod Dentofacial Orthop 2016 150:416-24.10.1016/j.ajodo.2016.02.02527585769 [Google Scholar] [CrossRef] [PubMed]
[5]. Zachrisson BU, Rosa M, Toreskog S, Congenitally missing maxillary lateral incisors: canine substitution. PointAm J Orthod Dentofacial Orthop 2011 139:434:436:438passim10.1016/j.ajodo.2011.02.00321457853 [Google Scholar] [CrossRef] [PubMed]
[6]. Robertsson S, Mohlin B, The congenitally missing upper lateral incisor. A retrospective study of orthodontic space closure versus restorative treatmentEur J Orthod 2000 22:697-710.10.1093/ejo/22.6.69711212605 [Google Scholar] [CrossRef] [PubMed]
[7]. Rosa M, Zachrisson BU, Integrating esthetic dentistry and space closure in patients with missing maxillary lateral incisorsJ Clin Orthod 2001 35:221-34. [Google Scholar]
[8]. Babacan H, Kilic B, Bicakci A, Maxillary canine-first premolar transposition in thepermanent dentitionAngle Orthod 2008 78:954-960.10.2319/090607-419.118298217 [Google Scholar] [CrossRef] [PubMed]