Introduction
Alcohol dependence is well known for its harmful effects and is considered as the ‘gate way’ drug of abuse across the globe. There has been a progressive increase in its abuse with a serious impact on health contributing to high morbidity and mortality.
Aim
To evaluate the extent and pattern of alcohol consumption, reasons for and factors influencing its consumption.
Materials and Methods
This was a cross-sectional study conducted in a tertiary Hospital. All in-patients admitted in psychiatry ward with diagnosis of alcohol dependence were included for the study. A pilot study was done to assess the feasibility of Case Record Form (CRF). Data collected from all alcohol dependent in-patients in psychiatry ward for a year on socio-demographic profile, patterns and types of alcohol use, the age at onset and duration of consumption/dependence along with treatment details was evaluated for in-patients reporting at a tertiary care hospital.
Results
In this cross-sectional study, 102 subjects were assessed, among them 35.30% from upper lower and middle socioeconomic category and 24.50% skilled worker group. The mean age of study population was 41.17±9.80 years with 81% in the productive age group. The mean age at onset of regular alcohol consumption was 24 years in 68.62% and 18 years in 27.45% of hospital admissions. The average number of years for first hospital admission after initiation of regular alcohol consumption was 19.92 years. The number of patients who consumed spirits was 96% and those consumed more than 3 units/day was 73.6%. The hospital admissions for alcohol related illnesses were 58.80% and those reported to seek medical help on their own was 52.9%.
Conclusion
The findings indicate that alcohol dependence is common among adolescents and young adults who are the in the productive age group. The upper lower and middle socioeconomic groups are at higher risk of dependence. There is a need for stringent policies, programs, early identification, treatment and preventive measures using age specific, feasible and efficient interventional tools to achieve ‘harm reduction’ due to alcohol dependence.
Introduction
Substance abuse presently is one of the major public and mental health problems which is on the rise throughout the world with a serious impact on the health as well as the socioeconomic status of the society. International Classification of Diseases (ICD 10) defines substance dependence as “A cluster of behavioural, cognitive, and physiological phenomena that develop after repeated substance use and that typically include a strong desire to take the substance, difficulties in controlling its use, persisting in its use despite harmful consequences, a higher priority given to drug use than to other activities and obligations, increased tolerance, and sometimes a physical withdrawal state” [1].
Among the abused substances, alcohol is considered as one of the most hazardous and harmful leading to ill health and a major risk factor contributing to high morbidity and mortality [2]. The harmful use of alcohol caused death of more than 3 million people in the year 2016, as reported by World Health Organisation (WHO). This represents 1 in 20 deaths. Overall, the harmful use of alcohol causes more than 5% of the Global Burden of Disease (GBD) [2]. Alcohol dependence is well known for its harmful effects and is considered as the ‘gate way’ drugs of abuse across the globe. It is linked to many health issues involving Neuropsychiatric disorders like withdrawal-induced seizures, Gastrointestinal diseases like liver cirrhosis, pancreatitis, alcohol-induced Cancers, Cardiovascular diseases like ischaemic heart disease, ischaemic stroke, hypertension, cardiac dysrhythmias, haemorrhagic stroke, foetal alcohol syndrome and pre-term birth complications. Tremors, convulsions, profuse sweating, anxiety, insomnia, hallucinations are some of the common clinical features associated with alcohol dependence. There has been a progressive increase in its abuse with a serious impact on health contributing to high morbidity and mortality.
GBD and injury reports a significant increase in psycho social burden like self-inflicted injuries, suicide, violence, unintentional injuries like road traffic accidents, falls, drowning, poisoning and economic loss to the community due to alcohol [3,4]. In India 4.5% of the adult men and 0.6% of women are reported to suffer from alcohol use disorders with a rapid increase in alcohol consumption [2,5]. There is a need for appropriate, simple and feasible interventional tools designed and delivered efficiently by lay therapists to target specific personality traits and high risk population in reducing problem drinking particularly among teenagers/adolescents and young adults.
For the control and management of harmful effects of alcohol consumption, designing regional based effective policies in school and social based educations, public information, advertisements, availability of alcohol and its pricing and taxing, there is a need to collect data regarding factors contributing to alcohol abuse, cost of treatment, and disease burden from alcohol abuse [6,7]. Hence this study was undertaken with the primary objective to evaluate extent and pattern of alcohol consumption, reasons for and factors influencing its consumption in Bangalore, Karnataka, India.
Materials and Methods
This cross-sectional study was conducted in a tertiary care hospital. A pilot study was conducted by division of Clinical Pharmacology at the in-patient wards of Department of Psychiatry for a month to assess the feasibility of the study and adequacy of sample size. From hospital medical record section we found that 100-120 patients were admitted each year with alcohol dependence syndrome in past three years, considering this sample size of 100 was considered for present study. This study was conducted from 1st December 2009 to 1st December 2010. The study has been approved by Institutional ethical review board with IERB Ref. number 81/2010. All patients aged more than 18 years of age admitted in psychiatry ward diagnosed as alcohol dependent by psychiatrist (According to ICD 10 criteria) [8] and consented for study were included in the study. Subjects with history of concurrent major physical or psychiatric co-morbid conditions prior to alcohol related disorders, harmful use of other substances like charas, bhang, ganja, opioids, amphetamine and their complicated withdrawal and/or patients with substance-induced psychotic disorders were excluded from the study. Total of 102 subjects were included in the study. A specially designed CRF was used to collect the data from hospital in- patients admitted at the Psychiatry wards [Annexure-1]. The data on socio-demography, age of onset of alcohol consumption, the amount, type and duration of alcohol consumption, the reason/s for consumption and persons responsible for hospital admission was collected on the day of admission to ward.
In this study any person who consumed alcohol every day was considered as regular basis of intake. Symptoms like anxiety, irritability, tremors, seizures, delirium tremens etc., which appeared after sudden discontinuation or decreased alcohol use were considered as Withdrawal symptoms.
Statistical Analysis
Data collected was entered on excel spread sheet. Baseline data was subjected to descriptive statistical analysis and was expressed as percentages. Categorical variables were compared using Chi-square (χ2) test. SPSS version 17.0 was used to analyse the data. Microsoft Word and Excel have been used to generate graphs and tables.
Results
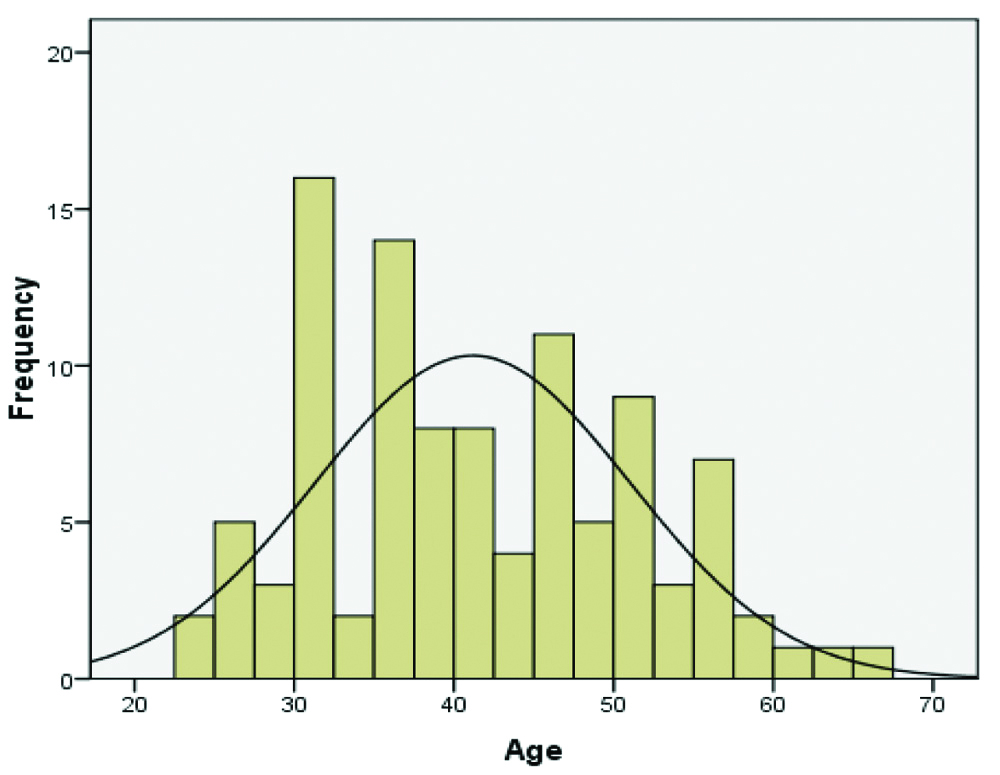
The age wise distribution of 102 patients with mean age of 41.17±9.8 years is shown in [Table/Fig-1]. There were 101 males and one female patient. Most of the subjects were from urban area (61.76%) and majority were married (90.18%). The distribution of patients based on their education, occupation and socioeconomic status with monthly income using modified Kuppuswamy classification is presented in [Table/Fig-2] [9].
Age wise distribution of study subjects. N=102.
Median=40, Mode=30 years
Socio- demographic profile of study subjects.
| Parameters | Classification | N (%) |
|---|
| Gender | Male | 101 (99.01) |
| Female | 001 (00.98) |
| Marital status | Married | 092 (90.18) |
| Unmarried | 010 (09.82) |
| Patient residence | Urban | 063 (61.76) |
| Semi-urban | 024 (23.52) |
| Rural | 015 (14.72) |
| Education | None | 005 (04.90) |
| Primary school | 018 (17.64) |
| High school | 034 (33.34) |
| PUC | 019 (18.63) |
| Degree | 025 (24.51) |
| Professional | 001 (00.98) |
| Occupation | Unemployed | 005 (04.90) |
| Unskilled worker | 017 (16.67) |
| Semiskilled worker | 015 (14.70) |
| Skilled worker | 025 (24.50) |
| Clerk, Shop/Farm owner | 020 (19.60) |
| Semi professional | 018 (17.65) |
| Professional | 002 (01.96) |
| Total income of the family per month (Used Kuppuswamy classification data) | <980 | 000 (00.00) |
| 980-2935 | 010 (09.80) |
| 2936-4893 | 021 (20.60) |
| 4894-7322 | 036 (35.30) |
| 7323-9787 | 011 (10.80) |
| 9788-19574 | 018 (17.60) |
| >17520 | 006 (05.90) |
| Socioeconomic status | Lower | 00 (00.00%) |
| Upper lower | 28 (27.50%) |
| Lower middle | 42 (41.20%) |
| Upper middle | 27 (26.50%) |
| Upper | 05 (04.90%) |
The onset of alcohol consumption on a regular basis before the age of 18 years and from 19 to 24 years was found to be 27.45% and 41.18%, respectively [Table/Fig-3]. Majority i.e., 81.37% of the current admissions was in the productive age group. The mean age at first hospital admission after the onset of regular alcohol consumption was 40.20 years. The differences related to hospital admission between the groups were not found to be statistically significant [Table/Fig-4]. The type of alcohol frequently consumed included: whisky, brandy, a combination of these followed by: rum, beer, gin, vodka, or any two of these. Majority of the patients consumed spirits (96.07%) and 73.52% consumed 4 or more units of alcohol per day [Table/Fig-5].
History of previous hospital admission for treatment with respect to their age of alcohol consumption onset.
| Prior admission for treatment | Age of onset of alcohol drinking on regular basis |
|---|
| ≤18 Years | 19-24 Years | 25-29 Years | ≥30 Years | Total |
|---|
| No | Mean age | No | Mean age | No | Mean age | No | Mean age | No |
|---|
| No | 17 | 16.70 | 27 | 20.51 | 06 | 26.33 | 11 | 34.72 | 61 |
| Yes | 11 | 16.63 | 15 | 20.66 | 08 | 26.62 | 07 | 32.71 | 41 |
| Total | 28 | 16.67 | 42 | 20.57 | 14 | 26.5 | 18 | 33.94 | 102 |
Patients age during present admission with respect to their age of onset of alcohol consumption on regular basis.
| Age of patients during present admission | Age of onset of alcohol drinking on regular basis |
|---|
| ≤18 years | 19-24 years | 25-29 years | ≥30 years | Total |
|---|
| 18-30 years, n=15(14.7%) | 7 (6.86%) | 6(5.88%) | 2(1.96%) | 0(0%) | 15 |
| 31-40 years,n=39 (38.23%) | 14(13.73%) | 16(15.68%) | 8(7.84%) | 1(0.98%) | 39 |
| 41-50 years,n=29 (28.43%) | 3(2.94%) | 15(14.70%) | 3(2.94%) | 8(7.84%) | 29 |
| 51-60 years,n=16 (15.7%) | 4(3.92%) | 3(2.94%) | 1(0.98%) | 8(7.84%) | 16 |
| 261 years,n=3 (2.9%) | 0(0%) | 2(1.96%) | 0(0 %) | 1(0.98%) | 03 |
Type and units of alcohol consumed by alcohol dependent patients.
| Type of alcohol consumed | Number of patients | Percentage (%) |
|---|
| Brandy | 19 | 18.6 |
| Brandy, Whisky | 08 | 07.8 |
| Whisky | 53 | 52.0 |
| Rum | 07 | 06.9 |
| Gin | 02 | 02.0 |
| Beer | 04 | 03.9 |
| Vodka | 02 | 02.0 |
| 2 or more brand | 07 | 06.8 |
| Total | 102 | 100 |
| Number of units of alcohol consumed | Number of patients | Percentage (%) |
| 2-3 units/day | 27 | 26.4 |
| 4-5 units/day | 43 | 42.2 |
| 6-7 units/day | 32 | 31.4 |
| Total | 102 | 100 |
1 unit=10 mL of pure alcohol
The reasons for seeking admission to hospital by most of alcohol dependent patients i.e., 58.80% was related to illnesses due to alcohol consumption, followed by the guilt feeling among 19.6%. The family problems, financial and job problems and social outcast together constituted 11.8% admissions. Majority of patients, 52.9% reported to hospital on their own for medical assistance, and 37.3% influenced by their family members and the remaining as referrals by other physicians, friends and employer [Table/Fig-6].
Data on reason for hospital admission of alcohol dependent patients.
| Sl. No. | Reasons for admission | No. of patients | Percentage |
|---|
| 1 | Physical ill health | 60 | 58.8 |
| 2 | Withdrawal symptoms | 10 | 09.8 |
| 3 | Social outcast | 02 | 02.0 |
| 4 | Financial problem | 04 | 03.9 |
| 5 | Family responsibility | 05 | 04.9 |
| 6 | Guilt | 20 | 19.6 |
| 7 | Job problem | 01 | 01.0 |
| Total | 102 | 100 |
| Sl. No. | Person responsible for referring patients to hospital | No. of patients | Percentage |
| 1 | Self | 54 | 52.9 |
| 2 | Family | 38 | 37.3 |
| 3 | Employer | 01 | 01.0 |
| 4 | Friends | 03 | 02.9 |
| 5 | Physician | 05 | 04.9 |
| 6 | Previous alcohol dependent patient | 01 | 01.0 |
| Total | 102 | 100 |
There were 40.20% patients with previous history of hospital admission for the management of alcohol dependence or alcohol related health problems and of these 30.39% received one of the three FDA approved anti-craving medications namely disulfiram, naltrexone and acamprosate for relapse prevention. The baseline characteristics of relapsed, readmitted patients were comparable to that of patients who were admitted for the first time 59.80% for the management of alcohol dependence. The data was published before as Lohit K et al., [10].
Discussion
The per capita alcohol consumption and the prevalence of alcohol related disorders including dependence are reported to be on the rise in India despite the strong efforts by the national government to reduce alcoholism [2]. It is estimated that there are 4.5% adult men suffering from alcohol related disorders/problems which account for more than a fifth of hospital admissions; 18% of psychiatric emergencies; more than 20% of all brain injuries and 60% of all injuries reporting to India’s emergency rooms [11].
In the present study the age of onset of alcohol consumption on a regular basis was found to be between 15-18 years (the correct age below 18 could not be ascertained) with the mean age around 16 years in more than quarter of the patients and less than 24 year age in 68% of patients which is similar to the study conducted in Mangalore by D’Souza PC and Mathai PJ, Canada by DeWit DJ et al., and Sartor CE et al., [12-14]. However, study from Assam and Punjab by Mahanta B et al., and Khosla V et al., respectively states very early onset of alcohol consumption before 14 years [15,16]. This difference in the finding may be attributed to a region and also difference in the study sample compared to our study.
The permissible age for drinking alcohol in India varies from 18 years to 25 years from state to state. In Karnataka the legal age for drinking alcohol is 18 years according to The Karnataka Excise Act, 1965 Section 36 [17]. It is important to note that despite this law, many of the adolescents are reported to consume alcohol even before 18 years of age as seen in the present study and the age of initiation of consumption on a regular basis was 18 to 24 years in 68.63% of patients and the remaining consumed alcohol beyond this age.
The existing Section 32, relevant to health permits of THE KARNATAKA PROHIBITION ACT, 1961 suggests, the State Government, or subject to its control, the Deputy Commissioner (DC), may grant a health permit for the use or consumption of liquor to any person who requires such liquor for the preservation or maintenance of his health, provided that no such permit shall be granted to a minor and such permits shall be granted for such quantity and shall be subject to further conditions as may be prescribed [18]. Even the section 13 of Bombay Prohibition Act 1949, states that “no person shall consume or use liquor and section 22A states that no person other than a Registered Medical Practitioner (RMP) shall issue any prescription for any intoxicating liquor unless he believes in good faith after careful medical examination of the person for whose use such prescription is sought, that the use of such intoxicating liquor by such person is necessary and will afford relief to him from some known ailment” [19]. Therefore, without prescription by a RMP or permission from the concerned authority no person can get alcohol/liquor. Despite existence of such laws the prevalence of alcohol consumption has increased during recent years which suggest failure in implementing the law. According to article 47 of the Constitution of India, prohibition is included among the directive principles of state policy which states “The State shall endeavour to bring about Prohibition of the use (of Alcohol) except for medicinal purposes of intoxicating drinks and of drugs which are injurious to health [20].” In the present study none of the patients gave history of ill health before consumption of alcohol and none were prescribed alcohol for medicinal purpose, this shows that the implementation of the article 47 appears to have failed. However, prohibition of liquor/alcohol is in force in few states of India [17].
The male preponderance of alcohol dependence is seen in our study which can be explained by prevalent socio cultural and religious factors across India [12,21,22]. However, this finding may need further confirmation since the possibility exists that females may not reveal due to fear of social outcast. Majority of the male patients were married (90.18%) and living with respective partners. However, it was not possible to ascertain adverse impact of alcohol dependence on the family such as domestic violence, psychosocial disturbances and increasing economic burden which are well known [5]. However, in the present study this data was not collected since patients were reluctant to reveal personal history and the same may be considered as a limitation. The finding that maximum numbers of patients were from urban and semi urban areas can be justified by the fact that study centre is a tertiary care hospital located centrally in an urban area and caters to patients around this. The socioeconomic status of our study subjects showed majority belonged to upper lower and middle classes which were similar to the study carried out by D’Souza PC and Mathai PJ, and by Benegal V et al., with 45% rural study participants [12,23]. This similarity can be explained as the study was conducted in a similar geographic location [24]. The low standards of living are said to be associated with adolescent onset drinking. The duration of regular alcohol consumption was nearly 20 years and the mean age at admission was 40 years. The fact that the adolescent and late adolescent group is representative of major part of India belonging to lower middle income category and this may be considered to contribute significantly to economic burden and to adversely influence the socioeconomic status [2,24]. The findings of the present follow-up study of three months also support that alcohol dependence is a major contributor of co-morbidities and therefore a reason for patients to be hospitalised for treatment. This latter finding may be considered to add to the economic burden and significantly affect quality of life. However, study needs to be carried out in a larger population.
While, majority of the alcohol dependent patients were seen to report on their own for treatment due to ill health a limited numbers were referred for consultation by family members. The findings in D’Souza PC and Mathai PJ, showed that majority was referred by family and then followed by self interest by the patients [12]. The differences may be due to the changes in the primary objective of the study. In both the studies only a few were referred either by their friends or employer or by patients with previous history of alcohol dependence. This finding appears to signify the least positive societal attitude to lend support in preventing alcohol consumption.
The baseline characteristics of patients who were admitted for the first time for management of alcohol dependence were comparable to that of patients who were re-admitted for the management of alcohol dependence and its ill effects [10]. Therefore, it may be hypothesised that there are increasing chances of relapse in alcohol dependence among this group of patients even after the complete treatment.
There are laws that exist to prevent drunkenness which are expected to help in harm reduction. According to section 76, “penalty for being drunk and for disorderly behaviour of the Karnataka prohibition act 1961, whoever in any street or thoroughfare or public place or in any place to which the public have or are permitted to have access is drunk and is incapable of taking care of himself, or behaves in a disorderly manner under the influence of drink, shall, on conviction, be punished unless the contrary is proved that the person accused of the said offence has drunk liquor or consumed any other intoxicant for the purpose of being intoxicated and not for a medicinal purpose” [18]. Further the observations of the present study shows that 96% of patients consumed >3 units per day support the rising trend in consumption of spirits over the years which is similar to that reported by WHO in 2011 (88%) and 2014 (93%) [2,21]. This suggests that even with the existence of strict laws the harmful use of alcohol is increasing with lack of support from the community.
Although, Indian National government is encouraging to reduce/stop alcoholism the report by Prasad R mentions that there have been hurdles like- low priority given to treatment of alcoholism, lack of access to pharmacological care, poor funding to support and encourage adequate training of appropriate health care professionals as well as failure to motivate them to work in this field [25].
A study by Steven D concludes that offering group therapy aimed at personality traits such as high-risk teenagers may influence significantly in halting progress to more risky drinking in this group of individuals [26]. In addition it has a potential for extension as a halo effect to low-risk students in schools to whom group therapy is offered. This approach is suggested as an early example of personalised prevention in psychiatry. Interestingly this modality appears appropriate, feasible and useful as a supplement to primary medication treatment which can be adopted in a resource poor country like India.
Limitation
As this was a hospital based study not all alcohol dependent cases were assessed and factors responsible for dependence also differs, need to conduct community based study to assess factors responsible for dependence.
Conclusion
There is an increase in alcohol dependence and early onset of use of alcohol on regular basis there is a need for implementation of robust national level policies laws and acts to change the societal attitude to prevent alcoholism and support from public towards social welfare.
Recommendations
To identify nationwide suitable strategies and models to offer appropriate training, making available safer anti-craving treatment options and preventive measures for alcohol dependence among most productive age group in order to reduce the economic burden to the society as well as in achieving significant harm reduction.
1 unit=10 mL of pure alcohol
[1]. The ICD-10 Classification of Mental and Behavioural Disorders. Clinical descriptions and diagnostic guidelines. Geneva, World Health Organization, 1992 [Google Scholar]
[2]. Global status report on Alcohol and health 2018. ISBN 978 92 4 156415 1. (NLM classification: WM 274) © World Health Organization 2018 [Google Scholar]
[3]. Parry CD, Patra J, Rehm J, Alcohol consumption and non-communicable diseases: Epidemiology and policy implicationsAddiction 2011 106(10):1718-24.10.1111/j.1360-0443.2011.03605.x21819471 [Google Scholar] [CrossRef] [PubMed]
[4]. Rehm J, Mathers C, Popova S, Thavorncharoensap M, Teerawattananon Y, Patra J, Alcohol and global health 1: Global burden of disease and injury and economic cost attributable to alcohol use and alcohol use disordersLancet 2009 373:2223-33.10.1016/S0140-6736(09)60746-7 [Google Scholar] [CrossRef]
[5]. Rehm J, Kanteres F, Lachenmeier DW, Unrecorded consumption, quality of alcohol and health consequencesDrug and Alcohol Review 2010 29:426-36.10.1111/j.1465-3362.2009.00140.x20636660 [Google Scholar] [CrossRef] [PubMed]
[6]. Anderson P, Chisholm D, Fuhr D, Effectiveness and cost-effectiveness of policies and programmes to reduce the harm caused by alcoholLancet 2009 373:2234-46.10.1016/S0140-6736(09)60744-3 [Google Scholar] [CrossRef]
[7]. Technical brief of burden and socio economic cost attributable to alcohol use in India. Geneva, World health Organization. Available from : http://www.searo.who.int/india/publications/assessment_burden_socioeconomic_cost.pdf (Accessed on 19/07/2019) [Google Scholar]
[8]. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical descriptions and diagnostic guidelines. Available from : https://www.who.int/substance_abuse/terminology/ICD10ClinicalDiagnosis.pdf?ua=1. (Accessed on 29/11/2019) [Google Scholar]
[9]. Kumar N, Shekhar C, Kumar P, Kundu AS, Kuppuswamy’s socioeconomic status scale-updating for 2007Indian J Pediatr 2007 74(12):1131-32. [Google Scholar]
[10]. Lohit K, Kulkarni C, Galgali RB, Factors influencing adherence to anti-craving medications and drinking outcomes in patients with alcohol dependence: A hospital-based studyJ Pharmacol Pharmacother 2016 7:72-79.10.4103/0976-500X.18477027440951 [Google Scholar] [CrossRef] [PubMed]
[11]. Swendsen J, Burstein M, Case B, Conway KP, Dierker L, He J, Use and abuse of alcohol and illicit drugs in US adolescents: Results of the national comorbidity survey-adolescent supplementArchives of General Psychiatry 2012 69(4):390-98.10.1001/archgenpsychiatry.2011.150322474107 [Google Scholar] [CrossRef] [PubMed]
[12]. D’Souza PC, Mathai PJ, Motivation to change and factors influencing motivation in alcohol dependence syndrome in a tertiary care hospitalIndian J Psychiatry 2017 59:183-88.10.4103/psychiatry.IndianJPsychiatry_262_1528827865 [Google Scholar] [CrossRef] [PubMed]
[13]. DeWit DJ, Adlaf EM, Offord DR, Ogborne AC, Age at first alcohol use: A risk factor for the development of alcohol disordersAmerican Journal of Psychiatry 2000 157(5):745-50.10.1176/appi.ajp.157.5.74510784467 [Google Scholar] [CrossRef] [PubMed]
[14]. Sartor CE, Lynskey MT, Heath AC, Jacob T, True W, The role of childhood risk factors in initiation of alcohol use and progression to alcohol dependenceAddiction 2007 102(2):216-25.10.1111/j.1360-0443.2006.01661.x17222275 [Google Scholar] [CrossRef] [PubMed]
[15]. Mahanta B, Mohapatra PK, Phukan N, Mahanta J, Alcohol use among school-going adolescent boys and girls in an industrial town of Assam, IndiaIndian J Psychiatry 2016 58(2):157-63.10.4103/0019-5545.18378427385848 [Google Scholar] [CrossRef] [PubMed]
[16]. Khosla V, Thankappan KR, Mini GK, Sarma PS, Prevalence and predictors of alcohol use among college students in Ludhiana, Punjab, IndiaIndian J Med Res 2008 128:79-81. [Google Scholar]
[17]. The Karnataka Excise Act, 1965. Act 21 of 1966: Available from http://www.lawsofindia.org/pdf/karnataka/1966/1966KR21.pdf accessed on 11/102/2019) [Google Scholar]
[18]. Karnataka prohibition act 1961: Available from: http://dpal.kar.nic.in/pdf_files/17%20of%201962%20(E).pdf (accessed on 11/10/2019) [Google Scholar]
[19]. Bombay prohibition Act, 1949. Maharastra section 13. Available from https://indiacode.nic.in/bitstream/123456789/6407/1/prohibition_act.pdf (accessed on 11/10/2019) [Google Scholar]
[20]. The constitution of India Article 47.1949. Available from http://www.indianconstitution.in/2016/05/article-47-constitution-of-india.html (accessed on 01/02/2017) [Google Scholar]
[21]. Global status report on alcohol and health. ISBN 978 92 4 156415 1. (NLM classification: WM 274) © World Health Organization 2011 [Google Scholar]
[22]. Ray R, Mondal AB, Gupta K, Chatterjee A, Bajaj P, The extent pattern and trends of drug abuse in India: National Survey 2004 New DelhiUnited Nations office on drugs and crimes and ministry of social justice and empowerment, Government of India [Google Scholar]
[23]. Benegal V, Velayudhan A, Jain S, Social costs of Alcoholism: A Karnataka perspectiveNIMHANS Journal 2000 18(1&2):67 [Google Scholar]
[24]. Pillai A, Nayak MB, Greenfield TK, Bond JC, Hasin DS, Patel V, Adolescent drinking onset and its adult consequences among men: a population based study from IndiaJournal of Epidemiology and Community Health 2014 68(10):922-27.10.1136/jech-2014-20405825096808 [Google Scholar] [CrossRef] [PubMed]
[25]. Prasad R, Alcohol use on the rise in IndiaLancet 2009 373(9657):17-18.10.1016/S0140-6736(08)61939-X [Google Scholar] [CrossRef]
[26]. Steven D, A personalized approach to prevention of risky drinkingJAMA Psychiatry 2013 70:33410.1001/jamapsychiatry.2013.1989 [Google Scholar] [CrossRef]