Bilateral Tortuous External Iliac Artery: An Unusual Variation
Rohini Motwani1, Prajakta Kishve2, Ratna Gosain3
1 Assistant Professor, Department of Anatomy, ESIC Medical College, Saanathnagar, Hyderabad, Telangana, India.
2 Professor, Department of Anatomy, ESIC Medical College, Saanathnagar, Hyderabad, Telangana, India.
3 Senior Specialist, Department of Pathology, ESIC Medical College and Superspeciality Hospital, Saanathnagar, Hyderabad, Telangana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rohini Motwani, N14B3, Aparna Sarovar, Nallagandla, Serilingampalli, Hyderabad, Telangana, India.
E-mail: rohinimotwani@gmail.com
Bilateral tortuosity in the external iliac arteries is a rare finding in the cadavers. We report highly tortuous external iliac arteries of both the sides in a 60-year-old male cadaver noted during routine dissection. Left external iliac artery had a ‘U’ shaped loop and right external iliac artery had a ‘S’ shaped loop. The loops were found in the lesser pelvis in close relation to the obturator nerve and vessels which may get compressed by the artery. In addition the tortuous external iliac artery was also compressing the internal iliac vessels on both sides. Mild tortuosity is usually asymptomatic, moderate to severe tortuosity can lead to ischaemia of the organs or structures supplied by them or even ischaemia of the lower limb, as external iliac artery continues as femoral artery. Mild dilatation of the right common iliac artery was also present. Tortuosity of the arteries may be due to abnormal development or vascular disease, but exact mechanism is not known clearly till now. Anatomical knowledge of the tortuosity, aneurysm or kinking of iliac arteries is of utmost importance to the urologists, gynaecologists and orthopaedic surgeons so that they can correlate their findings and can take great care while doing surgeries on the pelvic region.
Bilateral variation, Iliac arteries, Loop
Case Report
The present case was observed during routine dissection of abdomen and pelvis for MBBS undergraduates in the Department of Anatomy, ESIC Medical College, Sanathnagar, Hyderabad, Telangana, India. Dissection steps were followed as per Cunningham’s manual [1]. The study has received ethical approval from Institutional ethics Committee (ESICMC/SNR/IEC-F096/04/2019).
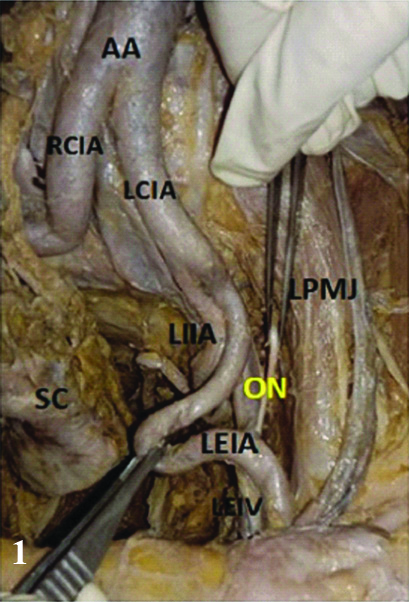
We report highly tortuous external iliac arteries of both the sides in a 60-year-old formalin embalmed male cadaver donated to the Department of Anatomy for study and research. The left external iliac artery initially was running down along the brim of the pelvis, and later descended down into the lesser pelvis to form the classical Ú’ shaped loop about 3 cm from the pelvic brim. The loop was lying superficial to the internal iliac vessels, where it may compress these vessels. After reaching the level of obturator nerve, about 3 cm from the pelvic brim, artery ascended back to the brim of the pelvis and continued as the femoral artery to the thigh behind the inguinal ligament [Table/Fig-1].
Showing course of Left External Iliac Artery (LEIA).
AA: Abdominal aorta; RCIA: Right common iliac artery; LCIA: Left common iliac artery; LEIA: Left external Iliac artery; LIIA: Left internal iliac artery; ON: Obturator nerve; LPMJ: Left psoas major muscle; SC: Sigmoid colon and its mesentery; LEIV: Left external iliac vein
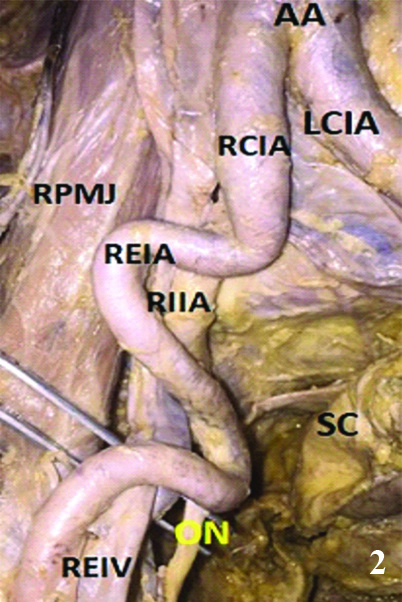
The right external iliac artery was arising as a continuation of right common iliac artery. Abdominal Aorta and Right common iliac artery showed some dilatation or aneurysm at its origin, formed a Ú’ shaped bend which entered into the lesser pelvis, giving rise to Internal Iliac Artery as a branch and went back up to the medial margin of right psoas major muscle and formed a characteristic ‘S’ shaped loop [Table/Fig-2]. This loop of the artery was found closely related to the obturator nerve and vessels. We didn’t find similar tortousity of arteries of other regions. But as such in this cadaver the connective tissue and fascia were very thickened as we can make out during the dissection in the head and neck, upper limb and lower limb regions, which we can correlate with some connective tissue disorder.
Showing course of Right External Iliac Artery (REIA).
AA: Abdominal aorta; RCIA: Right common iliac artery; LCIA: Left common iliac artery; LEIA: Left external Iliac artery; LIIA: Left internal Iliac artery; ON: Obturator nerve; RPMJ: Right psoas major muscle; SC: Sigmoid colon and its mesentery; REIV: Right external iliac vein
This type of looping of external iliac artery may be of special interest to urologists, gynaecologists and orthopaedic surgeons. The obturator nerve and vessels might might compress by the loop and can cause neurovascular symptoms. Since the loop is directly related to the inner aspect of acetabulum, it may be damaged in the surgeries of hip joint. In females, the loop might compress the fallopian tube or ovary and cause complications in transportation of ova or might get injured in the surgeries of ovary. It can also lead to reduction or lack of blood supply to the lower limbs if the artery itself get compressed by other pelvic organs.
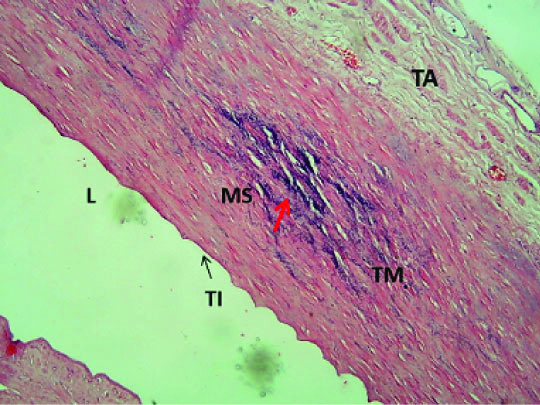
We also wanted to know if there was any histopathogical changes in the arteries, for which we took 2 cm thick sections of both the arteries and did tissue processing, followed by Haematoxylin and Eosin staining. Sections studied showed blood vessel composed of all three layers, inner tunica intima lined by flattened endothelium, thickened tunica media with foci of monckeberg’s sclerosis and unremarkable tunica adventitia [Table/Fig-3]. Monckberg’s sclerosis is seen in elderly people as a part of degeneration process.
Microphotograph of Externel iliac artery (EIA) wall with Monckeberg’s sclerosis (red arrow) in Tunica Media (TM). (Haematoxylin & Eosin stain; 40X), L: Lumen; TI: Tunica intima; TA: Tunica adventitia
Discussion
External Iliac arteries begin immediately anterior to the sacroiliac joints as the direct continuation of the common iliac arteries. Then the artery passes inferiorly and laterally in the lesser pelvis along the inlet of pelvis then it comes to lie in relation to psoas major muscle crossing it from medial to lateral side. It gives off a deep circumflex iliac artery and an inferior epigastric artery immediately superior to the inguinal ligament at the mid-inguinal point and then continues as femoral artery by passing posterior to the ligament [2].
At its origin, the external iliac artery is crossed by the ureter and the gonadal vessels, the genital branch of the genito-femoral nerve, the deep circumflex iliac vein and the vas deferens (male) or round ligament (female) of uterus. Posteriorly, it is separated from the medial border of psoas major by the iliac fascia. Laterally, it is related to psoas major, which is covered by the iliac and psoas fascia [3].
Tortuosity or looping of external iliac arteries bilaterally in the cadavers is a rare finding, as not much has been reported till now. The knowledge of the aneurysm, tortuosity, and kinking of these arteries is important for surgeons especially for planning surgeries in the hip and pelvic region. Some authors reported arterial tortuosity to be associated with ageing, atherosclerosis and hypertension, but the exact mechanism being not clear [4]. Mild tortuosity is usually asymptomatic. Severe tortuosity of the arteries can hinder the blood flow and lead to a transit ischemic attack of distal organs [5]. Clinical studies have shown that the major risk factor for tortousity of the arteries to be hypertension of the vessels [4,6].
Some authors have mentioned about Arterial Tortuosity Syndrome (ATS), which leads to elongation, tortuosity, and aneurysms of the large and middle-sized arteries. Recently, SLC2A10 gene mutations has been found to be responsible for ATS [7]. This gene decreases the function of GLUT10. This leads to overactivity (up-regulation) of TGF-β signaling by some unknown mechanism. This overactive TGF-β results in elongation of the arteries, leading to tortuosity. Overactive TGF-β signaling also interferes with normal formation of the connective tissues in other parts of the body, leading to the additional signs and symptoms of ATS [8].
The prevalence of aneurysm, tortuosity, and kinking of abdominal aorta and iliac arteries were observed in thai cadavers and the author also demonstrated 4 major variations of external iliac arteries [8]. They observed patterns of external iliac artery kinking and classified into 4 major types (S-shape; reversed -C shape; low grade shape; and V-shape). Von Hochstetter also reported a loop of external iliac artery [9], which can cause complications in total hip replacement surgeries. We observed S- shaped loop on one side and U-shaped loop of external iliac artery on other side. If the loop of the artery is too large it may lead to minor or major complications in prostatectomy. Moul JW et al., has reported a case of an abnormally large loop of external iliac artery in their case report [10]. In this case report [Table/Fig-1,2], external iliac arteries were seen compressing the internal iliac arteries bilaterally, which may lead to ischaemia of the organs supplied by the artery. Also, external iliac artery continues as femoral artery. Hence abnormality of external iliac artery may produce lower limb ischaemia.
In this case report, during the microscopic study of the artery, we observed Monckeberg’s sclerosis, where calcium deposits were found in the tunica media of the small-sized and medium-sized arteries first described by Monckeberg JG in 1903 [11]. The aetiopathogenesis remains unclear. Mediators of calcification which might be involved include abnormal smooth muscle cells of arteries with osteoblastic properties, cytokine modulators of bone mineralisation such as osteoprotegerin, Tumour Necrosis Factor (TNF)-related apoptosis-inducing ligand and receptor activator of nuclear factor kappa B ligand. This sclerosis is also found in diabetic patients related to autonomic neuropathy which suggests that autonomic dysfunction might play important role in calcification of vessel wall [12].
Assessments of the tortuosity and kinking of arteries by magnetic resonance angiography was also studied [13]. Complete anatomical knowledge of the abnormal tortuosity and kinking of the iliac arteries will be useful to decrease the complication rates or death following surgeries of aortic aneurysm [14].
Conclusion
With the present case report, we would like to bring in the notice of clinicians about this kind of bilateral tortousity of blood vessels which should be kept in mind while doing surgeries related to pelvic organs especially ovaries, ureter, prostate, seminal vesicles, or hip joint.
Author Declaration:
Financial or Other Competing Interests: No
Was informed consent obtained from the subjects involved in the study? NA
For any images presented appropriate consent has been obtained from the subjects. NA
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Sep 24, 2019
Manual Googling: Nov 20, 2019
iThenticate Software: Dec 05, 2019 (15%)
[1]. Romanes GJ, The lower limb: Cunningham’s Manual of Practical Anatomy 1986 15th edNew YorkOxford University Press:203-07. [Google Scholar]
[2]. Standring S, Borley NR, Collins P, Crossman AR, Gatzoulis MA, Healy JC, Posterior abdominal wall and retroperitoneumIn Gray’s Anatomy 2008 41st EdLondonChurchill Livingstone:1227 [Google Scholar]
[3]. Standring S, Ellis H, Healy JC, Johnson D, Williams A, Grays Anatomy 2008 40th ednNew York, USAChurchill Livingstone:1089 [Google Scholar]
[4]. Pancera P, Ribul M, Presciuttini B, Lechi A, Prevalence of carotid artery kinking in 590 consecutive subjects evaluated by echo-color Doppler. Is there a correlation with arterial hypertension?J Intern Med 2000 248:07-12.10.1046/j.1365-2796.2000.00611.x10947875 [Google Scholar] [CrossRef] [PubMed]
[5]. Cartwright MS, Hickling WH, Roach ES, Ischemic stroke in an adolescent with arterial tortuosity syndromeNeurology 2006 67:360-61.10.1212/01.wnl.0000225056.66762.f916864843 [Google Scholar] [CrossRef] [PubMed]
[6]. Hiroki M, Miyashita K, Oda M, Tortuosity ofthe white matter medullary arterioles is related to the severity of hypertensionCerebrovasc Dis 2002 13:242-50.10.1159/00005785012011548 [Google Scholar] [CrossRef] [PubMed]
[7]. Callewaert BL, Willaert A, Kerstjens-Frederikse WS, De Backer J, Devriendt K, Albrecht B, Arterial tortuosity syndrome: clinical and molecular findings in 12 newly identified familiesHum Mutat 2008 29:150-58.10.1002/humu.2062317935213 [Google Scholar] [CrossRef] [PubMed]
[8]. Wessels MW, Catsman-Berrevoets CE, Mancini GM, Breuning MH, Hoogeboom JJ, Stroink H, Three new families with arterial tortuosity syndromeAm J Med Genet A 2004 131:134-43.10.1002/ajmg.a.3027215529317 [Google Scholar] [CrossRef] [PubMed]
[9]. Von Hochstetter AH, The “lesser pelvic loop” of the external Iliac arterySurg Radiol Anat 1989 11(1):23-27.10.1007/BF021022402497529 [Google Scholar] [CrossRef] [PubMed]
[10]. Moul JW, Wind GG, Wright CR, Tortuous and aberrant External iliac artery precluding radical retropubic Prostatectomy for prostate cancerUrology 1993 42(4):450-52.10.1016/0090-4295(93)90384-M [Google Scholar] [CrossRef]
[11]. Monckeberg JG, Ueber die reine Mediaverkalkung der Extremitaetenarterien und ihr Verhalten zur ArterioskleroseVirchows Arch Pathol Anat 1903 171:141-67.10.1007/BF01926946 [Google Scholar] [CrossRef]
[12]. Gentile S, Bizzarro A, Marmo R, de Bellis A, Orlando C, Medial arterial calcification and diabetic neuropathyActa Diabetol Lat 1990 27:243-53.10.1007/BF025813362075787 [Google Scholar] [CrossRef] [PubMed]
[13]. Kristmundsson T, Sonesson B, Resch T, A novel method to estimate iliac tortuosity in evaluating EVAR accessJ Endovasc Ther 2012 19(2):157-64.10.1583/11-3704.122545879 [Google Scholar] [CrossRef] [PubMed]
[14]. Lederle FA, Wilson SE, Johnson GR, Reinke DB, Littooy FN, Acher CW, Variability in measurement of abdominal aortic aneurysms. Abdominal Aortic Aneurysm Detection and Management Veterans Administration. Cooperative Study GroupJ Vasc Surg 1995 21(6):945-52.10.1016/S0741-5214(95)70222-9 [Google Scholar] [CrossRef]